Article Text

Abstract
Background: Soluble E-selectin (sE-selectin) is a marker of activation of vascular endothelium.
Objective: To examine serum levels of sE-selectin in a cohort of 85 patients with early rheumatoid arthritis (RA) followed up for five years.
Methods: sE-selectin levels were assessed annually using an enzyme linked immunosorbent assay (ELISA) and related to simultaneously obtained clinical and laboratory measures. Joint inflammation was evaluated by active joint count, functional status by Health Assessment Questionnaire (HAQ), and radiographic findings in hands and feet by the Larsen method. Laboratory tests included serum C reactive protein (CRP) level, erythrocyte sedimentation rate, blood haemoglobin level, white blood cell count (WBC), and platelet count. Area under the curve (AUC) was calculated for each variable, and Jonckheere's test for ordered alternatives was applied to assess significance of association between sE-selectin AUC tertiles and other variables. Baseline sE-selectin tertiles were related to change in Larsen score and HAQ score at five years. Odds ratios (OR) with 95% confidence interval (CI) were calculated using univariate and multivariate logistic regression.
Results: sE-selectin levels were associated with CRP level (p=0.012), WBC (p=0.037), active joint count (p=0.019), progression of joint destruction (p=0.038), and HAQ score at five years (p=0.021), but not with extra-articular symptoms or comorbidity. Baseline sE-selectin levels in the third tertile predicted the HAQ score at five years (OR 4.18, 95% CI 1.15 to 15.22). sE-selectin levels of patients did not differ significantly from those of healthy control subjects.
Conclusion: The degree of activation of vascular endothelium is associated with activity and outcome of early RA.
- E-selectin
- endothelium
- rheumatoid arthritis
- AUC, area under the curve
- CI, confidence interval
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- ESR, erythrocyte sedimentation rate
- HAQ, Health Assessment Questionnaire
- IQR, interquartile range
- OR, odds ratio
- RA, rheumatoid arthritis
- WBC, white blood cell count
Statistics from Altmetric.com
- AUC, area under the curve
- CI, confidence interval
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- ESR, erythrocyte sedimentation rate
- HAQ, Health Assessment Questionnaire
- IQR, interquartile range
- OR, odds ratio
- RA, rheumatoid arthritis
- WBC, white blood cell count
Rheumatoid arthritis (RA) is an autoimmune disease characterised by a chronic inflammation of unknown cause. In addition to persistent joint inflammation, the hallmark of RA, patients often have systemic inflammation. This is reflected in biochemical tests by, for example, raised C reactive protein (CRP) level, secondary anaemia, and increased platelet count and also in symptoms such as loss of weight, fatigue, malaise, and low grade fever. During the course of the disease patients may develop extra-articular features such as alveolitis, glomerulonephritis, and vasculitis.1 Chronic systemic inflammation may also be a risk factor for cardiovascular morbidity2,3 and mortality.4
Systemic inflammation is characterised by activation of the vascular endothelium. Endothelial cells stimulated in vitro with proinflammatory cytokines express E-selectin, a cell adhesion molecule which promotes initial tethering of leucocytes to endothelium, a prerequisite for leucocyte emigration into tissues (reviewed by Ebnet and Vestweber5). Endothelial cells release, most probably by a proteolytic cleavage, E-selectin from their surfaces.6 Soluble E-selectin (sE-selectin) is considered to be a specific marker of endothelial cell activation during systemic inflammation. Low levels of sE-selectin are present in the serum of healthy subjects and increased levels occur in many disorders characterised by the occurrence of systemic inflammation (reviewed by Gearing and Newman7).
Serum sE-selectin levels in patients with longstanding RA have been shown to be comparable with those in healthy controls,8–,10 or raised.11–,13 So far, there seem to be no systematic longitudinal studies of circulating sE-selectin levels in early RA. In the only previous cross sectional study of patients with early RA the levels were not raised.14 In this study we wanted to investigate the role of activation of the vascular endothelium in a cohort of patients with early RA followed up prospectively. We examined the serum sE-selectin levels during the first five years in relation to the severity of systemic inflammation, severity of joint inflammation and destruction, functional status and development of extra-articular manifestations, and comorbidity.
PATIENTS AND METHODS
Patients
The study group comprised 85 consecutive patients (54 women, 31 men) with early RA taking part in an ongoing prospective study carried out at the Department of Rheumatology, University Hospital, Lund, Sweden.15 The patients fulfilled the 1958 American Rheumatism Association (ARA) criteria for definite or classical RA,16 duration of joint symptoms was less than 24 months, and patients were at least 18 years old on presentation. The patients were recruited between 1985 and 1987. Another four patients were enrolled during the same period but were lost to follow up: three of them died (two owing to malignancy and one owing to cardiovascular disease) and one moved to another part of the country. The patients were examined by a rheumatologist at least every six months, with the exception of a few patients in sustained remission who were assessed once a year. At each visit, a clinical examination was carried out and blood was drawn for laboratory analysis. Additional serum samples were stored at −80°C.
Evaluation of joint inflammation, functional status, and joint destruction
Joint inflammation was assessed using the active joint count, defined as the number of joints that were swollen and, in addition, tender on palpation or painful on motion. The 50 joints evaluated included all joints from the Ritchie index,17 except for the neck and the subtalar joints.
Functional status was evaluated with a Swedish version of the Stanford Health Assessment Questionnaire (HAQ) disability index.18
Radiographs of the hands and feet were taken with standard film and an anteroposterior projection at study entry and after five years. The radiographic findings were scored using the Larsen method,19 grading changes from 0 (normal) to 5 (maximal damage). Thirty two joints were evaluated. The wrist score was multiplied by five and all scores were added to yield a joint damage score with a theoretical range of 0–200. The same investigator scored all radiographs. Clinical and laboratory information was not available at the time of the radiological evaluation. Progression of radiographic destruction was evaluated by calculating the difference between the Larsen scores at presentation and after five years.
Evaluation of systemic inflammation
The serum sE-selectin levels were measured from frozen samples using a commercially available ELISA kit (Bender MedSystems Diagnostics GmbH, Vienna, Austria). According to the kit manufacturer, sE-selectin levels are not influenced by repeated freeze-thaw cycles or storage at room temperature. The detection limit was 1.6 ng/ml and intra- and interassay coefficients of variation were 5.4% and 6.0%, respectively. To obtain the sE-selectin level in healthy subjects, serum samples from 51 members of hospital and laboratory staff who were taking no drugs and had no signs of infection were assayed. Measurements were carried out according to the manufacturer's instructions. All samples were measured at least in duplicate.
The erythrocyte sedimentation rate (ESR), serum CRP concentration, blood haemoglobin concentration, and peripheral blood white blood cell count (WBC) and platelet count were determined at the time of the clinical evaluation by routine methods.
HLA-DRB typing and rheumatoid factor measurement
HLA-DRB alleles were typed by restriction fragment length polymorphism analysis with sequence-specific primers, as described previously.20 IgM class rheumatoid factor was analysed by an ELISA.21
Evaluation of comorbidity, extra-articular symptoms, and remission
On presentation, a comprehensive medical history of the patients was obtained. The presence of extra-articular manifestations was recorded continuously. At five years the medical records of the patients were reviewed for any chronic illnesses. Hypertension, thrombosis, cerebrovascular disease, and myocardial infarct were considered to be cardiovascular comorbidities in the analysis of the results.
Remission was defined according to the ARA criteria,22 where remission is defined according to six criteria, five of which must be fulfilled by the patient. However, fatigue was not measured in this study, and remission was therefore considered present if the patient fulfilled four of the remaining five criteria. The patients had to fulfil the remission criteria on at least two consecutive follow up visits (six months apart).
Statistical analyses
The descriptive values of the results are given as median or mean and interquartile range (IQR), range or standard deviation. Individual clinical and laboratory variables of each patient were plotted at one year intervals, and the area under the curve (AUC) was calculated using the trapezoidal rule approximation method and standardised by the length of the study.
The patients were divided into tertiles based on their sE-selectin AUC values, the cut off values being 25 and 38. Jonckheere's test was used to evaluate within the tertiles of sE-selectin AUC values the ordered alternative hypothesis of the AUC values of the other clinical and laboratory variables or the change in Larsen score. The χ2 test was used for categorical variables.
The patients were also divided into tertiles based on their baseline sE-selectin levels, the cut off values being 28 and 40. The outcome measures were categorised, the cut off point (median of the study group) being for HAQ score 0.9 and for change in Larsen score 29. Odds ratios (OR) and associated 95% confidence intervals (CI) were calculated using both univariate and multivariate logistic regression analysis with robust variance estimates. Sex, age at onset, rheumatoid factor, shared epitope, and tertiles of baseline sE-selectin level were entered as covariates.
The Mann-Whitney test was used to assess the differences in the serum sE-selectin levels of patients and control subjects. The Wilcoxon test was used to evaluate the differences in clinical, laboratory, and radiological findings at entry and after follow up. Two tailed p values less than 0.05 were considered significant. No adjustment was made for multiple testing.
RESULTS
Table 1⇓ shows characteristics of the patients. Patients with active disease were offered treatment with disease modifying antirheumatic drugs (DMARDs) together with low dose (≤10 mg daily) prednisolone, if clinically indicated. Active disease was considered as the presence of six or more swollen joints and at least two of the following features: (a) ≥9 tender joints; (b) morning stiffness lasting at least 45 minutes; (c) an ESR of ≥28 mm/1st h. At the first serum sampling, 11 (13%) patients were treated with DMARDs and two of them also with low dose oral prednisolone. Table 2⇓ shows the clinical, laboratory, and radiological findings on presentation and after the five year follow up. Despite the favourable clinical course, the joint destruction progressed. The median change (IQR) of the Larsen score during follow up was 30 (6–55) in the whole patient group.
Characteristics of the patients
Clinical, laboratory, and radiological findings at entry and after the five year follow up
Table 3⇓ presents the AUC values of clinical and laboratory findings according to the tertile distribution of sE-selectin AUC values. Serum CRP levels, peripheral blood leucocyte counts, and active joint counts all had a statistically significant monotonic increasing association with serum sE-selectin level AUC value tertiles.
Clinical and laboratory findings (AUC values) according to tertile distribution of serum sE-selectin AUC values
Table 4⇓ presents the outcome measures according to the tertile distribution of sE-selectin AUC values. The functional outcome—that is, the HAQ scores at the end of the follow up, had a monotonic increasing association with the sE-selectin levels. HAQ score AUC values were not associated with sE-selectin AUC values (data not shown). The progression of radiological joint destruction, expressed as the change in Larsen scores, was also associated with the sE-selectin levels.
Functional and radiological outcome measures according to tertile distribution of serum sE-selectin area under the curve (AUC) values
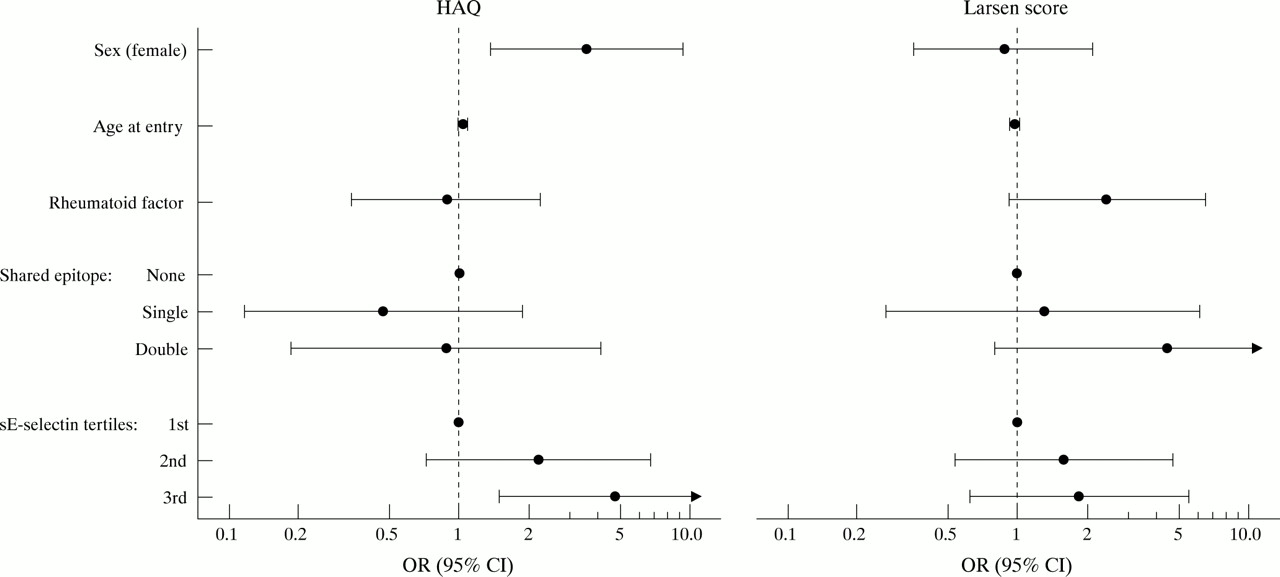
Table 5⇓ presents the results of the multivariate logistic regression analysis of the predictive value of baseline sE-selectin tertiles for functional and radiological outcome, and fig 1⇓ shows the results of the corresponding univariate analysis. The patients with baseline sE-selectin levels in the third tertile had an increased risk of having an above median HAQ score at five years in both multivariate and univariate analyses.
Odds of above median HAQ score at 5 years (cut off point 0.9) and change in Larsen score (cut off point 29) in multivariate logistic regression analysis

{kind=link}
Odds of above median HAQ score at five years and change in Larsen score in univariate logistic regression analysis. Odds ratios with 95% confidence intervals are shown.
At study entry 26 patients had a total of 27 comorbidities (cardiovascular diseases in 20, asthma 3, diabetes 1, goitre 1, malignancy 2). During the five year follow up, seven additional patients developed comorbidities (cardiovascular disease 6, malignancy 1). Six patients developed major extra-articular manifestations (pulmonary disease 2, amyloidosis 2, skin vasculitis 1, polyneuropathy 1). Rheumatoid nodules were detected in 25 patients. sE-selectin levels were not associated with total or cardiovascular comorbidity, extra-articular manifestations, or the presence of rheumatoid nodules. Age, sex, presence of rheumatoid factor or shared epitope, achievement of remission, and use of DMARDs or oral corticosteroids were not associated with the sE-selectin AUC values or with the baseline sE-selectin levels (data not shown).
The median sE-selectin levels of the patients at study entry (35.4 ng/ml, IQR 26.4–49.0, n=85) and healthy control subjects (42.8 ng/ml, IQR 28.5–53.5, n=51) were comparable. Four patients (5%) had a raised sE-selectin level at entry (range 81.6–105.6 ng/ml).
DISCUSSION
In this prospective study of patients with early RA serum sE-selectin levels were associated with markers of systemic inflammation. Previous studies failed to find such associations.10,12,13 However, these other studies were cross sectional and examined patients with chronic RA.
We also found an association between sE-selectin levels and the joint damage process. Other investigators6 have shown a correlation between serum and synovial fluid concentrations of sE-selectin, and our findings might therefore give some support to the hypothesis that E-selectin participates in the pathogenic mechanisms in the rheumatoid joint. The synovial fluid levels are higher in RA than in non-inflammatory joint diseases.6,11 Furthermore, expression of E-selectin molecules occurs in the rheumatoid synovial tissue23,24 and seems to be associated with synovial inflammatory activity.23 E-selectin expression can also be seen in rheumatoid noduli,24 regarded as a form of local vasculitis.
sE-selectin has been reported to have proinflammatory properties. It is chemotactic for monocytes25 and neutrophils,26 increases β2-integrin mediated adhesion26–,28 and superoxide production of neutrophils,27,28 and promotes angiogenesis.29 These proinflammatory properties contribute to the presence of monocytes and neutrophils in the rheumatoid synovial fluid and might thus enhance joint inflammation and destruction.30 On the other hand, it has also been reasoned that sE-selectin might have an anti-inflammatory effect by competing with the endothelial cell membrane bound E-selectin for ligands on the surfaces of leucocytes.7
In our study sE-selectin levels at entry and during follow up were associated with functional status after five years. The observed association can be explained, at least in part, by the proinflammatory properties of sE-selectin, which might promote joint inflammation and thereby compromise physical function of the patient. Furthermore, interleukin 1, the key mediator of systemic inflammation, causes fatigue through its effects on the central nervous system.31 Fatigue affects the subjective experience of functional ability and is reflected in the HAQ score.32,33
The circulating sE-selectin levels in this study were almost within the range of those of healthy control subjects. Similar levels have been detected in another study of 13 patients with early RA14 and also in studies of patients with longstanding RA.8–,10 Such levels, although within the normal range, may affect chronic inflammation and may occur, for example, in patients with clinically relevant atherosclerosis.34,35 Similarly, CRP levels, although within the normal range, have been shown to predict coronary events.36 Given that CRP and sE-selectin are both markers of systemic inflammation, the hypothesis can be proposed that sE-selectin levels within the normal range may also reflect smouldering inflammation. The clinical relevance of sE-selectin levels is an entirely different issue, and the results of this study show that the use of sE-selectin measurements in the clinic cannot be advocated owing to their inadequate predictive value.
Increased circulating sE-selectin levels might maintain low level microvascular inflammation, which may in time result in systemic inflammatory tissue injury. However, in this study on patients with early RA with relatively few cardiovascular complications, comorbidity was not associated with the sE-selectin levels. This is in contrast with previous findings, which showed that raised levels of von Willebrand factor, another marker of endothelial activation, were predictive of thromboembolic complications in patients with chronic RA.37
In conclusion, activation of vascular endothelium, reflected by sE-selectin levels, was associated with joint inflammation and markers of systemic inflammation during a follow up period of five years. Serum sE-selectin levels during follow up were associated with functional and radiological outcome after five years as well, and baseline levels also predicted functional outcome. The results emphasise the importance of activation of vascular endothelium in early RA.
Acknowledgments
The study was supported by grants from the Donation Funds from the Sjukvården I Landskrona Lund-Orup, Riksförbundet mot Reumatism, Konung Gustav V:s 80-års fond, and the Helsinki University Central Hospital Research Funds.