Article Text

Statistics from Altmetric.com
Psoriasis is an important clinical feature in ankylosing spondylitis (AS) and spondyloarthritis (SpA) in general,1 with inflammatory spinal disease developing in 5%–25% of psoriasis cases.2 ,3 However, there have been few studies assessing the differences between AS patients with and without concomitant psoriasis.4–9
Our aim was to compare the demographic, clinical and imaging characteristics between AS patients with and without psoriasis. Baseline data from an 80% random sample of the AS Study for the Evaluation of Recombinant Infliximab Therapy (ASSERT) database were used for this analysis. Details of the ASSERT trial and study population have been previously published.10 Briefly, patients with active AS (fulfilling modified New York criteria) for at least 3 months, a Bath AS disease activity index score of at least 4 (range 0–10) and a spinal pain assessment score of at least 4 (range 0–10) were eligible for the study.
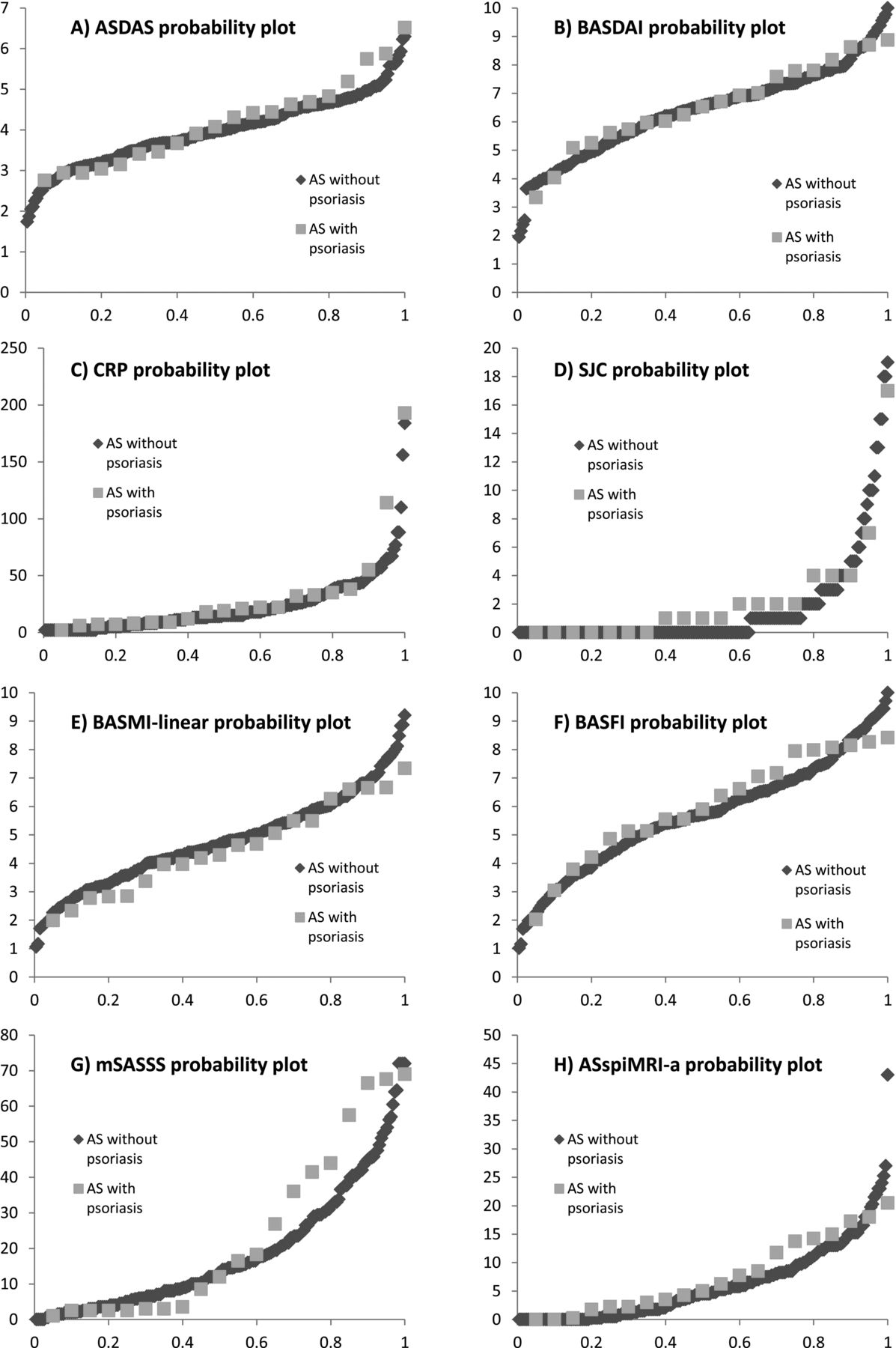
AS patients with psoriasis (n=20) were similar to AS patients without psoriasis (n=191–201) (table 1), namely, regarding baseline demographic characteristics (age, disease duration, body mass index and sex), genetic features (human leukocyte antigen-B27 positivity), presence of extra-articular manifestations (uveitis and inflammatory bowel disease), disease activity measures (AS disease activity score, Bath AS disease activity index, patient global assessment and C reactive protein), severity of enthesitis (Mander enthesitis index), measures of spinal mobility (individual measures and the Bath AS metrology index), physical function (Bath AS functional index), health related quality of life (36-item short form health survey), spinal radiographic damage (modified Stoke AS spine score), location of damage in cervical versus lumbar spine and MRI inflammation of the spine (AS spine MRI score for activity). The only difference that we found was regarding the number of swollen joints. However, this difference did not seem clinically relevant (average 2.4±3.9 swollen joints in patients with psoriasis vs 1.6±3.5 in patients without psoriasis) and the swollen joint count was not independently associated with the presence of psoriasis in the logistic regression analysis (table 1). Probability plots for several outcome measurements were created and stratified for AS patients with and without psoriasis, confirming the similarity between groups at the individual level (figure 1).
Comparison of baseline demographic, genetic, clinical and imaging characteristics of patients with and without psoriasis in the study cohort

{kind=link}
Probability plots for (A) ASDAS, (B) BASDAI, (C) CRP, (D) SJC, (E) BASMI-linear, (F) BASFI, (G) mSASSS and (H) ASspiMRI-a, stratified for AS patients with and without psoriasis. The y-axis represents the score of the outcome measure and the x-axis represents the cumulative probability. AS, ankylosing spondylitis; ASDAS, ankylosing spondylitis disease activity score; ASspiMRI-a, ankylosing spondylitis spine MRI score for activity; BASDAI, Bath ankylosing spondylitis disease activity index; BASFI, Bath ankylosing spondylitis functional index; BASMI, Bath ankylosing spondylitis metrology index; CRP, C reactive protein; mSASSS, modified Stoke ankylosing spondylitis spine score; SJC, swollen joint count.
In this study, we found that demographic characteristics, disease activity, spinal mobility, physical function, structural damage and quality of life are comparable between AS patients with and without psoriasis. Previous studies, performed in heterogeneous populations (early inflammatory back pain, axial psoriatic arthritis and AS patients) have shown conflicting results.4–9 One of the advantages of our study is the large number of disease variables that were studied. One of the limitations of our study is the low number of patients with psoriasis (20 patients, 10% of the study population), increasing the risk of type II error (ie, the failure to reject a false null hypothesis). Furthermore, this is a clinical trial cohort of patients with severe and active disease fulfilling modified New York criteria for AS; therefore, results are not generalisable to other axial SpA subgroups. Importantly, futures studies should focus on the whole spectrum of axial SpA patients, including patients with radiographic and non-radiographic axial SpA.1 The application of the axial SpA paradigm can be a particularly useful and unifying concept, given the long-standing debate on the question of whether patients with inflammatory back disease and psoriasis represent AS with psoriasis or psoriatic spondylitis.1 ,3
References
Footnotes
-
Contributors All authors participated in the design of the analyses. PM, RL and DvdH performed the analyses. All authors participated in drafting the paper and all authors approved the final manuscript.
-
Funding PM was supported by the Fundação para a Ciência e a Tecnologia (FCT) grant SFRH/BD/62329/2009.
-
Competing interests None.
-
Ethics approval Ethics committee approval was secured for the ASSERT trial. This study is an investigator-preformed subanalysis of the ASSERT cohort.
-
Provenance and peer review Not commissioned; externally peer reviewed.