Article Text

Abstract
Background Anti-citrullinated protein antibodies (ACPA) are a marker of RA, and the presence of the immunoglobulin M (IgM) isotype indicates an ongoing immune response involving the recruitment of naïve B cells.1 Abatacept (ABA) modulates T-cell co-stimulation and has been shown to impact ACPA maturation, including seroconversion of IgM, in the AVERT (Assessing Very Early Rheumatoid arthritis Treatment) trial.2
Objectives To assess the efficacy of treatment with ABA+MTX, ABA monotherapy or MTX alone in patients (pts) from the AVERT trial based on their anti-cyclic citrullinated peptide 2 (CCP2; a surrogate for ACPA) IgM serostatus at baseline (BL), and seroconversion (anti-CCP2 IgM positive to negative) through 1 year.
Methods The AVERT trial has been described previously.3 In this post hoc analysis, pt samples were analysed by ELISA to determine anti-CCP2 IgM serostatus. Efficacy outcomes analysed by BL anti-CCP2 IgM serostatus included remission rate at 12 mths (CDAI, SDAI, Boolean and DAS28 [CRP] <2.6-defined remission), and adjusted mean change in DAS28 (CRP) and HAQ-DI over time (samples taken every 28 days up to Mth 12 and analysed with a longitudinal repeated-measures model). Boolean remission was analysed in pts who seroconverted.
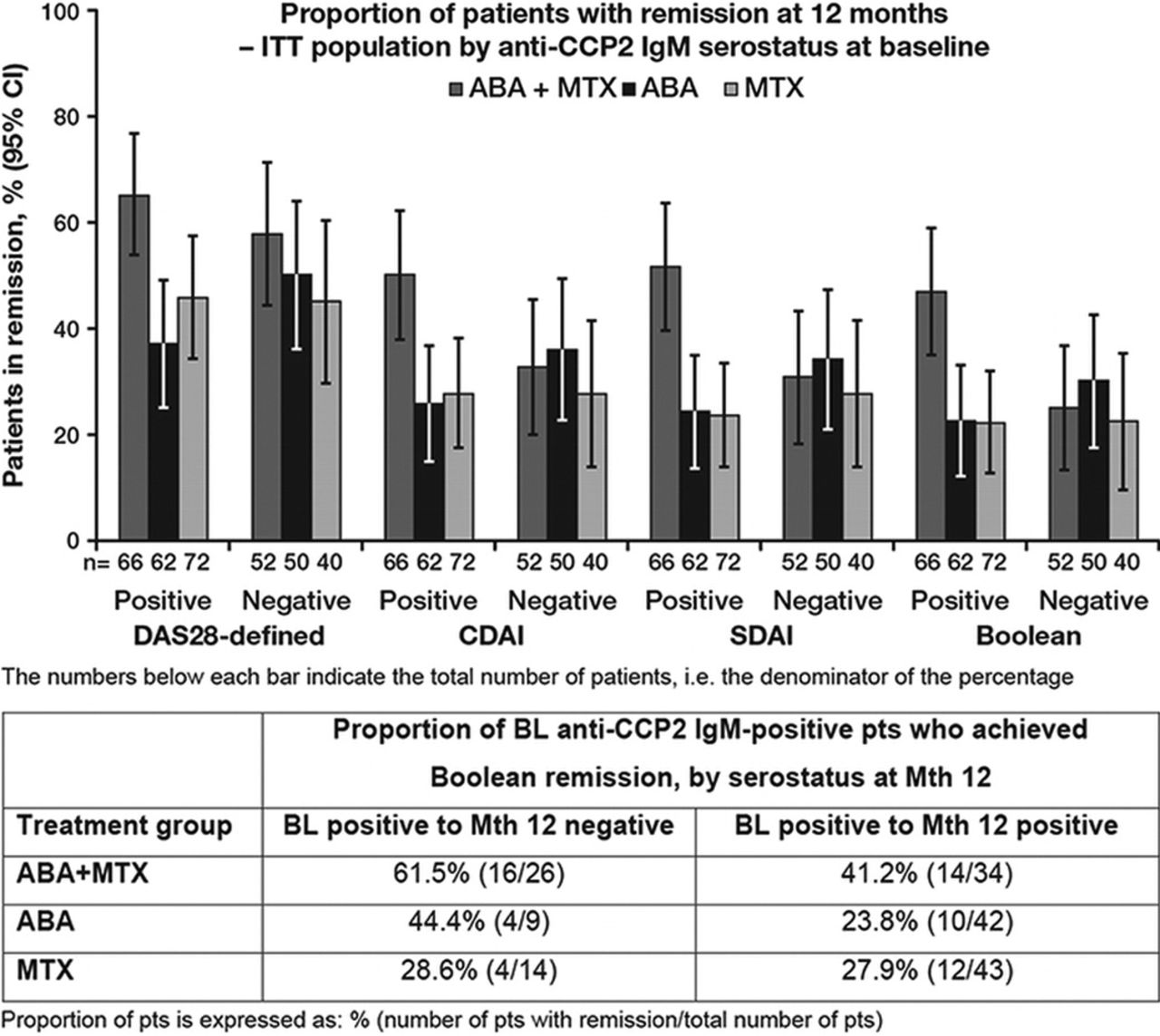
Results In the ABA+MTX treatment arm, a higher proportion of pts who were anti-CCP2 IgM positive at BL achieved remission by all indices compared with pts who were BL IgM negative (Figure). This trend was most clearly observed in the stringent indices of CDAI, SDAI and Boolean remission, compared with DAS28 (CRP)-defined remission. This trend was not observed in either the ABA monotherapy or MTX alone arms. Mean improvement in DAS28 (CRP) and HAQ-DI over time was also greatest in BL anti-CCP2 IgM-positive pts treated with ABA+MTX. A numerically higher proportion of pts who seroconverted from anti-CCP2 IgM positive at BL to negative at Mth 12 achieved Boolean remission versus pts who remained seropositive in the ABA+MTX and ABA monotherapy arms (Table).

{kind=link}
Conclusions Abatacept in combination with MTX had greater clinical efficacy in pts who were anti-CCP2 IgM positive at BL than in those who were anti-CCP2 IgM negative at BL, and in those who seroconverted over time than those who did not, suggesting that the impact on ACPA is associated with clinical benefit.
References
Verpoort KN, et al. Arthritis Rheum 2006;54:3799–808.
Huizinga TWJ, et al. Arthritis Rheum 2014;66:S666. Poster 1515.
Emery P, et al. Ann Rheum Dis 2015:74:19–26.
Disclosure of Interest T. W. J. Huizinga Grant/research support from: EU & Dutch Arthritis Foundation, Consultant for: Abbott Laboratories, Biotest AG, Bristol-Myers Squibb, Crescendo Bioscience, Inc, Novartis Pharmaceuticals Corporation, Pfizer Inc, Roche, sanofi-aventis, Schering-Plough, UCB, Inc., Eli Lilly, Meteor Board, Speakers bureau: Abbott Laboratories, Biotest AG, Bristol-Myers Squibb, Novartis Pharmaceuticals Corporation, Pfizer Inc, Roche, sanofi-aventis, Schering-Plough, S. E. Connolly Shareholder of: Bristol-Myers Squibb, Employee of: Bristol-Myers Squibb, A. Johnsen Employee of: Bristol-Myers Squibb, J. Zhu Employee of: Bristol-Myers Squibb, D. E. Furst Grant/research support from: AbbVie, Actelion, Amgen, Bristol-Myers Squibb, Gilead, GSK, NIH, Novartis, Pfizer, Roche/Genentech, UCB, Consultant for: AbbVie, Actelion, Amgen, Bristol-Myers Squibb, Cytori, Janssen, Gilead, GSK, NIH, Novartis, Pfizer, Roche/Genentech, UCB, Speakers bureau: (CME only) AbbVie, Actelion, UCB, V. P. Bykerk Grant/research support from: Amgen, Pfizer, Bristol-Myers Squibb, Janssen, UCB, Roche/Genentech, Consultant for: Amgen, Pfizer, Bristol-Myers Squibb, UCB, Roche, G. R. Burmester Grant/research support from: Bristol-Myers Squibb, AbbVie, Pfizer, Medimmune, Novartis, Roche, UCB, Lilly, Consultant for: Bristol-Myers Squibb, AbbVie, Pfizer, MSD, Medimmune, Roche, UCB, Speakers bureau: Bristol-Myers Squibb, AbbVie, Pfizer, MSD, Roche, UCB, B. G. Combe Grant/research support from: Pfizer, Roche-Chugai, Speakers bureau: Bristol-Myers Squibb, Merck, Pfizer, Roche-Chugai, UCB, D. A. Wong Shareholder of: Bristol-Myers Squibb, Employee of: Bristol-Myers Squibb, L. A. Trouw: None declared, R. E. M. Toes: None declared, P. Emery Grant/research support from: Abbvie, Merck, Pfizer, Roche, Consultant for: Abbvie, Bristol-Myers Squibb, Merck, Pfizer, Roche, Lilly, Novartis