Article Text

Statistics from Altmetric.com
Vitamin K is best known for its role in blood coagulation. The reduced form of vitamin K is a necessary cofactor for the γ-carboxylase enzyme that converts specific glutamic acid residues to γ-carboxyglutamic acid (Gla) in the coagulation factors II, XII, IX, X and protein C and protein S.1 Proteins containing one or more Gla residues are often referred to as vitamin K-dependent proteins. The presence of calcium-binding Gla residues is critical to the structure and function of the vitamin K-dependent coagulation proteins. The anticoagulant drugs warfarin and acenocoumarol interfere with the reduction of vitamin K to its active form by inhibiting vitamin K epoxide reductase complex 1 (VKORC1) and so are known as vitamin K antagonists (VKAs).1 These drugs are widely used clinically to treat patients with blood clots or at high risk of blood clots, although newer anticoagulants are available that do not act by inhibiting vitamin K function. These are often referred to as direct oral anticoagulants (DOACs) or non-vitamin K oral anticoagulants (NOACs).
The vitamin K-dependent coagulation proteins are produced primarily in the liver and function within the systemic circulation and vasculature. However, there are a number of vitamin K-dependent proteins not involved in blood coagulation, including several found in joint tissues.2–5 The latter include matrix Gla protein (MGP), Gla-rich protein (GRP) and growth arrest specific gene 6 (Gas6) found in cartilage, the bone proteins bone Gla protein (osteocalcin) and transforming growth factor β (TGFβ)-induced protein, and periostin found in cartilage and the periosteum.5–10 Periostin and TGFβ-induced protein may not be γ-carboxylated in all tissues,11 and their γ-carboxylation status has not been determined in the joint. Although the precise function of the vitamin K-dependent proteins in the joint is not known, MGP and GRP have been shown to inhibit mineralisation, Gas6 promotes chondrocyte survival, and osteocalcin regulates bone turnover. Genetic studies have shown that MGP variants that result in reduced MGP expression are associated with hand and knee osteoarthritis (OA).12–14 MGP knockdown in chondrocytes increased expression of genes related to chondrocyte hypertrophy (type X collagen) and cartilage degradation (MMP-13, ADAMTS4).15 Importantly, when compared with healthy articular cartilage, uncarboxylated MGP and GRP are more abundant in human osteoarthritic articular cartilage suggesting a deficiency in γ-carboxylase activity or decreased availability of reduced vitamin K in OA cartilage.7 8 Mice with the γ-glutamyl carboxylase enzyme deleted in osteoblasts have thicker cortical bone width and increased bone formation,16 a characteristic of the OA joint. In addition, mice aged on a low vitamin K diet were noted to have greater articular cartilage proteoglycan loss than mice aged on a control diet.17 Together, these studies suggest that vitamin K-dependent proteins have a role in maintaining healthy joints (figure 1).
{kind=link}
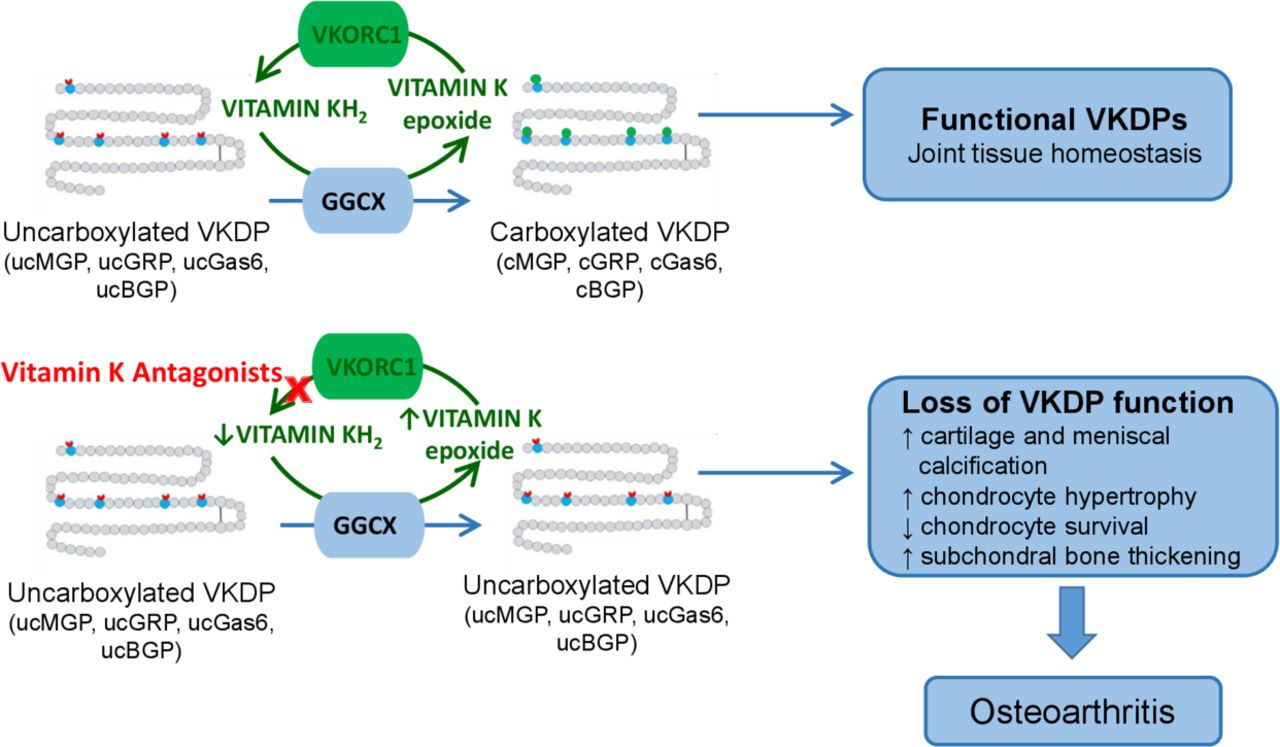
Synthesis and function of vitamin K-dependent proteins (VKDPs) in the joint. The reduced form of vitamin K (KH2) serves as a cofactor for the gamma carboxylase enzyme (GGCX) that post-translationally converts uncarboxylated (uc) glutamic acid residues in VKDPs to form functional γ-carboxylated (c) glutamic acid (Gla) residues. During this process, vitamin KH2 is oxidised to vitamin K epoxide which is reduced by the vitamin K epoxide reductase complex 1 (VKORC1) back to the active vitamin KH2. Vitamin K antagonists function by inhibiting VKORC1 and thus decrease the amount of reduced vitamin K and, in turn, the production of functional Gla-containing VKDPs. These include specific coagulation proteins but also proteins necessary to maintain joint tissue homeostasis including matrix Gla protein (MGP), Gla-rich protein (GRP), growth arrest specific gene 6 (Gas6) and bone Gla protein (BGP, also called osteocalcin).
Additional evidence that vitamin K is important for joint health comes from observational studies examining vitamin K intake and vitamin K blood levels as well as the level of uncarboxylated MGP as a functional measure of vitamin K status. Higher vitamin K intake and/or vitamin K status have been associated with a lower prevalence,18 19 incidence20 and progression of OA.21 Furthermore, low vitamin K status is associated with worse physical performance and more functional decline.22–24 In the Health, Ageing and Body Composition (Health ABC) knee OA study, those with low plasma vitamin K had slower gait speed and worse physical performance battery scores over 4–5 years of follow-up.22 Health ABC participants with low plasma vitamin K also had 1.7- and 2.6- fold higher odds of worsening articular cartilage damage and meniscus damage over 3 years.21 In the Multicenter Osteoarthritis Study (MOST), participants with low plasma vitamin K were 56% more likely to develop radiographic knee OA and had a greater than twofold higher risk of developing MRI-based cartilage lesions over 30 months.20
In Annals of he Rheumatic Diseases, two new studies provide additional compelling evidence for a role of vitamin K-dependent proteins in joint health. Both studies used observational databases to examine the relationship between VKA use and OA and both found a positive association, one by examining acenocoumarol use and risk of incident and progressive knee and hip OA25 and the other examining warfarin use and risk of knee or hip replacement.26 Both studies controlled for age, sex and body mass index, as well as cardiovascular and metabolic factors which might present confounding by indication bias for use of anticoagulants. In addition, the Ballal26 study examined indication bias by including only patients prescribed anticoagulants for atrial fibrillation and by comparing those prescribed warfarin with patients matched for age and sex prescribed a DOAC. The study by Boer et al 25 examined over 4000 participants in the Rotterdam Study and noted that acenocoumarol users had a combined risk of radiographic knee and hip OA incidence and progression of 2.5 (95% CI 1.94 to 3.20) compared with controls not using anticoagulants, while Ballal et al used a UK general practitioner database and noted that compared with treatment with DOACs, individuals with atrial fibrillation prescribed warfarin had a 1.59 times higher risk (95% CI 1.31 to 1.92) of knee or hip replacement.
The study by Boer et al 25 also examined the potential additive effects of MGP and VKORC1 gene variants that would affect the levels of MGP expression, and the dose of acenocoumarol needed for adequate anticoagulation, respectively, and found over a four times higher risk of knee and hip OA incidence and progression in acenocoumarol users who carried both gene variants. It is noteworthy that neither study examined OA pain as an outcome but only radiographic progression or total joint replacement. Although there is no evidence at this time that vitamin K-dependent proteins play a role in regulating pain pathways, at least one of them, osteocalcin, is expressed in sensory neurons.27 So the relationship between VKA use and pain remains an unanswered question.
Although both studies are observational, limiting causal inferences, the results presented in the studies by Boer et al 25 and Ballal et al 26 demonstrating increased OA risk with VKA use, taken together with the prior epidemiologic and biologic studies on vitamin K intake and vitamin K functional status relevant to OA noted above, suggest two important conclusions. First, when prescribing anticoagulant drugs, healthcare providers need to weigh the risk of the potentially harmful effects of the VKA class of anticoagulants on joint tissues that may worsen OA in those already with OA and potentially those at higher risk of OA and decide if, for approved indications, other classes of anticoagulants such as the DOACs (NOACs) would be more appropriate. Second, a randomised clinical trial is needed to determine if individuals with vitamin K insufficiency and OA would benefit from vitamin K supplementation. The only published clinical trial examining the effects of vitamin K supplementation on OA was an ancillary study of hand OA that analysed data from a trial designed to examine vitamin K supplementation for bone loss and vascular calcification.28 Although in a comparison with placebo, randomization to the vitamin K supplement was not associated with a difference in radiographic hand OA, only radiographs taken at the end of the study were available. In a subgroup analysis of participants with insufficient vitamin K levels at baseline, less joint space narrowing was seen in those given vitamin K supplements. A properly powered randomised controlled trial of vitamin K in people with knee or hip OA who are vitamin K insufficient is needed. Given the large number of individuals with OA across the globe, the present studies and future work have important implications for public health.
Acknowledgments
The authors thank Sarah Booth and Kyla Shea for reviewing the editorial and providing helpful comments.
References
Footnotes
Handling editor Josef S Smolen
Twitter @larhumato
Contributors RFL: Data analysis and interpretation; drafting the article; final approval of the version to be published. MK: Data analysis and interpretation; critical revision of the article; final approval of the version to be published. FB: Critical revision of the article; final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; externally peer reviewed.