Article Text

Abstract
Introduction The molecular mechanisms of syndesmophyte formation in ankylosing spondylitis (AS) are yet to be characterised. Molecules involved in bone formation such as Wnt proteins and their antagonists probably drive syndesmophyte formation in AS.
Methods This study investigated sequential serum levels of functional dickkopf-1 (Dkk1), a potent Wnt antagonist involved in bone formation in arthritis, by capture ELISA with its receptor LRP6 in 65 AS patients from the German Spondyloarthritis Inception Cohort. Dkk1 levels were then related to structural progression (syndesmophyte formation) as well as sclerostin and C-reactive protein (CRP) levels.
Results Functional Dkk1 levels were significantly (p=0.025) higher in patients with no syndesmophyte growth (6.78±5.48 pg/ml) compared with those with syndesmophyte growth (4.13±2.10 pg/ml). Dkk1 levels were highly correlated to serum sclerostin levels (r=0.71, 95% CI 0.53 to 0.82; p<0.001) but not to CRP (r=0.15, 95% CI −0.10 to 0.38; p=0.23).
Conclusion AS patients with no syndesmophyte formation show significantly higher functional Dkk1 levels suggesting that blunted Wnt signalling suppresses new bone formation and consequently syndesmophyte growth and spinal ankylosis. Similar to serum sclerostin levels, the functional Dkk1 level thus emerges as a potential biomarker for structural progression in patients with AS
Statistics from Altmetric.com
Ankylosing spondylitis (AS) is characterised by bone marrow inflammation leading to apposition of bone along periosteal sites.1 2 Bony spurs (syndesmophytes) contribute to the signs and symptoms of AS and are considered to precipitate functional decline. Current cytokine blocking strategies do not overcome new bone formation, suggesting that molecular processes eliciting syndesmophyte formation differ from the inflammatory processes in AS.3 The differentiation of mesenchymal cells into bone-forming osteoblasts appears to be a key pathogenic event for syndesmophyte formation. Wnt proteins, which govern the differentiation of osteoblasts, have recently been identified as contributing to new bone formation in inflammatory arthritis. Therefore, fostering of the Wnt signalling pathway by blocking its natural inhibitor dickkopf-1 (Dkk1) leads to the excessive growth of peripheral osteophytes as well as fusion of the sacroiliic joints.4 5 These observations suggested that Wnt signalling is of key importance in osteophyte formation and that Wnt activity may represent a biomarker for ankylosis.6 In support of this concept, low serum levels of the Wnt inhibitor sclerostin are predictive of progressive syndesmophyte formation in AS patients.7 Moreover, high serum levels of sclerostin as well as Dkk1 are linked to erosive bone diseases, such as rheumatoid arthritis or multiple myeloma.4 8 Interestingly, very recent investigations suggest that sclerostin and Dkk1 appear to be tightly linked, as Dkk1 induces sclerostin expression.9 Here we correlate the Dkk1 levels measured over 2 years in patients with AS with the growth of syndesmophytes in the same patients over the same time period.
Materials and methods
Patients
Patients were those participating in the recently described German Spondyloarthritis Inception Cohort (GESPIC)10 on patients with AS according to the modified New York criteria and symptom duration of less than 10 years. Serum at baseline, year 1 and year 2 and radiographs from the spine at baseline and year 2 were available from 65 AS patients. None of the patients was treated with tumour necrosis factor (TNF) blockers. Patient characteristics were as follows: mean age (SD): 35.2 years (10.4); duration of symptoms 5.9 years (2.7), 46 out of 65 (70.8%) were men, 60 out of 65 (92.3%) were human leucocyte antigen (HLA) B27 positive, mean Bath ankylosing spondylitis disease activity index 3.7 (1.9), mean Bath ankylosing spondylitis functional index 3.1 (2.3).
Scoring of radiographs
Radiographs of the lumbar and cervical spine were scored by three readers blinded for time points using the modified Stokes ankylosing spondylitis spinal score (mSASSS), as previously described.7 11 Patients were divided into different groups depending on whether there were syndesmophytes present at baseline or not and whether there was a growth of syndesmophytes, defined by an increase of the mSASSS score from 0 or 1 to 2 or 3. An increase in the mSASSS score from 0 to 1 was not counted because it reflects erosive/sclerotic changes but not syndesmophyte growth. Moreover, new formation or growth of syndesmophytes was only counted if observed by at least two out of three readers. Similarly, no growth of syndesmophytes was only counted if there was agreement among the readers.
Measurement of Dkk1 serum levels
Functional serum Dkk1 levels were measured by plate-bound human LRP-6 (1 mg/ml) (R&D, Wiesbaden, Germany) and detected by biotinylated antihuman Dkk1 immunoglobulin (R&D) as previously described.4 Total Dkk1 levels were assessed by commercial sandwich ELISA (Biomedica, Vienna, Austria).
Statistical analyses
Statistical comparisons were made between the groups with a non-ambiguous defined status of syndesmophyte presence or syndesmophyte growth. To compare Dkk1 levels assessed at three points in time between groups a non-parametric variance analysis of longitudinal data (as proposed by Brunner et al)12 was applied. Two-way non-parametric variance analyses included as outcome Dkk1 levels and as factors time points as one factor and syndesmophyte formation (or syndesmophyte presence) yes/no as another factor. Furthermore, in multiway variance analyses risk factors of radiographic progression were included in addition. Spearman's rank correlation coefficient was used to calculate the association between Dkk1 levels and those of sclerostin or C-reactive protein (CRP). The Kruskal–Wallis test was applied for univariate comparisons at baseline as well as for the comparison of the mean functional Dkk1 levels per patient between groups. Of note, this last comparison of mean Dkk1 levels per patient excludes some additional information available by the single Dkk1 values and therefore has a lower power than the variance analytical approach proposed by Brunner et al.12
Results
Dkk1 level and baseline syndesmophyte status
According to the definition given in the Methods section, no syndesmophytes were present in 31 patients at baseline, whereas syndesmophytes were present in 23 patients. In 11 patients there was no agreement among the scorers. The mean Dkk1 level at baseline was higher (7.55±6.26 pg/ml) in patients without syndesmophytes compared with those with syndesmophytes (4.68±4.38 pg/ml), although this difference did not reach statistical significance (p=0.09). The mean total Dkk1 levels were not different between patients with compared to those without syndesmophytes at baseline. When assessing total Dkk1 levels, no significant difference (p=0.92) was found between patients with (2019±988 pg/ml) compared to those without (2067±1036 pg/ml) syndesmophytes at baseline.
Dkk1 level and progression of syndesmophytes
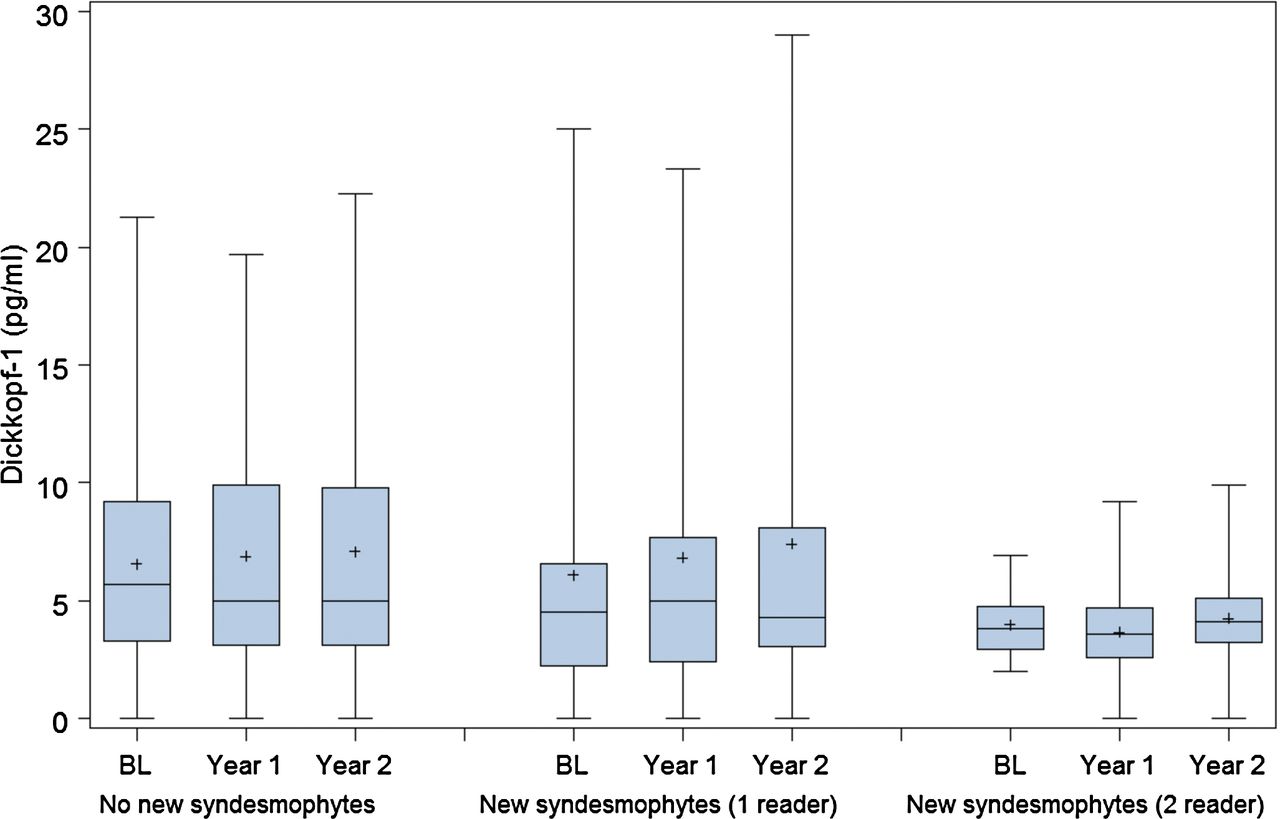
No growth of syndesmophytes over 2 years was observed in 37 patients, while in 12 patients new formation or growth of syndesmophytes was seen. In the other 16 patients growth of syndesmophytes was scored by only one reader. The Dkk1 level was significantly higher (p=0.025) in patients with no syndesmophyte growth (6.78±5.48 pg/ml) compared with those patients with syndesmophyte growth detected by two readers (4.13±2.10 pg/ml) (figure 1). This difference remained significant (p=0.002) when controlled for risk factors of syndesmophyte growth (presence/absence of syndesmophytes at baseline, CRP status, continuous/non-continuous treatment with non-steroidal anti-inflammatory drugs, gender, disease duration and HLA-B27 status) by multifactorial non-parametric variance analysis (Brunner test). Furthermore, considering the mean of the three Dkk1 levels per patient higher levels of functional Dkk1 (over 10 pg/ml) are exclusively found in patients with no new syndesmophyte formation (see probability plot figure 2, comparison between both groups p=0.08). Again, no significant difference between AS patients progressing in ankylosis (2481.2±1409 pg/ml) and those with no progression (2052.0±1278 pg/ml) was found, when total Dkk1 levels were measured.

Progression in syndesmophytes and serum level of dickkopf-1 (Dkk1). Serum analysis for Dkk1 levels at baseline (BL) and after 1 and 2 years. Patient group at the left (N=37) indicates those with no progression of syndesmophytes. Patients in the middle show questionable progression, only one out of three readers scored progression (N=16); and patients at the right show clear progression, with two or three readers agreeing on new syndesmophytes (N=12). Boxes show the range between the lower and upper quartile, horizontal lines within the boxes indicate the medians and the plus sign indicates the means. Dkk1 levels were significantly lower in the group of patients with no progression compared with those with syndesmophyte growth (p=0.025), while the difference of any of these two groups compared to the middle group was not significant.

Cumulative distribution of dickkopf-1 (Dkk1) serum levels in two groups of patients. The mean values of three sequential Dkk1 measurements per patient are shown. Circles: patients who did not develop new syndesmophytes according to the readers; triangle: patients with syndesmophyte growth according to two or three readers.
Dkk1 level and correlation to sclerostin and CRP levels
Dkk1 serum levels were highly correlated between the different time points: baseline versus year 1: r=0.91, 95% CI 0.85 to 0.94; year 1 versus year 2: r=0.90, 95% CI 0.83 to 0.94; baseline versus year 2: r=0.84, 95% CI 0.75 to 0.90. When Dkk1 serum levels were compared with the serum level of another Wnt antagonist, sclerostin, which has recently been associated with syndesmophyte formation,7 a high correlation between Dkk1 and sclerostin was found (r=0.71, 95% CI 0.53 to 0.82; p<0.001; figure 3). Interestingly, there was no correlation between Dkk1 and CRP levels (r=0.15, 95% CI −0.10 to 0.38; p=0.23).

{kind=link}
{kind=link}
{kind=link}
Correlation of dickkopf-1 (Dkk1) and sclerostin serum levels. X-axis indicates sclerostin serum level; y-axis indicates Dkk1 level in ankylosing spondylitis patients r=0.71 (p<0.001).
Discussion
Here we show that high serum level of functional Dkk1 binding to its receptor LRP-6 is associated with the lack of syndesmophyte formation in AS patients. These data provide translational evidence that active Wnt signalling may support syndesmophyte formation in AS. Evidence for this concept comes from experimental data showing that: (1) Dkk1 blockade leads to enhanced bone formation and ankylosis of peripheral joints;4 (2) axial joint ankylosis is elicited by Dkk1 blockade;5 (3) other Wnt antagonists such as sclerostin are associated with syndesmophyte formation;7 and (4) Wnt agonists such as R-spondin induce bone spur formation along inflamed joints.9 13 Therefore, and as the expression of Dkk1 is tightly linked to sclerostin expression, we considered Dkk1 as a potential marker for the progression of syndesmophyte formation in AS.
The fact that serum Dkk1 levels are associated with the number of pre-existing syndesmophytes and growth of new syndesmophytes suggests that high Wnt activity lacking the appropriate balance by Wnt antagonists is a crucial trigger for spinal ankylosis in patients with AS. Conflicting data on Dkk1 serum levels in AS have been reported. One study showed elevated circulating Dkk1 serum level in AS patients, but the binding of Dkk1 and its cellular effects were impaired,14 whereas our group showed that functional Dkk1 levels are lower in AS than in patients with rheumatoid arthritis.4 In fact, these at first sight diverging observations are in accordance, given that the authors using the protein assay for Dkk1 measuring total Dkk1 showed that Dkk1 might be dysfunctional in AS patients. Our assay only measures receptor-bound and thus functional Dkk1, which reflects the net effect of all Wnt proteins and their antagonist in the serum. As a consequence functional Dkk1 levels are lower than when measuring total Dkk1 protein in the serum.4 Our data are also in accordance with previous data on sclerostin levels, which showed that low sclerostin levels are linked to the progression of syndesmophytes in AS, and in fact our data showed a good correlation between Dkk1 and sclerostin levels.5
In contrast, no correlation between Dkk1 and CRP was found indicating that expression of this Wnt antagonist is not linked to acute phase responses. No association of a decrease of CRP levels with a change in the Dkk1 levels was also reported recently in AS patients treated with TNF blockers.14 These findings support previous notions in experimental animal models of AS and patients with AS that inflammation may not be tightly linked to bone responses.2 15 16 Anti-inflammatory therapy with TNF inhibitors does not affect syndesmophyte formation, but strongly suppresses the synthesis of CRP leading to a rapid decrease in serum levels. We do not know, however, whether other anti-inflammatory or anti-cytokine treatments behave similarly.
Another interesting finding was the stability of Dkk1 levels between the three time points covering a 2-year interval. In the present study we investigated only patients without TNF blocker therapy, but along the same line, no change in the functional Dkk1 was found before and after treatment of AS patients with TNF blockers in another report.14 Our data need further validation. Because of the limited number of patients we were not able to control for all possible confounders by means of a multivariate analysis. Future research has to clarify whether there are low and high Dkk1 producers among AS patients, whether this production is controlled genetically or by other mechanisms, and whether Dkk1 levels, or other Wnt inhibitors can be used to predict fast progression of new bone formation.
References
Footnotes
-
Funding This study was supported by the Deutsche Forschungsgemeinschaft (SPP1468-IMMUNOBONE), the Bundesministerium für Bildung und Forschung (BMBF; projects ANCYLOSS and Competence Network Rheumatology), the MASTERSWITCH and BTCure projects of the European Union, the Interdisciplinary Centre for Clinical Research and the ELAN fund of the University of Erlangen-Nuremberg.
-
Competing interests None.
-
Ethics approval The GESPIC study was approved by the medical ethics committees of all participating centres.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.