Article Text

Abstract
Background Studies suggest that periodontitis may be a risk factor for rheumatoid arthritis (RA). The purpose of this study was to determine whether periodontitis is associated with autoantibodies characteristic of RA.
Methods Serum samples were tested for anti-cyclic citrullinated peptide (CCP), anti-mutated citrullinated vimentin (MCV), anti-citrullinated α-enolase peptide-1 (CEP-1), anti-citrullinated vimentin (cit-vim), anti-citrullinated fibrinogen (cit-fib) and their uncitrullinated forms anti-CParg (negative control for anti-CCP), anti-arginine-containing α-enolase peptide-1 (REP-1), anti-vimentin and anti-fibrinogen antibodies in patients with and without periodontitis, none of whom had RA.
Results Periodontitis, compared with non-periodontitis, was associated with a normal frequency of anti-CCP and anti-MCV (∼1%) but a higher frequency of positive anti-CEP-1 (12% vs 3%; p=0.02) and its uncitrullinated form anti-REP-1 (16% vs 2%; p<0.001). Positive antibodies against uncitrullinated fibrinogen and CParg were also more common among those with periodontitis compared to non-periodontitis patients (26% vs 3%; p<0.001, and 9% vs 3%; p=0.06). After adjusting for confounders, patients with periodontitis had 43% (p=0.03), 71% (p=0.002) and 114% (p<0.001) higher anti-CEP-1, anti-REP-1 and anti-fibrinogen titres, compared with non-periodontitis. Non-smokers with periodontitis, compared with non-periodontitis, had significantly higher titres of anti-CEP-1 (103%, p<0.001), anti-REP-1 (91%, p=0.001), anti-vimentin (87%, p=0.002), and anti-fibrinogen (124%, p<0.001), independent of confounders, confirming that the autoantibody response in periodontitis was not due to smoking.
Conclusions We have shown that the antibody response in periodontitis is predominantly directed to the uncitrullinated peptides of the RA autoantigens examined in this study. We propose that this loss of tolerance could then lead to epitope spreading to citrullinated epitopes as the autoimmune response in periodontitis evolves into that of presymptomatic RA.
- Ant-CCP
- Autoantibodies
- Autoimmunity
- Rheumatoid Arthritis
- Smoking
Statistics from Altmetric.com
Background
Rheumatoid arthritis (RA) is a chronic immune-mediated inflammatory disease characterised by synovial inflammation and cartilage and bone destruction that often results in structural damage, disability and functional loss. Causes of RA remain unknown but a complex interplay between genetic and environmental factors is involved in its development.1 A key feature of RA is the presence of antibodies to citrullinated peptide/protein antigens (ACPA) and these have now been included as a criterion in the recent American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) RA classification criteria.2 ACPA can be detected with generic assays such as citrullinated peptide antibodies (anti-CCP)3 or antibodies to distinct autoantigens such as citrullinated fibrinogen, vimentin, α-enolase and collagen.4 ACPA levels are predictive of disease severity and adverse clinical outcomes,5 ,6 and increasing evidence implicates ACPA in RA aetiopathogenesis.4
Studies have suggested an association between RA and periodontitis.7 ,8 Periodontitis, one of the most common chronic inflammatory diseases, is characterised by loss of the periodontal ligament and alveolar bone, and is a major cause of tooth loss. Periodontitis is initiated by a pathogenic biofilm accumulating above and below the gum margin, which in susceptible patients triggers a dysregulated inflammatory immune response that causes collateral host-tissue damage.9–11 Periodontal bacteria enter the circulation and trigger an acute-phase response involving C-reactive protein and fibrinogen,12 and may activate neutrophils.13 Porphyromonas gingivalis, a common periodontal pathogen associated with periodontitis, is the only prokaryote known to express an endogenous peptidyl-arginine deiminase (PPAD) enzyme14 that citrullinates human proteins,15 which are abundantly present in periodontal tissues.16 It is therefore conceivable that increased citrullination of human or bacterial proteins by PPAD, or host peptidyl-arginine deiminases (PAD), in patients with periodontitis may result in a break in immune tolerance to citrullinated proteins and play a causal role in the initiation of RA.
It has therefore been hypothesised that RA-specific autoimmunity may be generated within the periodontium and that periodontal citrullination may be important in generating autoantigens in periodontitis.17 Once systemic tolerance is lost, epitope spreading and cross-reactivity may result, perpetuating the immune response leading to RA. ACPA appear many years before disease onset,18–22 in the preclinical phases up to the development of RA,23 suggesting that the initial immune dysregulation occurs years before symptom onset, although how this takes place initially is yet to be determined. Interestingly, in a recent study using an animal model, immunisation with both uncitrullinated and citrullinated enolase caused rapid-onset arthritis,24 and higher antibody titres to uncitrullinated and citrullinated enolase were shown in mice immunised with recombinant P gingivalis citrullinated and uncitrullinated enolase, indicating that the initiation of the response was not necessarily citrulline dependent.
Few studies have shown that patients with periodontitis have a slightly increased presence and/or titres of ACPA compared to controls,4 ,8 but these studies have all been small and differences between patients and controls were not statistically significant. Moreover, antibodies to peptides and their uncitrullinated controls from specific citrullinated antigens have not been investigated. The purpose of this study was to determine the immune reactivities to peptides from citrullinated and uncitrullinated antigens in non-RA individuals with and without periodontitis.
Methods
Study sample
The study sample comprised patients who had been referred to Birmingham Dental Hospital for treatment of periodontitis or for surgical removal of third molars who had been enrolled in clinical trials on outcomes of periodontal treatment and lower third molar surgery, respectively. Patients in the periodontal study had moderate or advanced periodontitis25 and were otherwise healthy and did not meet any of the following exclusion criteria: pregnancy, lactation, course of anti-inflammatory or antimicrobial therapy or vitamin supplementation within the previous 3 months, regular mouthwash use, and any special dietary requirements (eg, coeliac disease). The presence of moderate to advanced periodontitis was confirmed by clinical and radiographic examination. Patients in the third molar study required surgical removal of at least one lower third molar with the following exclusion criteria: pregnancy, lactation, regular use of anti-inflammatory medication or vitamin supplementation. The presence or absence of periodontitis was ascertained by determination of bone loss from radiographs of the dentition. Smoking status was collected at the study visit and classified as never, former and current. All subjects provided written informed consent and studies were approved by the NHS Research Ethics Service (REC ref 05/Q2707/252 and South Birmingham LREC/0405).
Antibody measurements
Fasting blood samples were collected at baseline, that is, before initiation of any dental treatment and immediately processed, aliquotted and stored at −80°C until analysis.
Anti-CCP antibodies were quantified using second-generation assays (Phadia UniCAP system; Phadia Ltd, Milton Keynes, UK). Antibodies against mutated citrullinated vimentin (anti-MCV IgG) were determined using a quantitative immunometric enzyme immunoassay (ORGENTEC Diagnostika GmbH, Mainz, Germany). These are clinically validated tests with a cut-off for positivity of 10 U/ml and 20 U/ml, respectively.
Antibodies to the uncitrullinated equivalent of CCP (CParg) were measured by ELISA. Sera diluted 1:100 were incubated on plates pre-coated with the antigen (kindly provided by Eurodiagnostica, Malmo Sweden) for 30 min. Plates were washed and incubated with peroxidase-conjugated mouse anti-human IgG (Hybridoma Reagent Laboratory, Baltimore, USA) (diluted 1:3000 in RIA buffer) for 30 min at room temperature. After a final wash bound antibodies were detected with TMB substrate (Biolegend, San Diego, USA). The reaction was stopped by the addition of 1 M H2SO4 and absorbance measured at 450 nm. Optical density (OD) values obtained for each sample were evaluated against a panel of normal healthy individuals to determine relative reactivity.
Antibodies to immunodominant peptides from established RA autoantigens were also measured, including citrullinated α-enolase (amino acids 4–21: KIHA-Cit-EIFDS-Cit-GNPTVE) (CEP-1),26–30 citrullinated vimentin (amino acids 60–75: VYAT-Cit-SSAV-Cit-L-Cit-SSVP)21 ,27 ,31–34 and citrullinated fibrinogen β chain (amino acids 36–52: NEEGFFSA-Cit-GHRPLDKK).21 ,27 ,31 ,33 Serum samples from patients and controls were analysed for antibodies to these peptides by ELISA. Cysteine residues were added at the amino and carboxy-termini of each peptide to facilitate cyclisation, and antibodies to the corresponding arginine-containing control peptides (arginine-containing α-enolase peptide-1 antibodies (REP-1); vimentin and fibrinogen β chain) were measured in parallel. Ninety-six well plates were coated with peptide at 10 µg/ml overnight at 4 °C, washed with PBS-Tween (0.05%) and blocked with 2% BSA for 2 h. Samples were diluted 1:100 in RIA buffer (10 mM Tris, 1% BSA, 350 mM NaCl, 1% Triton-X, 0.5% Na-deoxycholate, 0.1% SDS) and added in duplicate for 1.5 h. Plates were washed with PBS-Tween (0.05%) and incubated with peroxidase-conjugated mouse anti-human IgG (Hybridoma Reagent Laboratory, Baltimore, USA) (diluted 1:3000 in RIA-buffer) for 1 h at room temperature. After a final wash to remove unbound conjugate, bound antibodies were detected with TMB substrate (Biolegend, San Diego, USA). The reaction was stopped by the addition of 1 M H2SO4 and absorbance was measured at 450 nm. OD values obtained for each sample were evaluated against a standard curve for each of the citrullinated peptides and uncitrullinated vimentin peptides and expressed as μ/ml. There was no standard curve available for antibodies to REP-1 or uncitrullinated fibrinogen peptide and these were expressed as OD units. Values greater than the 98th percentile of the healthy controls used in this study were considered positive for all antibodies.
Statistical analysis
Summary statistics were calculated as appropriate. For univariate comparisons between patients with and without periodontitis we used χ2 and Mann–Whitney U tests for categorical and continuous variables, respectively. Multiple linear and logistic regression models were used to compare titres of antibodies to citrullinated and uncitrullinated antigens and prevalence of seropositivity between patients with and without periodontitis, adjusting for age, sex and smoking. Antibody titres were log transformed to achieve normality for linear regression models. To facilitate interpretability of the resulting estimates, antibody titres were standardised and expressed as percentage differences between groups, calculated as (eβ−1)×100. STATA statistical software was used for all analyses.
Results
The total sample included 194 participants, of whom 96 had periodontitis and 98 did not have periodontitis, with a mean age of 46 years (SD±8.9) and 29 years (SD±7.3), respectively. The proportion of women was similar in both groups (62% and 59%, respectively). Current smoking was prevalent in 24% of subjects with periodontitis and 22% of the non-periodontitis subjects. Ever smoking, defined as current and previous smoking, was present among 29% and 45% of the patients with and without periodontitis (p=0.02), respectively. None of the participants had a diagnosis of RA at the time of the study.
Antibody seropositivity
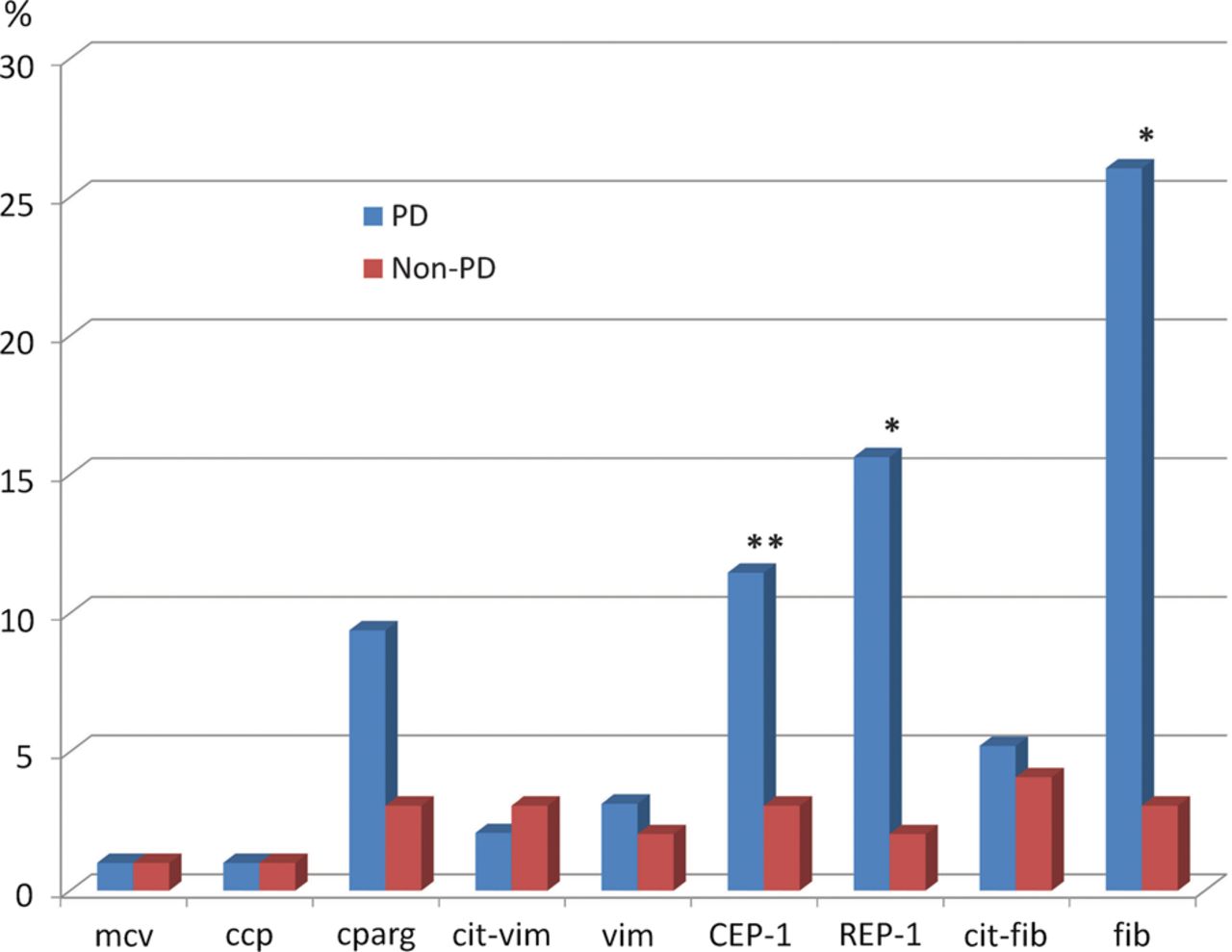
There was a low prevalence of antibody seropositivity to the generic tests for ACPA including anti-CCP and anti-MCV, with frequencies around 1% in both periodontitis and non-periodontitis subjects (figure 1). Among the antibodies to peptides from specific citrullinated antigens, anti-CEP-1 seropositivity was significantly higher in patients with periodontitis compared with non-periodontitis (12% and 3%, respectively; p=0.02). There was no significant difference in the frequency of anti-citrullinated vimentin (cit-vim) or anti-citrullinated fibrinogen (cit-fib) (range 2–5%) in periodontitis and non-periodontitis. The prevalence of antibody seropositivity to the non-citrullinated peptides REP-1 (arginine control peptide for CEP-1) and fibrinogen was much higher in periodontitis. Anti-REP-1 seropositivity was found in 16% with periodontitis compared with 2% in non-periodontitis (p<0.001). Similarly, anti-fibrinogen (negative control peptide for cit-fib) and CParg antibodies (negative control peptide for CCP) were also more common among those with periodontitis compared to non-periodontitis patients (26% vs 3%; p<0.001, and 9% vs 3%; p=0.06, respectively).

Frequency of seropositivity for citrullinated and uncitrullinated antibodies among patients with periodontitis (PD) and without periodontal disease (non-PD). Antibody positivity was defined based on the 98th percentile of the healthy controls. **p=0.02; *p≤0.001. CCP, cyclic citrullinated peptide; CEP-1, citrullinated α-enolase peptide-1 antibodies; cit-fib, citrullinated fibrinogen antibodies; cit-vim, citrullinated vimentin antibodies; CParg, antibodies to the uncitrullinated equivalent of CCP; fib, uncitrullinated fibrinogen antibodies; MCV, mutated citrullinated vimentin; REP-1, arginine-containing α-enolase peptide-1 antibodies; vim, uncitrullinated vimentin antibodies.
Logistic regression models
Logistic regression analyses showed that patients with periodontitis were significantly more likely to have positive anti-CEP-1 (OR 4.1, 95% CI 1.1 to 15) compared to patients without periodontitis, but this difference was attenuated after adjusting for age. After controlling for major confounders, patients with periodontitis were significantly more likely to be anti-REP-1 and anti-fibrinogen positive compared with patients without periodontitis (OR 7.11, 95% CI 1.4 to 36 and OR 10, 95% CI 2.5 to 40, respectively) (table 1).
Logistic regression models
Antibody titres
The distribution of the antibody repertoire in periodontitis compared with non-periodontitis status is shown in figure 2. Serum antibody titres were significantly higher in patients with periodontitis compared with those without periodontitis for antibodies against CEP-1 (p<0.0001), REP-1 (p<0.0001), cit-vim (p=0.003), vimentin (p<0.0001), and fibrinogen (p<0.0001), but not cit-fib (p=0.1) (figure 2). There was no difference between the two groups in anti-CCP, anti-CParg and anti-MCV levels.

Antibody repertoire in patients with and without periodontal disease. The boxes designate the 25th and 75th centiles, while the line in the boxes indicating the median number. The error bars indicate the minimum and maximum values. The numbers on the x axis indicate the periodontal disease (periodontitis; PD) status. CEP-1, citrullinated α-enolase peptide-1 antibodies; cfib, citrullinated fibrinogen antibodies; cvim, citrullinated vimentin antibodies; fib, uncitrullinated fibrinogen antibodies; REP-1, arginine-containing α-enolase peptide-1 antibodies; vim, uncitrullinated vimentin antibodies.
Linear regression models
Univariate analyses confirmed that antibody titres were significantly higher in patients with periodontitis compared with those without periodontitis for antibodies against cit-vim, vimentin, CEP-1, REP-1 and fibrinogen, but not cit-fib. These differences between groups were attenuated by adjustment for age but remained strongly statistically significant (table 2).
Linear regression analyses with antibody titres shown as percentage differences in patients with periodontal disease (periodontitis) compared with patients without periodontitis
Multivariate regression analyses showed that compared to those without periodontitis, patients with periodontitis had 43% (p=0.03), 71% (p=0.002) and 114% (p<0.001) higher anti-CEP-1, anti-REP1 and anti-fibrinogen titres, after adjustment for age, sex and smoking (figure 3). There was no difference between groups in anti-CCP, anti-CParg, anti-MCV, anti-cit-vim and anti-vimentin titres in multivariate analyses.

Antibody titres shown as percentage differences in patients with periodontal disease (periodontitis) compared with patients without periodontitis. The dark blue columns represent the results of univariate linear regression models and the light blue columns show the results of multiple linear regression models controlling for age, sex and smoking. p Values: *p<0.001; **p=0.02; §p=0.002; §§p=0.03. CEP-1, citrullinated α-enolase peptide-1 antibodies; cit-fib, citrullinated fibrinogen antibodies; cit-vim, citrullinated vimentin antibodies; fib, uncitrullinated fibrinogen antibodies; REP-1, arginine-containing α-enolase peptide-1 antibodies; vim, uncitrullinated vimentin antibodies.
There was a highly significant interaction between periodontitis and smoking for anti-CEP-1 (p<0.001) and anti-vimentin antibodies (p<0.001) in age and sex-adjusted models (table 3).
Multivariate linear regression shown as percentage differences in antibody titres in periodontitis subjects compared with non-periodontitis subjects, stratified by smoking
Among non-smokers, patients with periodontitis had significantly higher titres of anti-CEP-1 (103%, p<0.001), anti-REP-1 (91%, p=0.001), anti-vimentin (87%, p=0.002), and anti-fibrinogen (124%, p<0.001), compared with non-periodontitis patients, independent of age and sex.
The levels of anti-cit-vim and anti-cit-fib were also higher among non-smokers with periodontitis compared to non-smokers without periodontitis, although the differences did not reach statistical significance in multivariate models (p=0.30 and p=0.15, respectively). Among smokers, periodontitis was associated with increased anti-fibrinogen antibodies (98%, p=0.006) independent of age and sex. No difference was observed for other antibodies (table 3).
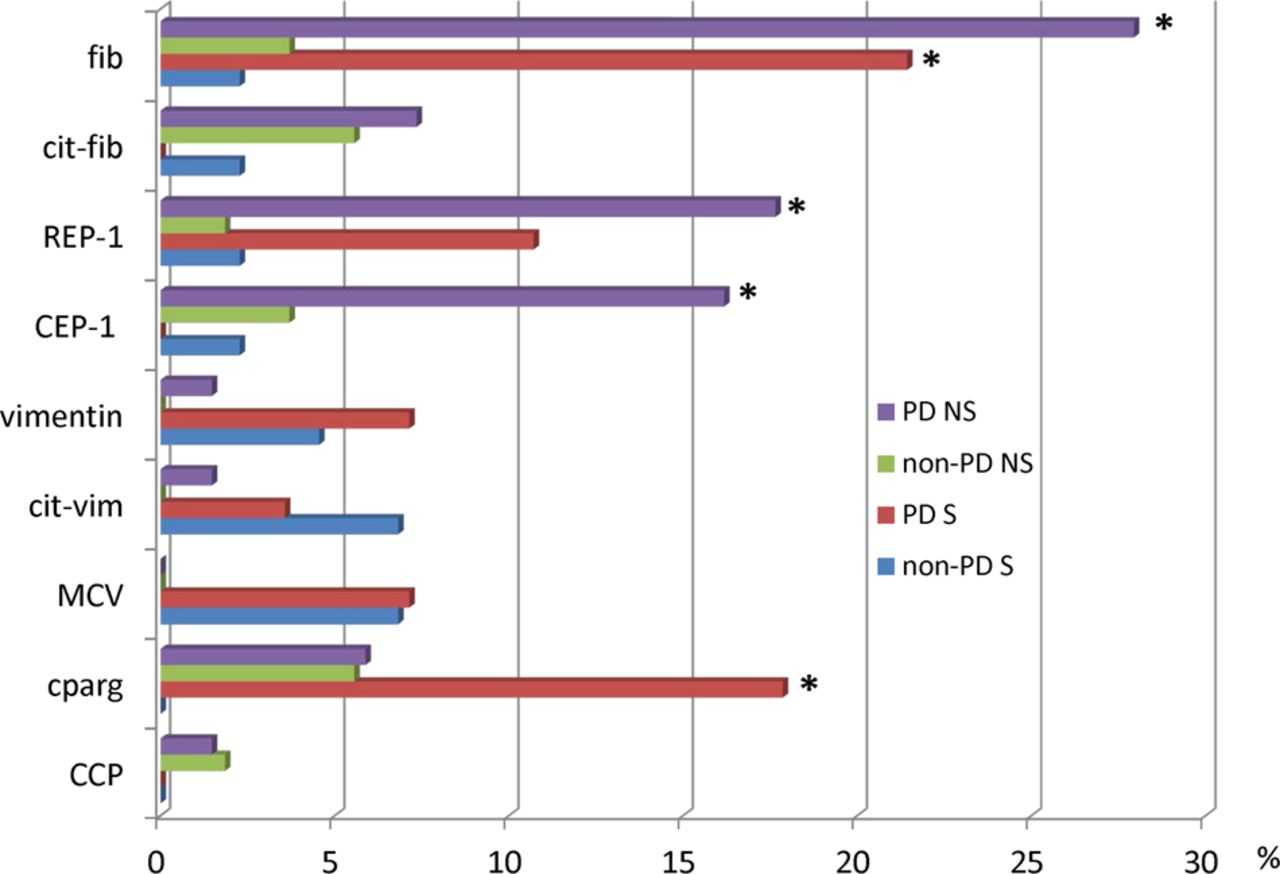
The prevalence of seropositive antibody reactivity to citrullinated and non-citrullinated peptides by periodontitis and smoking status is shown in figure 4. Among smokers, those with periodontitis had a higher frequency of positive anti-CParg (p=0.004) and anti-fibrinogen (p=0.007) compared to non-periodontitis. Among non-smokers, patients with periodontitis had a higher prevalence of positive anti-CEP1 (p=0.02), anti-REP1 (p=0.005) and anti-fibrinogen antibodies (p<0.001) than patients without periodontitis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prevalence of positive citrullinated and uncitrullinated antibody reactivity by periodontal disease and smoking status. Among non-smokers, patients with periodontitis (PD) had a higher prevalence of positive anti-CEP-1 (*p=0.02), anti-REP-1 (*p=0.005), and anti-fibrinogen (*p<0.001) than patients without PD. Among smokers, those with PD had a higher frequency of positive anti-CParg (*p=0.004), and anti-fibrinogen (*p=0.007) compared to non-PD. CCP, citrullinated peptide antibodies; CEP-1, citrullinated α-enolase peptide-1 antibodies; cit-fib, citrullinated fibrinogen antibodies; cit-vim, citrullinated vimentin antibodies; CParg, antibodies to the uncitrullinated equivalent of CCP; fib, uncitrullinated fibrinogen antibodies; MCV, mutated citrullinated vimentin; REP-1, arginine-containing α-enolase peptide-1 antibodies; vim, uncitrullinated vimentin antibodies.
Discussion
To our knowledge, this is the first study to examine the immune reactivity profile to citrullinated antigens and their uncitrullinated forms among individuals with and without periodontitis. The finding of an increased prevalence and titre of antibodies to citrullinated peptides and/or their uncitrullinated controls in periodontitis supports the hypothesis that periodontitis might induce the autoimmunity that evolves into that of established RA. One major unexpected finding was that antibodies to the uncitrullinated controls such as CParg and the fibrinogen peptide were considerably increased in periodontitis relative to their citrullinated variants, which in turn suggests that it may be the uncitrullinated variants of the peptides that break tolerance in periodontitis.
Of the ACPA measured in this study, only one, anti-CEP-1, showed a significantly increased frequency in periodontitis. A similar increase was seen with antibodies to REP-1, suggesting that the anti-CEP-1 response was not citrulline specific. The increased prevalence of autoantibodies to both peptides was confirmed by a highly significant increase in antibody titres in periodontitis. This may be due to crossreaction with the bacterial enolase from P gingivalis,28 a common periodontal pathogen associated with periodontitis. Evidence that this crossreaction may be relevant in vivo was previously demonstrated in an animal model,24 in which immunisation of DR4 transgenic mice with P gingivalis enolase, both citrullinated and uncitrullinated, caused arthritis and antibodies to CEP-1 and REP-1. Therefore the antibody response that we observed in periodontitis could be induced by bacterial enolases from P gingivalis or other bacteria within the pathogenic biofilm.
One of the most striking findings from this study was the significantly increased frequency and levels of antibodies to the uncitrullinated fibrinogen peptide in periodontitis. This cannot be explained by molecular mimicry because, unlike enolase, there is no homologue of fibrinogen in prokaryotes. One explanation may be found in the extraordinary efficiency with which two enzymes from P gingivalis, arginine gingipains and PPAD, can degrade human fibrinogen into small C-terminally citrullinated peptides.14 ,15 This reaction, which occurs in less than 1 min in culture, produces peptides that would not occur with human PAD because human PAD produce only internal citrullines. Therefore, such peptides would be neoantigens that could induce a T-cell response, but with the antibodies reacting with internal (non-citrullinated) amino acid sequences. Moreover, P gingivalis has been shown preferentially to bind fibrinogen and other immobilised extracellular matrix proteins in the presence of their soluble forms,35 which may be a colonisation or nutritional mechanism in the oral cavity and may explain why P gingivalis specifically targets fibrinogen.
Similarly, there was an increased frequency of antibodies to CParg. The mechanisms underlying these phenomena are uncertain, particularly in the case of CParg, because the sequence of the peptides in CCP and CParg has not been published. However, with both antigens, the reaction in the periodontitis sera was preferentially with uncitrullinated forms of the antigen.
There were also raised levels, but not a significantly raised frequency, of antibodies to both citrullinated and uncitrullinated vimentin peptides in our periodontitis population, although the statistical significance of antibodies to citrullinated vimentin was lost in multivariate analysis. Interestingly, there was a highly significant interaction between periodontitis and smoking for anti-vimentin antibodies. Among non-smokers, patients with periodontitis had significantly higher titres of anti-vimentin antibodies, compared with non-periodontitis patients, independent of confounders.
Our finding that the autoantibody response to periodontitis is restricted to non-smokers is intriguing. Smoking is a strong dose-dependent risk factor both for chronic periodontitis36 and tooth loss,37 as well as an established dose-dependent environmental risk factor for antibody positive RA and RA disease severity,38–44 which may be partly mediated through its effect on citrullination of peptides45 ,46 in the lungs of smokers. Major genetic susceptibility factors for RA (ie, HLA-DRB1 shared epitope and PTPN22) and smoking have recently been shown to be associated with anti-CEP-1 and anti-cit-vim-positive RA.26 ,47 In the present study, there was effect modification by smoking. Among non-smokers, patients with periodontitis had higher anti-CEP-1 titres than non-periodontitis patients, and all anti-CEP-1-positive individuals were non-smokers, suggesting that periodontal disease (periodontitis) per se, rather than smoking, is involved in the generation of reactivity against CEP-1 in patients with periodontitis. The anti-cit-vim and anti-cit-fib titres were also higher among non-smokers with periodontitis, although the differences did not reach statistical significance after adjusting for confounders. Our results may suggest that smoking-induced citrullination and the citrullination induced by PPAD (or neutrophil activity during periodontitis) are entirely different mechanisms. Furthermore, the interaction may be due to differences in periodontal pathophysiology between smokers and non-smokers. For example, it is well established that smoking suppresses gingival inflammation,48 ,49 and recent studies suggest that the periodontal microbiome in periodontitis is different in smokers compared to non-smokers.50 Moreover, cigarette smoke has been shown to antagonise antibody-mediated HOCl release in neutrophils,51 which may have downstream effects on neutrophil extracellular trap release.52 The mechanisms whereby periodontitis may ultimately lead to an ACPA response and RA are unknown. Our findings suggest that uncitrullinated peptides may break tolerance in periodontitis, independent of major confounders including age, sex and smoking.
Disease duration could be a key factor in antibody formation and antibody profile. The natural course of periodontitis is known to be that of a slowly progressing disease, which is typically asymptomatic. Given that the periodontitis group consisted mainly of patients with relatively advanced periodontal breakdown, it is likely that they have had chronic periodontitis for many years. Whether these antibodies occur early in the disease course of periodontitis is yet to be determined.
In RA, ACPA precede the appearance of clinically identifiable arthritis by several years,18–22 and epitope spreading occurs before disease onset, but does not expand after disease onset.18–22 This might explain the low frequency of antibody reactivity to the arginine-containing control peptides for α-enolase, vimentin and fibrinogen in established RA, as reported in a study of samples from nearly 2000 RA cases.47 Therefore, if our theory is correct it would be predicted that antibodies to the non-citrullinated versions of RA autoantigens may well occur before the evolution of ACPA. Certainly, it would be well worth studying pre-disease serum samples not only for fine specificity antibodies to established citrullinated antigens but also for antibodies to their uncitrullinated (arginine) control peptides.
In summary, distinct antibody reactivity against both citrullinated and uncitrullinated peptides was observed between individuals with and without periodontitis, independent of major confounders, suggesting that uncitrullinated peptides break tolerance in periodontitis, with epitope spreading to citrullinated epitopes in the small proportion of patients that may evolve into RA.
References
Footnotes
-
Handling editor Tore K Kvien
-
Contributors PdeP was involved in study conception and design, data analysis, interpretation of results and drafting the article. TD made contributions to data acquisition and analysis. MC and MM made contributions to data acquisition. PJV, PJC, CDB, IC and TD made contributions to study implementation, and were involved in revising the manuscript critically for important intellectual content. All authors gave final approval of the final version.
-
Funding This work was supported by ‘Gums & Joints’, a European Union FP7 grant FP7 HEALTH-F2-2010-261460, FP7 ITN project RAPID No. 290246 and by the Birmingham Black Country Comprehensive Research Network (BBC CLRN).
-
Competing interests None.
-
Ethics approval Studies were approved by the NHS Research Ethics Service (REC ref 05/Q2707/252 and South Birmingham LREC/0405).
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Correction notice This article has been updated since it was published Online First. In the results section of the abstract a percentage has been corrected.