Article Text

Abstract
Background Biologic-disease modifying anti-rheumatic drugs (b-DMARDS) have become the standard of care for the treatment of rheumatoid arthritis (RA) not adequately responding to conventional therapy. International Guidelines (1) do not provide a preference on the mechanism of action (MoA) to be chosen as first bDMARD therapy. Switching among bDMARDs is also mainly left to the clinician's decision between a second TNF inhibitor (TNFi) or a different MoA. Real-life data have emphasized prescription differences among bDMARDs, possibly influenced by the emerging evidence demonstrating a better safety profile of Abatacept (ABA) compared to anti-TNF agents (2).
Objectives To analyze whether comorbidities influence the choice of the first-line bDMARD or the switching strategy in RA, focusing on the prescription of ABA compared to TNFi.
Methods Patients for the analysis were selected from the Lombardy Rheumatology Network (LORHEN) Registry. The analysis was restricted to LORHEN patients registered since 2008, when ABA become available for use in everyday clinical practice. Comorbidities were categorized into organ-systems groups. The study population was divided into the “first-line” bDMARD prescription, and the “switch” group including all other treatment lines.
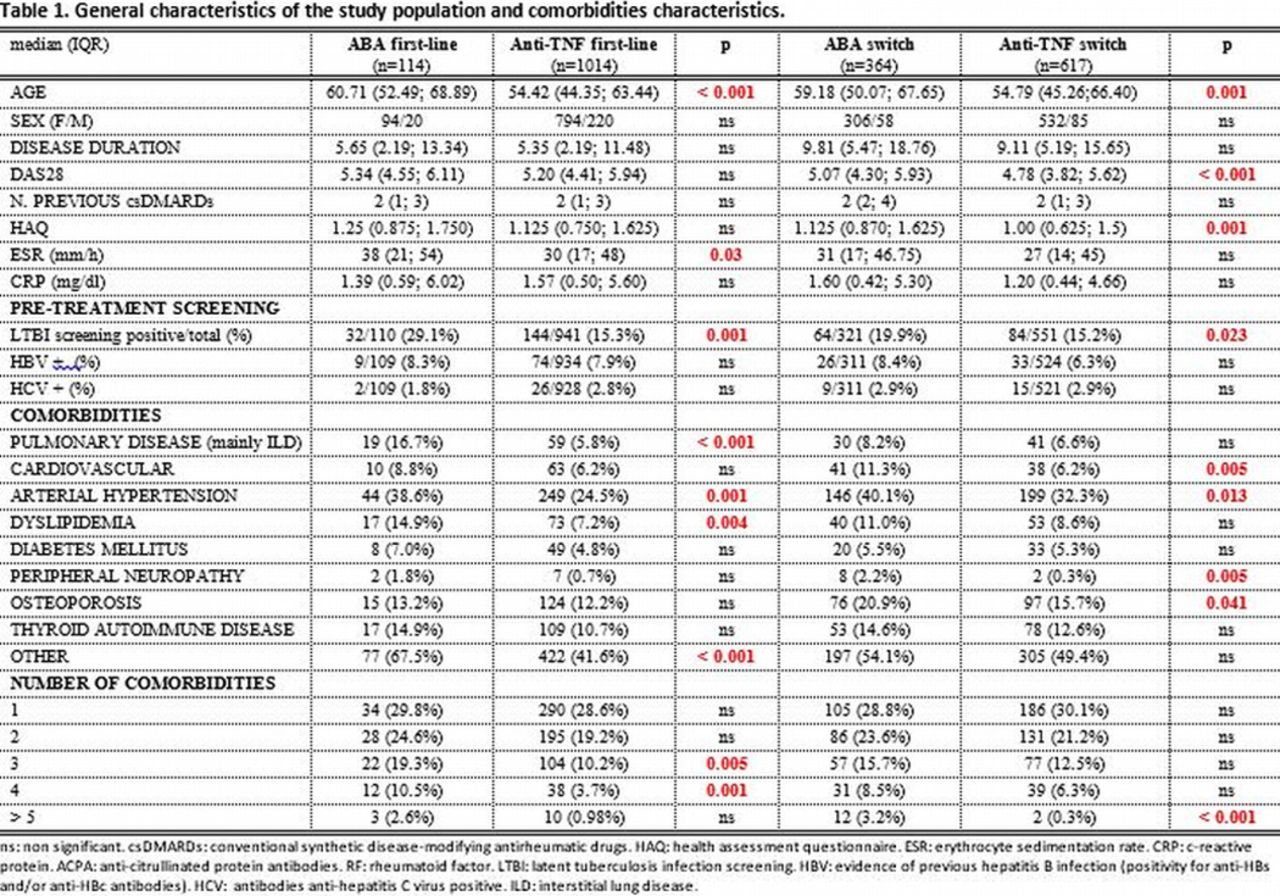
Results A total of n=2109 patients were included in the study. The general characteristics of the population are presented in table 1. Age was significantly higher in patients treated with ABA compared to TNFi. The type and the number of comorbidities were significantly associated with the prescription of ABA as a first-line bDMARD. The presence of pulmonary disease, mainly interstitial lung disease (p<0.001), arterial hypertension (p=0.001), dyslipidemia (p=0.004), and other comorbidities (p<0.001) were significantly more represented in the ABA first-line group compared to TNFi. When switching bDMARDs, the presence of cardiovascular disease (p=0.005), arterial hypertension (p=0.013), peripheral neuropathy (p=0.005) and osteoporosis (p=0.041) were significantly associated with the prescription of ABA. The number of comorbidities was also significantly higher in patients who started or switched to ABA. Positivity of the pre-treatment latent TB screening was significantly associated with ABA prescription in both groups (p=0.001; p=0.023 respectively).
{kind=link}
Conclusions The emerging evidence of a particularly favorable safety profile of ABA reflects into real-life bDMARD prescription. Results from the Italian LORHEN Registry demonstrate that older age, positivity of LTB screening, the type and the number of comorbidities influence the choice of first-line and switching bDMARD, with a preference for ABA compared to TNFi.
References
Smolen JS, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update. Ann Rheum Dis 2014;73(3):492–509.
Schiff M, et al. Head-to-head comparison of subcutaneous abatacept versus adalimumab for rheumatoid arthritis: two-year efficacy and safety findings from AMPLE trial. Ann Rheum Dis 2014;73(1):86-94.
Disclosure of Interest None declared