Article Text

Statistics from Altmetric.com
Primary Sjögren’s syndrome (pSS) is a chronic autoimmune disease characterised by lymphocytic infiltration of the exocrine glands, presenting chiefly with keratoconjunctivitis sicca and xerostomia. Estimates of the prevalence of pSS have varied widely among population based surveys, partly because of the different classification criteria used and partly because of methodological differences. We previously reported the prevalence of pSS as 0.15%, in the ESORDIG study,1 and we now report more detailed information about these patients and compare our findings with those from other studies.
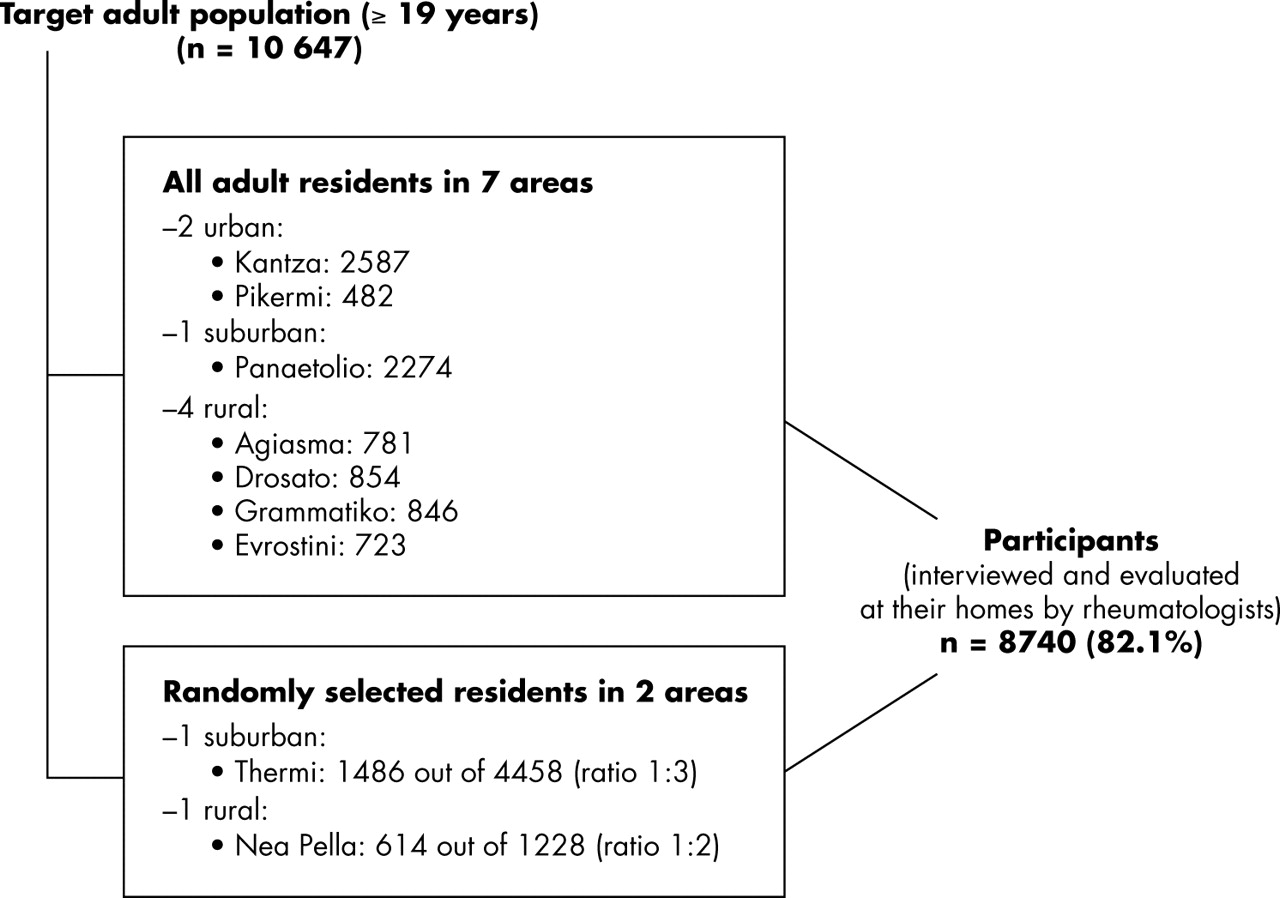
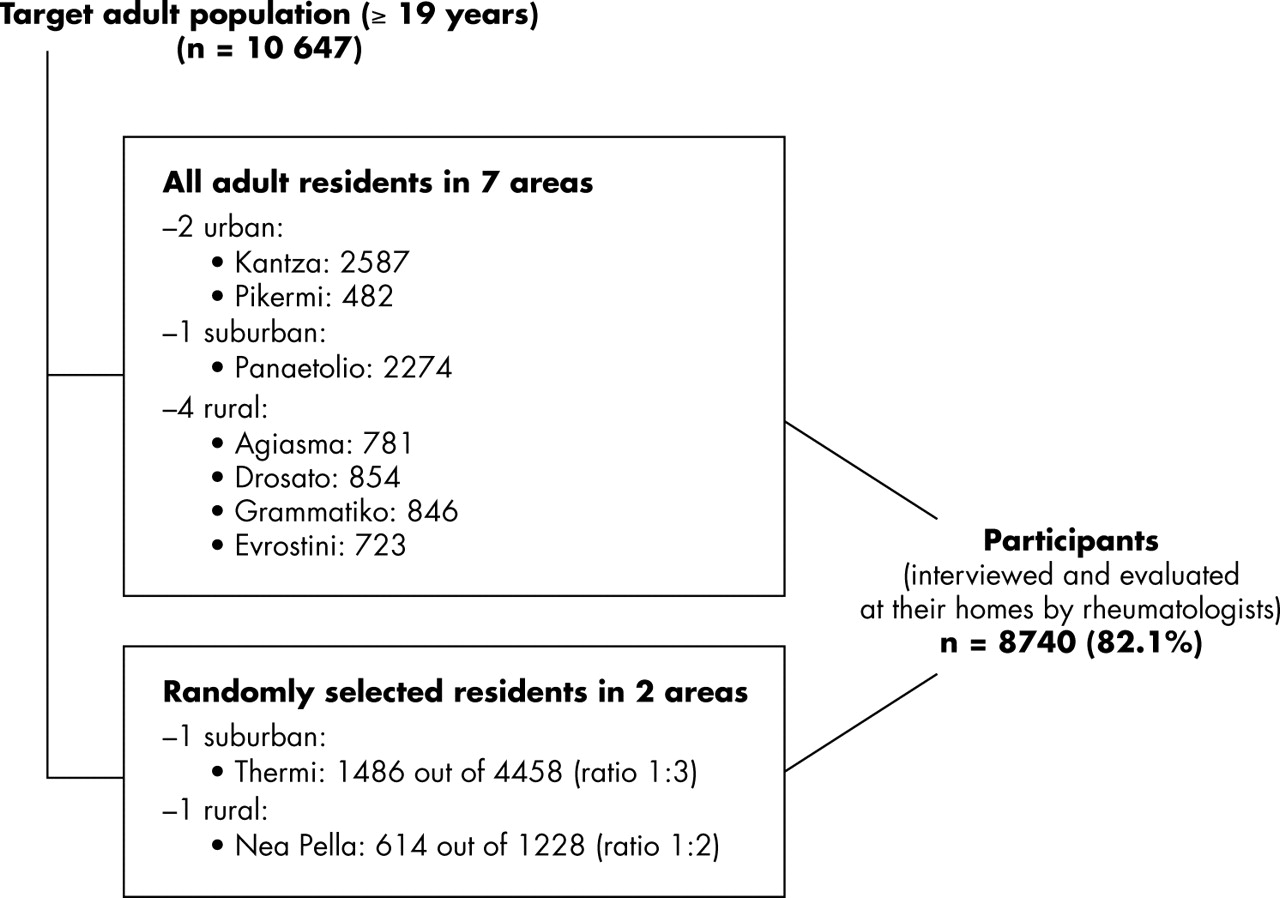
The ESORDIG study was a cross sectional epidemiological study of the rheumatic diseases in Greece (target the adult white population: 10 647 residents; fig 1⇓). The preliminary European (EU) criteria for the classification of pSS were used.2 Subjects who responded positively during the interview to one or more of the three specific questions related to oral symptoms and/or to one or more of the three specific questions related to ocular symptoms were subsequently evaluated by the investigators (medical history, clinical examination, consideration of available laboratory findings). When necessary, procedures for the four objective EU criteria items were carried out until pSS was diagnosed or until three out of the six criteria items were negative. Because the EU-USA consensus group has recently published a revised version of the above criteria, we present our data in accordance with these revised criteria.3
{kind=link}
Flow chart of the ESORDIG study design.
We found 13 patients with pSS (1 man, 12 women, mean (SD) age 55 (16); table 1⇓). Possible cases were not included in our calculations. Thus, the estimate of the age and sex adjusted point prevalence of pSS in both sexes was 0.15%, (95% confidence interval (CI) 0.09 to 0.21) and in the female population 0.29% (95% CI 0.16 to 0.42). The prevalence was higher in the elderly and among residents of urban areas (table 1⇓).
Primary Sjögren’s syndrome cases of the ESORDIG study: patients’ characteristics
Our estimate is lower than that of studies in Manchester (3.3%)4 and in Slovenia (0.60%)5 (both of which used the preliminary EU criteria), and also lower than that of a study in China (0.33% and 0.77%, according to modified San Diego and Copenhagen criteria, respectively).6 Apart from the different sets of criteria used, other methodological differences may be the reason for these discrepancies. The initial phase involving a questionnaire sent by post in some surveys results in a low response rate (37.3–61.6%),4,5 and this is one of the most likely causes of bias. In addition, the population in some of the studies was non-white6 or not exclusively white,4 and genetic differences may influence the results.
We found almost half the prevalence in the female population of that reported in a previous study in a Greek village (0.60%).7 There is no apparent explanation for this discrepancy, although it should be noted that there was an overlapping of the 95% CI between the two studies. The ESORDIG study involved a large sample size, conducted in many dispersed areas around Greece, and the study population was representative of the general adult population of the country.1 There may have been a very slight underestimate in our data, because in a community study it is impossible to determine the, perhaps only few, patients with pSS who fulfilled three of the four objective criteria but who were without oral or ocular symptoms. Nevertheless, our results were close to those in recent reports from Birmingham, UK (0.14% up to 0.40% in the female population)8 and from Izmir, Turkey (0.21% in both sexes),9 both of which used EU-USA criteria. The above may be evidence that the prevalence of pSS in the general white population is lower than previously thought.