Article Text

Abstract
AIMS To determine whether HLA-B27 typing helps the clinician in the diagnostic examination of uveitis in a HLA-B27 rich population and also whether the clinical picture of HLA-B27 positive unilateral acute or recurrent anterior uveitis (AAU) is distinguishable from the idiopathic negative form.
METHODS During a 3 year period 220 consecutive patients with undetermined uveitis at onset were examined in the Helsinki University Eye Clinic. HLA-B27 antigen was tested for 85% of the patients. Other laboratory or x ray examinations were performed on the basis of the anatomical classification of uveitis and the biomicroscopic features characteristic of uveitis associated systemic diseases.
RESULTS HLA-B27 antigen was found significantly more often in patients with anterior (71%) and acute/recurrent unilateral (79%) uveitis than in patients with intermediate, posterior panuveitis (7%), and chronic (7%) or bilateral (12%) forms. Of the 16 cases of HLA-B27 negative unilateral AAU, five showed biomicroscopic features representing uveitis entities. The remaining 11 cases did not differ in any respect from the cases of HLA-B27 positive unilateral AAU.
CONCLUSION HLA-B27 antigen helps the clinician in the diagnostic examination of unilateral AAU. Positive test results serve as a clue to search for spondyloarthropathies, and negative results indicate the need to look for specific uveitis entities and other systemic diseases. The occurrence of HLA-B27 positivity in conjunction with uveitis entities other than unilateral AAU is of the same level or less than in the population of Finland in general.
- uveitis
- HLA-B27 typing
Statistics from Altmetric.com
The frequency of HLA-B27 in the general population of Finland (14%) is higher than in most white populations.1 The association of HLA-B27 antigen with acute anterior uveitis (AAU), ankylosing spondylitis (AS), and other seronegative spondyloarthropathies (SpA) has been confirmed by many researchers.2-7 AAU has been one of the commonest uveitis entities diagnosed in both tertiary eye care centres and in general practices of ophthalmology.8 The clinical picture and outcome of HLA-B27 positive AAU with or without systemic disease has been reported to differ from that of HLA-B27 negative AAU.9-11 However, HLA-B27 negative AAU has been associated with different diseases, which have varied from survey to survey. It has been difficult to compare the observations of these heterogeneous series.
The aim of our study was to determine whether HLA-B27 typing not only helps the clinician in the diagnostic examination of unilateral AAU but also the examination of bilateral and/or chronic and/or posterior uveitis or whether HLA-B27 antigen is only a coincidence in many patients of Finland's genetically HLA-B27 rich population. We also wanted to determine whether the clinical picture of idiopathic HLA-B27 positive and negative AAU groups differs.
Patients and methods
Between March 1993 and February 1996 we conducted a prospective study of patients treated for uveitis in the outpatient clinic of the department of ophthalmology in the Helsinki University Hospital. Altogether 277 consecutive patients were referred to the clinic by practising ophthalmologists, general practitioners, or specialists from other hospitals in southern Finland.
Each patient's history of ocular and systemic diseases and also his or her family history were recorded. Questions were asked about respiratory, genitourinary and neurological symptoms, gastrointestinal infections and disorders, back pain and arthralgia, mucocutaneous lesions, tick bites, and journeys abroad. Data concerning age, sex, age at onset of first uveitis, number of attacks, and duration of present attack were collected on standard forms. On the basis of the clinical data, 57 patients with a history of systemic diseases known to be associated with uveitis entities were excluded from the study, leaving 220 patients with a diagnostic challenge.
A visual acuity test, tonometry, a slit lamp examination, and an evaluation of the fundus with a 90 dioptre lens, or indirect ophthalmoscopy, and a three mirror lens when necessary, were performed. Uveitis was graded as anterior, intermediate, posterior, or panuveitis according to the criteria of the International Uveitis Study Group.12 It was considered acute if it disappeared within 3 months and chronic if not. In cases of one or more previous acute attacks, it was categorised as recurrent. Furthermore, when both eyes were affected simultaneously, the uveitis was classified as bilateral; otherwise it was recorded as unilateral.
Eighty five per cent of the patients were tested for HLA-B27 antigen with a flow cytometer using a Becton Dickinson HLA-B27 kit (specificity 99.2%).13 Because Finland is endemic for Lyme borreliosis,14 antibodies to Borrelia burgdorferi and treponemal serology were examined for 86% of the patients on the basis of the differential diagnosis. The results of these patients have been reported elsewhere.15 Other laboratory and x ray examinations were performed if indicated by the medical history, the anatomical classification of uveitis, and the clinical and biomicroscopic specific features characteristic of uveitis associated disorders. In patients with granulomatous uveitis and/or with symptoms suspicious of sarcoidosis, serum angiotensin converting enzyme and serum lysozyme were analysed, and the chest x rays were examined. Antitoxoplasma antibodies were tested for patients with a focal retinochoroiditis. Antinuclear antibodies were tested for children under 16 years of age with joint symptoms and for adults when a connective tissue disease was suspected.
The diagnosis of systemic disease was confirmed by specialists. Patients with back pain or arthralgia suspicious of spondyloarthropathies or other rheumatic disorders were referred to a rheumatologist. Ankylosing spondylitis was diagnosed according to the criteria set by the New York Symposium on Population Studies in Rheumatic Diseases.16 In the diagnosis of non-systemic specific ocular entities, current diagnostic criteria17were followed. Statistical analyses were performed using the equal variance t test, Fisher's exact test, the χ2 test, and the Mann–Whitney U test.
Results
A total of 220 patients (99 men and 121 women) had no established systemic disease known to be associated with uveitis entities when they entered this study. At the time of the first symptomatic uveitis attack the subjects' median age was 36 (range 9–91) years.
Seventy one per cent of the patients with anterior uveitis but only 7% of the patients with intermediate, posterior, or panuveitis were positive for HLA-B27 antigen (χ2, 1 df=76.24, p<0.0001) (Table 1). In addition, 79% of the patients with acute or recurrent unilateral disease, but only 7–12% of those with chronic and/or bilateral disease were HLA-B27 positive (χ2, 1 df=94.90, p<0.0001) (Table 2).
HLA-B27 antigen and the anatomical location of uveitis
HLA-B27 antigen and the duration and laterality of uveitis
Of the patients with unilateral acute or recurrent anterior uveitis, 72 (82%) were HLA-B27 positive and 16 (18%) were HLA-B27 negative (Table3). In the latter group, biomicroscopic specific features gave clues to distinct uveitis entities in five cases. Three patients had patchy or sectorial iris atrophy combined with fatty keratic precipitates suggestive of herpetic infections, one patient had sarcoid lung manifestations in the x ray and histologically confirmed conjunctival granulomas, and one patient had a clinical picture consistent with Posner Schlossman uveitis. Among the unilateral HLA-B27 positive AAU patients, ankylosing spondylitis was diagnosed in one man and one woman. In addition, undetermined spondyloarthropathy was detected in seven people.
General characteristics and biomicroscopic features of the unilateral cases of acute anterior uveitis
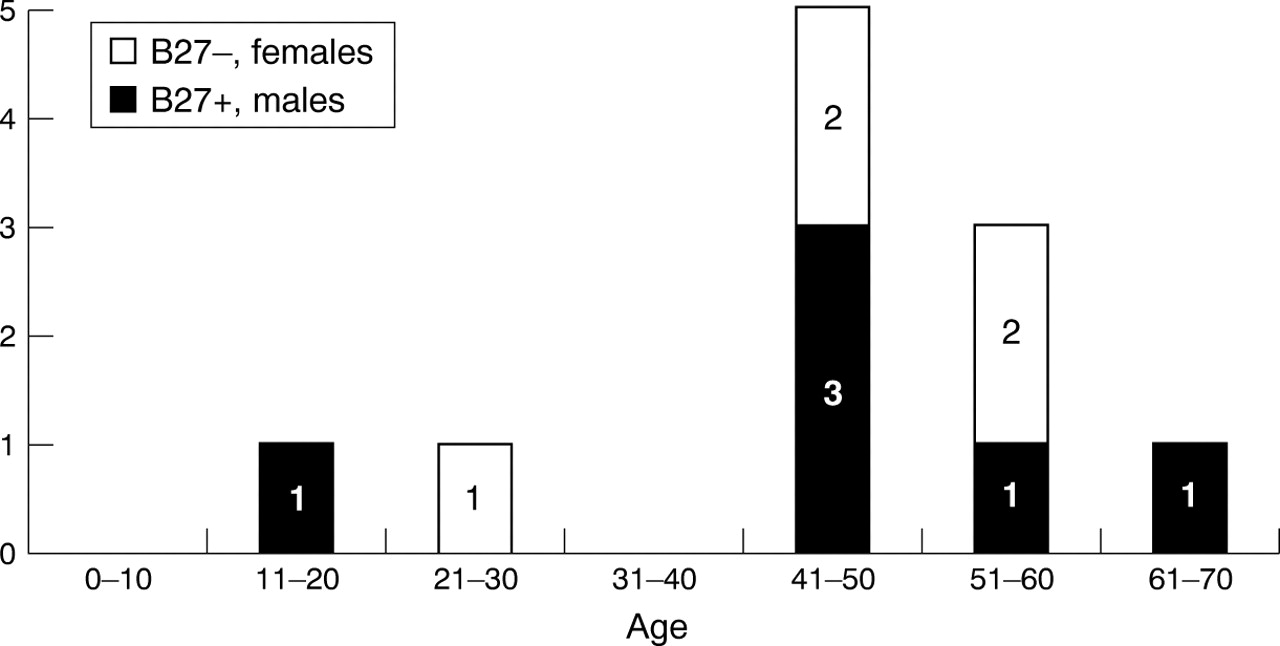
The median age at the time of the first uveitis attack was significantly lower (30.5 versus 45 years) (Mann–Whitney U test, p=0.007) for the HLA-B27 positive unilateral AAU group (Fig 1) than for the group with HLA-B27 negative idiopathic unilateral AAU (Fig 2). The male to female ratio was 1.2:1 and 1.3:1 for the idiopathic HLA-B27 positive and negative groups, respectively (Table 3). The male dominance (3.5:1) was more evident among the patients with ankylosing spondylitis or spondyloarthropathy than among the idiopathic cases. However, in the age group of over 40 years, there was a tendency towards female dominance among the HLA-B27 positive unilateral AAU cases (Fig 1).

Age at onset of the first uveitis in the HLA-B27 positive group with acute anterior uveitis.

{kind=link}
{kind=link}
Age at onset of the first uveitis episode in the HLA-B27 negative group with acute anterior uveitis.
Patients with HLA-B27 positive unilateral AAU, especially when associated with ankylosing spondylitis or spondyloarthropathy, had a history of recurrent attacks more often than patients with idiopathic HLA-B27 negative unilateral AAU (Table 3). The presence of fibrin exudate was not observed to be more frequent in patients with idiopathic HLA-B27 positive unilateral AAU (43%) than in those with idiopathic HLA-B27 negative unilateral AAU (55%) or in those with ankylosing spondylitis or spondyloarthropathy (56%). Hypopyon was detected in 11% of the HLA-B27 positive and 18% of the HLA-B27 negative patients between the HLA-B27 positive and idiopathic HLA-B27 negative groups.
In the entire group of 220 patients, HLA-B27 positivity was unevenly distributed among the patients with different uveitis entities or associated disorders (Table 4). Seventy four cases (34%) were categorised as idiopathic unilateral acute anterior uveitis. Eighty five per cent of these cases were HLA-B27 positive. Ankylosing spondylitis or related spondyloarthropathy was diagnosed in 10 patients with HLA-B27 positive anterior uveitis, one of which was chronic and bilateral in nature. None from the idiopathic HLA-B27 negative group had ankylosing spondylitis or spondyloarthropathy. Among the systemic disorders most were sarcoidosis (12/14). Of those with sarcoid uveitis, six out of the seven tested were HLA-B27 negative. Of the patients with infections, only one with herpes induced uveitis, one with Lyme borreliosis, and none with toxoplasma retinochoroiditis were HLA-B27 positive. As regards uveitis entities such as Fuchs' heterochromic iridocyclitis and pars planitis, and also posterior uveitis entities such as white dot syndromes and idiopathic retinal vasculitis, HLA-B27 antigen was found in only one case out of the 34 tested. In 48 cases (23%) a final diagnosis could not be made. The vast majority of this group was HLA-B27 negative.
Distribution of HLA-B27 antigen in uveitis entities or associated disorders
Discussion
Our uveitis study population had a homogeneous demographic background. All the patients were white and were born in Finland. Although our clinic is a tertiary eye care centre, 30% of the patients are referred by general practitioners.
In published reports HLA-B27 has been examined in unilateral acute or recurrent anterior uveitis patients but in only some of the patients with bilateral or chronic uveitis or intermediate, posterior, or panuveitis.2-4 18-23 One might argue on the basis of the evidence that only AAU has a relation with HLA-B27 antigen. However, since we found no studies in the literature on this topic and HLA-B27 is common in our population, we wanted to determine the distribution of HLA-B27 antigen with respect to different uveitis entities. Furthermore, we were interested in whether the presence of HLA-B27 antigen helps to categorise uveitis when the clinical picture is not typical at onset. Unilateral AAU can begin insidiously, and affect one eye after another in a short period of time. However, it has sometimes been classified as bilateral. In addition the evaluation of the fundus is sometimes impossible in the beginning of iridocyclitis because of a reaction in the anterior vitreous.
In our series HLA-B27 existed significantly more often in cases of unilateral, acute/recurrent, and anterior uveitis than in bilateral and/or chronic ones. In addition, HLA-B27 antigen was found significantly less frequently in relation to other uveitis entities and systemic diseases than in conjunction with unilateral AAU and spondyloarthropathies. The diagnosis of these disorders was based on duration, laterality, typical biomicroscopic features, and, in selected cases, some laboratory and ancillary tests. These findings suggest that the clinician does not benefit from HLA-B27 typing when uveitis is classified as bilateral and/or chronic or the inflammation is located in the posterior part of the eye. However, HLA-B27 positive AAU in connection with symptoms suspicious of spondyloarthropathy can sometimes develop into posterior or panuveitis. Rodriguez and colleagues23 described a series of patients with seronegative arthritic syndromes and HLA-B27 associated uveitis with severe, sight threatening, posterior segment ocular manifestations. There were five patients in our original series who were HLA-B27 positive and who also had spondyloarthropathy. Their inflammation began as acute anterior uveitis but during the course of the disease involved also posterior uveal tissues. We classified these cases as panuveitis. The systemic diseases and HLA-B27 positivity were diagnosed the patients entered our study; therefore we excluded them according to our study protocol. HLA-B27 typing can be recommended in posterior or panuveitis when associated with symptoms of spondyloarthropathies. Because patients with typical symptoms of iritis and unilateral acute anterior eye involvement have an 80% probability of being HLA-B27 positive in Finland, one could assume that HLA-B27 typing is not necessary at all in such cases. Power and colleagues11showed that the prognosis of anterior uveitis associated with the HLA-B27 haplotype, either with or without associated systemic disease, was less favourable when compared with that of HLA-B27 negative patients with idiopathic anterior uveitis. In addition to having their prognosis estimated, AAU patients benefit from HLA-B27 typing because a positive test result alerts the clinician to the need to search for spondyloarthropathies.
Of the unilateral AAU patients in our study, only 13% were diagnosed as having spondyloarthropathy, in contrast with the 24% to 90% reported earlier by other researchers.9 11 18-22 24-31 Our series consisted strictly of patients with unilateral acute or recurrent anterior uveitis with no previous history of systemic diseases. There were 27 patients with spondyloarthropathy that had been diagnosed earlier in the excluded group, five of whom had posterior eye involvement. In addition, 34 of our 72 unilateral HLA-B27 positive AAU patients had their first attack when entering our study, and they may not have had time to develop the symptoms characteristic of ankylosing spondylitis. One might also argue that asymptomatic ankylosing spondylitis or undifferentiated spondyloarthropathy might have been diagnosed if all the patients had been referred to a rheumatologist and sacroiliac x rays had been taken. However, we believe that, in addition to exogenous factors, there must be other genetic markers besides HLA-B27 that predispose patients to ankylosing spondylitis or related spondyloarthropathies. These conclusions are supported by the results of epidemiological, family, and twin studies.5-7
The second most important reason for the HLA-B27 typing of unilateral AAU patients is its value to differential diagnosis. The lack of HLA-B27 antigen in a unilateral AAU patient may be a clue for the clinician to search for other specific uveitis entities and other systemic diseases. In our series five out of 16 HLA-B27 negative AAU cases involved distinct uveitis entities when examined carefully. The remaining 11 did not differ in clinical manifestation from the idiopathic B27 positive ones, although the sample size was too small for definite conclusions. This phenomenon has been observed also previously in four patients by Linssen and Meenken.10Whether idiopathic unilateral HLA-B27 negative AAU is a specific uveitis entity is subject to debate.
We conclude that HLA-B27 antigen is highly prevalent among patients with unilateral AAU. In uveitis entities affecting the posterior part of the eye or bilateral or chronic in nature, HLA-B27 was found rarely. The biomicroscopic features of HLA-B27 positive patients with or without spondyloarthropathies did not differ from idiopathic HLA-B27 negative ones.
Acknowledgments
This study was supported by the Eye and Tissue Bank Foundation (Silmä-ja kudospankkisäätiö). The authors wish to thank Professor Marjatta Leirisalo-Repo for her advice in editing the manuscript.