Article Text

Abstract
Background: Active anti-neutrophil cytoplasmic antibody-associated vasculitis (AAV) is commonly treated with cyclophosphamide, a drug with serious side effects, and with corticosteroids.
Objective: To determine the efficacy of a possible alternative drug for cyclophosphamide, oral mycophenolate mofetil (MMF) 1000 mg twice daily and oral prednisolone 1 mg/kg once daily as remission induction treatment.
Methods: 32 consecutive patients with 34 episodes of active vasculitis who could not be treated with cyclophosphamide were diagnosed for a median (range) of 6.0 (0.3–22) years and experienced 4 (0–14) relapses prior to the current episode. Treatment response and relapse-free survival were analysed.
Results: Complete remission (CR) was obtained in 25 (78%) patients, partial remission (PR) in 6 (19%), whereas 1 (3%) patient did not respond. 19 patients relapsed, 13 (52%) after CR, 14 (3–58) months after starting the treatment and 6 (100%) after PR, 6 (2–10) months after starting the treatment. The median relapse-free survival was 16 months, comparable with the interval between the previous relapse and the current MMF-treated relapse (17 (3–134) months). Relapse-free survival at 1, 3, and 5 years was 63%, 38% and 27%, respectively. Patients who had been treated successfully with cyclophosphamide before responded better (CR 84%, relapse 50%) than those who had not (CR 50%, relapse 100%). Minor gastrointestinal side effects and infections occurred frequently. MMF was prematurely discontinued due to adverse effects in two patients.
Conclusion: MMF, in combination with prednisolone, can induce remission in patients with relapses of AAV intolerant to cyclophosphamide.
- AAV, ANCA-assocciated vasculitis
- BVAS, Birmingham Vasculitis Activity Score
- CR, complete remission
- PR, partial remission
- MMF, mycophenolate mofetil
- WG, Wegener’s granulomatosis
Statistics from Altmetric.com
- AAV, ANCA-assocciated vasculitis
- BVAS, Birmingham Vasculitis Activity Score
- CR, complete remission
- PR, partial remission
- MMF, mycophenolate mofetil
- WG, Wegener’s granulomatosis
Treatment of anti-neutrophil cytoplasmic antibody-associated vasculitis (AAV) with cyclophosphamide and oral corticosteroids effectively induces remission. However, cyclophosphamide causes serious acute and long-term side effects, such as haemorrhagic cystitis, opportunistic infections, gonadal failure, bladder cancer, bone marrow depression, myelodysplasia and myeloproliferative disease. Furthermore, 50% of patients with vasculitis relapse at least once within 5 years.1 Cumulative adverse effects due to repeated treatment leads to increasing numbers of patients who cannot tolerate cyclophosphamide. For this reason, and for avoiding cyclophosphamide-related toxicity, alternative induction treatments are sought.
Mycophenolate mofetil (MMF) is a pro-drug. Its active metabolite mycophenolic acid suppresses guanine synthesis in lymphocytes by inhibiting inosine monophosphate dehydrogenase, and blocks DNA synthesis and proliferation after activation.2 As most other cells, in contrast to lymphocytes, can synthesise guanine using a different salvage pathway, the effect on lymphocytes is rather selective, and fewer side effects are expected. Indeed, in general MMF is well tolerated. In patients who underwent renal transplantation, adverse effects led to the discontinuation of MMF within the first year in 8.7% of patients, whereas 5.2% of patients in the placebo/azathioprine group had to stop their medication.3 Moreover, in these patients who underwent renal transplantation, MMF showed superior efficacy when compared with azathioprine. Also, in patients with auto-immune diseases such as systemic lupus erythematosus, MMF was effective in inducing remission with short-term efficacy reported to be comparable with cyclophosphamide.4–,7
To date, five uncontrolled studies and case series,8,9,10,11 one based on some of our patients,12 and two case reports13,14 on the use of MMF in patients with active AAV have been published. We report our experience with MMF in combination with corticosteroids as induction treatment in a cohort of consecutive patients with active AAV who could not be treated with cyclophosphamide.
METHODS
Patients
Between 1997 and 2005, all consecutive patients with active AAV who could not be treated with cyclophosphamide were treated with MMF. These patients fulfilled the Chapel Hill Consensus Conference definitions for Wegener’s granulomatosis (WG) or microscopic polyangiitis.15 All patients gave informed consent.
Treatment
Induction treatment consisted of oral MMF 1000 mg twice daily and oral prednisolone 1 mg/kg once daily (maximum 60 mg). After 1 year, in patients who were still in complete remission (CR), MMF was tapered by 500 mg every 3 months. Prednisolone was tapered after 6 weeks by 10 mg every 2 weeks until a dose of 30 mg was reached, and by 5 mg every 2 weeks until 10 mg. Next, we attempted to reduce the dose by 2.5 mg every month. Other immunosuppressive medication was stopped. All patients received prophylaxis against pneumocystis carinii pneumonia, candidiasis, peptic ulcer disease and osteoporosis. Patients were seen at least every month during the first 6 months and every 6–12 weeks thereafter, and evaluated for disease activity and side effects.
Design
Our treatment protocol was designed to offer an alternative to patients who could not be treated with cyclophosphamide. The study was not controlled. However, as all our patients with AAV in our specialised vasculitis outpatient clinic are treated using protocols for (tapering) immunosuppressive treatment, comedication (prophylaxis against pneumocystis carinii pneumonia, osteoporosis etc) and follow-up, we were able to collect all needed data prospectively. These data were analysed retrospectively.
Definitions
Disease activity at baseline and during follow-up was scored using the Birmingham Vasculitis Activity Score (BVAS).16 CR was defined as the absence of signs or symptoms of active vasculitis (BVAS = 0), in combination with a normal serum C reactive protein level (<10 mg/l).17 Partial remission (PR) was defined as clinically relevant improvement of disease activity without fulfilling the criteria for CR. Relapse/treatment failure was defined as new, increasing or persistent disease activity requiring the use of renewed or intensified immunosuppressive treatment.
Statistics
Values are presented as medians with ranges unless stated otherwise. Actuarial relapse-free survival was calculated using the Kaplan–Meier method.
RESULTS
Patient characteristics
Between 1997 and 2005, 32 consecutive patients with active AAV, who could not be treated with cyclophosphamide, were treated with MMF (table 1⇓).
Baseline characteristics at the moment of start of mycophenolate mofetil induction treatment in 32 patients with active anti-neutrophil cytoplasmic antibody-associated vasculitis.
All patients fulfilled the Chapel Hill Consensus Conference definitions for WG (n = 29) or microscopic polyangiitis (n = 3).15 Patients were diagnosed for a median (range) of 6.0 (0.3–21.6) years before and experienced 4 (0–14) relapses prior to the current episode. One patient was treated for newly diagnosed disease. A total of 15 (47%) patients had active renal disease (biopsy proven in 10). At the moment of relapse, five patients used no immunosuppressive medication, the remainder using cyclophosphamide (n = 4), azathioprine (n = 14), methotrexate (n = 3) and prednisolone (n = 21). Follow-up since start of MMF treatment until relapse or end of follow-up was 19 (1.9–88) months.
Treatment with cyclophosphamide for the current relapse was considered contra-indicated for the following reasons: previous haemorrhagic cystitis (n = 6), treated bladder cancer (n = 2), recently diagnosed melanoma (n = 1), bone marrow depression (n = 7), relapse during maximal tolerated cyclophosphamide (n = 3), previous episodes with insufficient response to cyclophosphamide (n = 3), an unacceptable cumulative dose of cyclophosphamide (n = 4) and patient refusal (n = 6).
Response to treatment
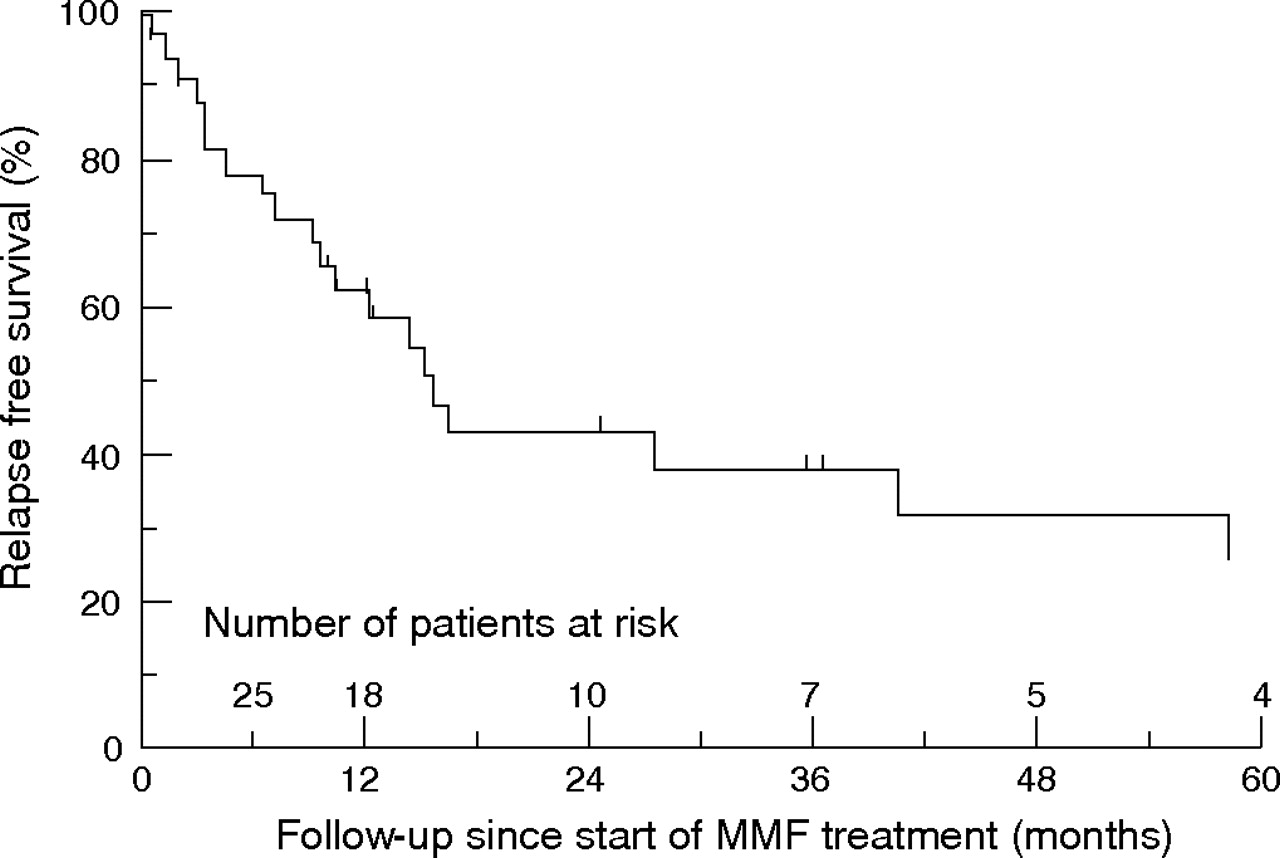
CR was achieved in 25 (78%) patients, PR in 6 (19%) after 2.2 (1–5) months of treatment. One patient (3%) did not respond. This patient developed severe thrombocytopenia within 2 weeks and had to stop MMF. During follow-up, 19 patients with initial response relapsed 12 (2–58) months after start of treatment. Nine patients relapsed within 1 year. Median relapse-free survival was 16 months, which is comparable to the interval between the previous relapse and the current relapse, that was treated with MMF (17 (range 3–134) months (table 1⇑). Relapse-free survival at 1, 3, and 5 years after start of MMF treatment was 63%, 38% and 27%, respectively (fig 1⇓).
{kind=link}
Relapse-free survival (% on vertical axis) in 32 patients with active ANSA-associated vasculitis treated with induction treatment with mycophenolate mofetil (MMF) and prednisolone. Follow-up since start of treatment is indicated (on the horizontal axis) in months; subjects censored are also indicated.
All but 2 patients were still on MMF at the time of relapse, with 12 using prednisolone as well. All PRs (n = 6) were followed by relapse after 6 (2–10) months, while 13 relapses followed CR (n = 25) after 14 (3–58) months (table 2⇓). After CR, median disease-free survival was 41 months. Two patients who relapsed after 40.6 and 16.3 months were treated with a second course of MMF and prednisolone; again, both reached CR that was sustained during 8 and 26 months of follow-up.
Patient and disease characteristics for those with complete remission and those with no or partial remission on induction treatment with mycophenolate mofetil and prednisolone
Renal involvement (n = 15) caused renal dysfunction (increase in creatinine level of 25%) in 12 episodes. Renal function in these 12 episodes (median (range) creatinine level 211 (115–542) μmol/l) improved after starting MMF in eight patients, stabilised in two, while two patients with severe pre-existing renal failure slowly progressed to renal replacement therapy, without signs of active glomerulonephritis, 3 months and 1.5 years later. Neither the response to MMF treatment nor the occurrence of relapses were different between episodes with (n = 15; CR in 12, PR in 2 and relapse in 8) or without (n = 17; CR in 13, PR in 4 and relapse in 11) renal involvement with a median relapse-free survival of 15 and 17 months, respectively.
We looked for differences in disease characteristics in patients who reached CR (n = 25) compared with those who did not (n = 7; table 2⇑). No differences were found in demographic parameters or in disease activity at the time of the current relapse. However, duration of disease and the interval between previous and current relapse were longer in the patients who reached CR. These findings could indicate that the disease in these patients who reached CR tends to relapse less frequently. In the same way, we compared patients who previously responded well to cyclophosphamide (n = 25) with patients who relapsed during the use of cyclophosphamide (n = 3), or with previous failure using this drug (n = 3). The 25 patients who were previously treated successfully with cyclophosphamide responded better to MMF, with CR being achieved in 84% as compared with 50% in the remaining group. In addition, fewer of these 25 patients relapsed (52% vs 100%).
During treatment with MMF, five patients died. Causes of death were invasive aspergillosis (n = 1), ischaemic heart failure (n = 2), metastatic bladder cancer (n = 1) and respiratory failure during relapsed activity of WG (n = 1). Two patients died 6 and 24 months after stopping MMF due to myocardial infarction and sepsis with Staphylococcus aureus, respectively. One patient had active disease at the time of death, and one was in PR.
Adverse effects
Two patients stopped MMF treatment prematurely. One patient reported difficulties with concentration, and switched to methotrexate after 6 months of treatment with MMF once stable CR for 3 months was obtained. One patient with pre-existing thrombocytopenia as reason to avoid cyclophosphamide showed progressive thrombocytopenia within 2 weeks of starting MMF. Five patients reported gastrointestinal complaints, one of whom needed hospitalisation because of diarrhoea. Anaemia (n = 2), thrombocytopenia (n = 4) and leucocytopenia (n = 4) were seen. All these adverse effects responded to, often only temporary, dose reduction of MMF.
During treatment with MMF, 16 infectious episodes occurred in 12 patients: dialysis catheter-related bacteraemia (n = 2), sepsis (n = 1), epidydimitis (n = 1), urinary tract infection (n = 5), bacterial pulmonary infection (n = 3), herpes simplex (n = 1) and herpes zoster (n = 2), all of which resolved with appropriate treatment. Finally, an 81-year-old patient died while in PR, due to invasive aspergillosis despite antifungal therapy, 2 months after starting MMF. None of the infectious episodes occurred during leucocytopenia.
DISCUSSION
The goals of the treatment of AAV have shifted from avoiding mortality to avoiding disease- and treatment-associated long-term morbidity, as current treatment with cyclophosphamide is effective, but also very toxic.1 In addition, with longer patient survival and increasing number of relapses, some patients can no longer be treated with cyclophosphamide at the time of renewed disease activity. Therefore, other treatments are needed. In our study, we show that oral MMF in combination with prednisolone is able to successfully induce remission of active vasculitis in a group of patients with AAV who could not be treated with standard cyclophosphamide treatment. All but one patient responded within 5 months of treatment with MMF and prednisolone. However, the relapse rate was high and overall median relapse-free survival was only 16 months in these negatively selected patients with predominantly longstanding and frequently relapsing AAV. The relapse-free survival was comparable to the interval between the previous and the MMF-treated disease episode (median 17 months), undoubtedly reflecting our selected population. Most patients were diagnosed as having WG, experienced many relapses before, and were proteinase 3-anti-neutrophil cytoplasmic antibody positive, all known risk factors for relapse.18 Furthermore, all patients who did not reach CR (n = 6), those who had relapsed during the use of cyclophosphamide or with previous failure of this drug (n = 6) relapsed. In such patients, switching to an alternative treatment that induces CR should be considered. Importantly, despite these characteristics, median relapse-free survival was 41 months in 78% of patients in whom a CR could be obtained.
We tapered prednisolone somewhat more slowly than others do. It is therefore possible that our results are influenced positively by the dosage of prednisolone we used. However, within 4–5 months, the prednisolone dose is so low that the observed treatment effect cannot be completely explained by the prednisolone. The sustained remission (relapse-free survival 16 months) during follow-up also cannot be explained by the prednisolone used in the first months of the treatment. Of note, we always use and have used this prednisolone-tapering scheme in combination with cyclophosphamide. Therefore, our patients, most of whom had been treated with steroids before, had been given the same amount of steroids in the past. Despite their prior treatment, the interval between the previous and the MMF-treated disease episode was comparable to the relapse-free survival, which also pleads against a disproportionate contribution of the prednisolone.
A total of 46 patients with active AAV receiving induction treatment with MMF have been reported in two uncontrolled studies and two small case series (table 3⇓).8,9,10,11
Efficacy of mycophenolate mofetil as remission induction treatment in patients with anti-neutrophil cytoplasmic antibody-associated vasculitis*
Overall, remission was successfully induced in 70% of these 46 patients (range 33–82). In the pilot study by Joy et al,10 six patients with relapsing disease and six patients who were resistant to cyclophosphamide were treated with MMF. Of these 12 patients, 6 reached CR and 3 reached PR, as shown by decreases in BVAS scores. Similar to our study, the six patients treated for disease activity because of resistance to cyclophosphamide did not respond well to MMF (only two patients reached CR and both relapsed during follow-up). However, these six patients received less prednisolone than the six patients with relapsing disease (data not shown; deduced from treatment protocol). Koukoulaki and Jayne11 described their retrospective experience with MMF for the induction of remission in 22 patients with AAV. Most patients (82%) responded well to MMF, but the relapse rate was high (56% after 2 years). They suggest that low MMF dosing (because of adverse effects) may have contributed to this high relapse rate. Unfortunately, no strict treatment protocol, also with respect to steroid doses used, or commonly used definitions of remission or relapse are provided, which makes their study difficult to assess. In general, patient selection and the use of different treatment protocols and definitions of remission and relapse can explain differences in outcome in these studies and series.
As in these other studies with MMF, our study is not a controlled study. We included patients who could not be treated with (n = 26) or refused cyclophosphamide (n = 6) and who had been difficult to treat in the past. The results of our study can therefore not be extrapolated to all patients with AAV. Furthermore, the retrospective analysis of the data may have led to the underestimation of adverse effects. However, our cohort was treated by a small team of doctors who used the treatment protocol and criteria for (partial) remission and relapse uniformly, and were vigilant in detecting adverse effects.
As MMF is considered a potent immunosuppressive drug with a favourable side effect profile, it constitutes an attractive alternative to cyclophosphamide treatment in patients with AAV. Indeed, MMF was generally well tolerated in our patients, despite the fact that many had previously received multiple courses of cyclophosphamide. During MMF treatment, bone marrow depression resulted in anaemia, leucocytopenia or thrombocytopenia in a number of patients. This depression responded to temporary dose reduction in nearly all patients, but caused treatment failure in one patient. Likewise, a number of infections were encountered, although most were managed successfully without interrupting MMF treatment. No episodes of leucocytopenia preceded these infections. This finding stresses the need for vigilance for infections, irrespective of the leucocyte count. Furthermore, 5 (16%) patients experienced gastrointestinal side effects, which is lower than that reported by others (23% in patients with AAV,11 up to 45.5% in patients who underwent renal transplantation).19 Owing to relatively short follow-up, we have no information about possible long-term side effects. In transplantation medicine, more experience with MMF, usually in combination with calcineurin inhibitors and steroids, is available. This suggests that treatment with MMF is safe with prolonged follow-up.3
Other alternative drugs for cyclophosphamide are currently under study. As shown in one randomised study20 and in two uncontrolled studies,21,22 methotrexate effectively induced remission in 90% and 71–74% of the patients, respectively. However, relapses occurred more frequently than when cyclophosphamide was used (70% vs 47%) after an unusually short treatment period of 12 months.20 Furthermore, methotrexate cannot be used in all patients; it is contraindicated when renal function is impaired. Intravenous immunoglobulins induced remission in 40–82% of patients.23–,26 However, in the former study, no CRs were induced, and no improvements of ophthalmic, pericardial, pulmonary or renal manifestations were seen. Rituximab, a monoclonal antibody against anti-CD20, was useful in several case series27–,29 and four uncontrolled studies.30–,33 However, the response to rituximab may be temporary, as shown by the return of B lymphocytes and the occurrence of relapses after 6–9 months.28,31–,33 A multicentre study is underway. In some patients, 15-Deoxyspergualin can be effective, but has to be administered subcutaneously, and the patients have to be carefully monitored because of frequent occurrence of leucocytopenia.34,35 Furthermore, after withdrawal of 15-deoxyspergualin, the disease relapses. Although daily oral azathioprine is not able to induce remission,36 high-dose intravenous pulse therapy with azathioprine was effective and well tolerated in a small group of patients with WG.37 In conclusion, although some alternative drugs are and will become available, they cannot be used in all patients, are not effective in all patients, or not feasible on a large scale.
Unlike for systemic lupus erythematosus,4–,7 no randomised studies comparing MMF with cyclophosphamide for induction treatment have been performed in AAV. Unfortunately, the uncontrolled nature of and the patient selection in our study allow us to only hypothesise on the efficacy and safety of MMF in less selected patients with AAV. The finding that MMF was effective in our selected patients, who had proven difficult to treat in the past, suggests that MMF may also be useful in patients who are in an earlier stage of their disease. It might even be possible that induction treatment with MMF may be more effective than our results show, both with respect to remission and relapse rates, in less selected patients. Fewer previous immunosuppressive treatment may also beneficially influence some MMF-related side effects. A randomised comparison between MMF and cyclophosphamide for induction treatment of active AAV early on in the course of the disease seems warranted. Moreover, the role of MMF as a maintenance therapy alternative to azathioprine should be investigated, as switching from cyclophosphamide to azathioprine for maintenance therapy may be associated with more relapses during long-term follow-up.38
In conclusion, our results show that MMF can be used to induce remission of active AAV in patients who cannot be treated with cyclophosphamide at the expense of acceptable side effects. Whether induction treatment with MMF deserves a more prominent position in the treatment of AAV should be studied in prospective randomised studies.
REFERENCES
Footnotes
Published Online First 19 December 2006
Competing interests: None.