Article Text

Statistics from Altmetric.com
Rituximab therapy is a promising treatment for primary Sjögren's syndrome (pSS).1 ,2 So far, treatment studies performed in patients with pSS lacked the use of a uniform outcome measure to monitor disease activity.
Recently, the European League Against Rheumatism (EULAR) developed the EULAR Sjögren's Syndrome Disease Activity Index (ESSDAI).3 ESSDAI was shown to be able to monitor disease activity in patient profile and open-label studies.4 ,5 To further study the utility of ESSDAI for clinical studies, we assessed the responsiveness of ESSDAI after rituximab treatment in a randomised controlled trial (RCT) of patients with pSS.6
As the principal investigator (HB) was involved in the development of ESSDAI, the database of a single-centre, randomised, double-blind, placebo-controlled trial (see ref. 6 for details) was prospectively completed with regard to all ESSDAI domains, namely the cutaneous, respiratory, renal, articular, muscular, peripheral and central nervous system, haematological, glandular, constitutional, lymphadenopathy and biological domains. After completion of the RCT, an independent and blinded researcher (RM) assessed the medical records of all included patients (n=30) and calculated ESSDAI at baseline and at 5, 12, 24 and 48 weeks after treatment.
Generalised estimating equations were used to analyse ESSDAI over time within subjects and between treatment groups. Since the residuals were non-normally distributed, ESSDAI was square-root transformed before entering into the equation. Responsiveness of ESSDAI was assessed using standardised response mean (SRM) and effect size (ES).7 SRM and ES <0.5 were interpreted as small, 0.5–0.8 as moderate and >0.8 as large. Statistical analysis was performed with IBM SPSS Statistics 20 (SPSS, Chicago, Illinois, USA). p Values <0.05 were considered statistically significant.
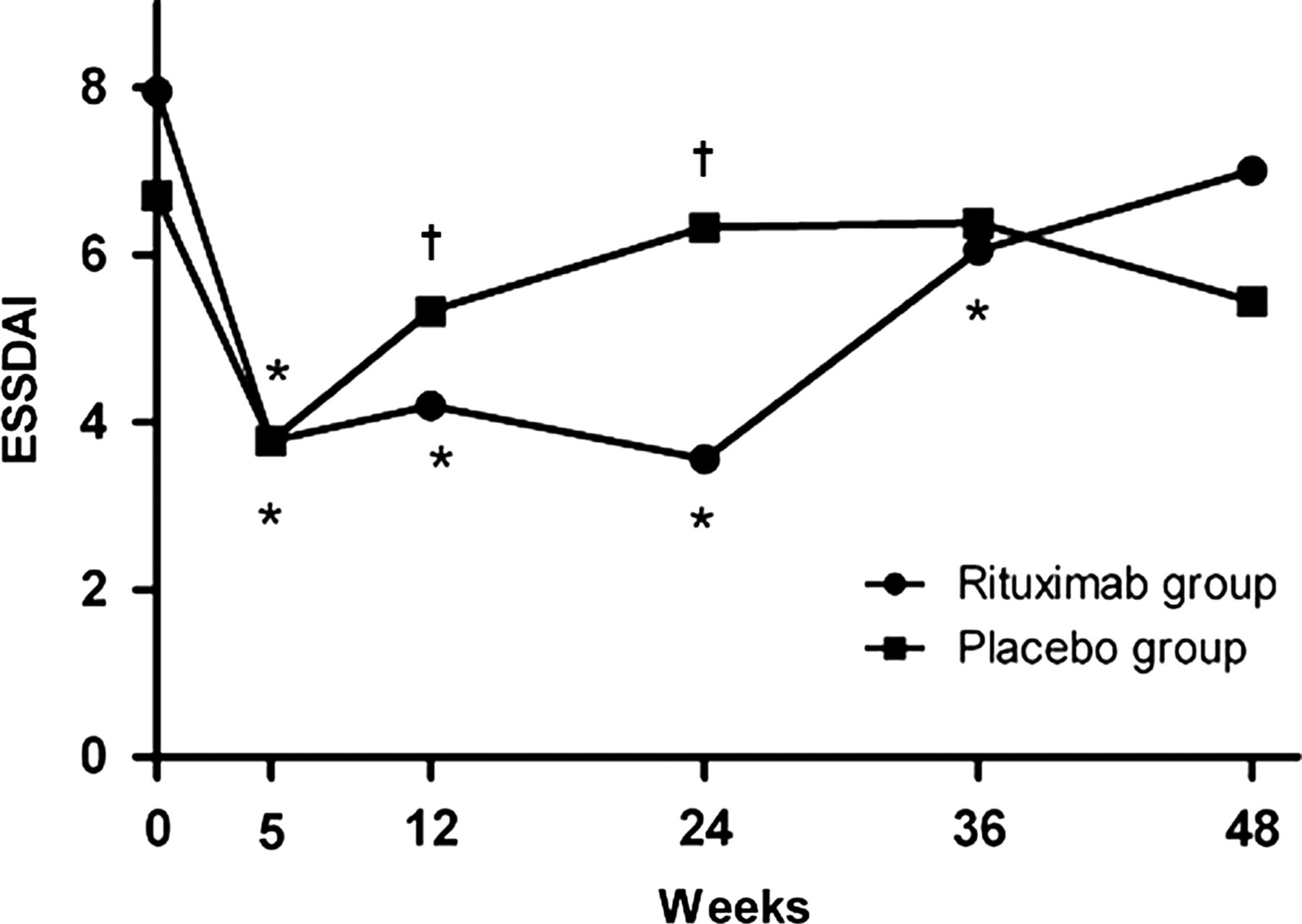
Median (range) ESSDAI at baseline were 8.0 (4–13) and 6.5 (2–13) in the rituximab group and placebo group, respectively. In rituximab-treated patients, ESSDAI improved significantly compared with baseline up to 36 weeks after treatment and had returned to baseline values by week 48. In placebo-treated patients, a significant decrease in ESSDAI was found only at week 5 (figure 1). From 5 to 24 weeks, the evolution of ESSDAI scores over time was significantly different between rituximab-treated and placebo-treated patients. ESSDAI was significantly lower in the rituximab group compared with the placebo group at weeks 12 and 24, which demonstrates the effectiveness of rituximab in reducing disease activity.

{kind=link}
Median European League Against Rheumatism Sjögren's Syndrome Disease Activity Index (ESSDAI) scores of primary Sjögren's syndrome patients treated with rituximab (n=20) or placebo (n=10). *p<0.05 versus baseline. †p<0.05 rituximab versus placebo.
In the rituximab group, SRM and ES for ESSDAI were large at weeks 5–24, moderate at week 36 and small at week 48 (table 1). This indicates that ESSDAI adequately reflects the transient effect of the rituximab with decreasing disease activity up to week 24 and relapse of the disease activity at week 48. In the placebo group, SRM and ES were moderate at week 5 and small at all other time points.
Responsiveness of ESSDAI in pSS patients treated with rituximab (n=20) or placebo (n=10)
The present analysis demonstrates that ESSDAI is able to show significant changes in disease activity in patients with pSS treated with rituximab compared with placebo. These findings confirm the usefulness of ESSDAI for clinical studies, as suggested previously.4 ,5 The high responsiveness of ESSDAI at weeks 5–24 matches the results of changes in clinical and laboratory values, as reported before.6 These parameters returned to baseline values within the same time frame as ESSDAI after rituximab treatment. The significant decrease in ESSDAI as well as the moderate SRM and ES in the placebo group at week 5 are likely due to steroids (100 mg intravenous methylprednisolone, followed by an oral tapering of 2 days 60 mg, 2 days 30 mg and 1 day 15 mg prednisone) administered to minimise side effects of rituximab infusions.6
The large differences in responsiveness of ESSDAI between rituximab and placebo groups show that ESSDAI is a sensitive instrument to assess changes in disease activity over time. Based on the present data, ESSDAI at week 24 seems to be a good end point to assess treatment efficacy of rituximab. Overall, these results support the usefulness of ESSDAI in future clinical trials.
Acknowledgments
We thank J Bulthuis-Kuiper for her contribution to the data collection.
Footnotes
-
Contributors All authors contributed to the conception and design or analysis and interpretation of data, drafting the article or revising it critically for important intellectual content and final approval of the version to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics committee of the University Medical Center Groningen.
-
Provenance and peer review Not commissioned; externally peer reviewed.