Article Text

Statistics from Altmetric.com
Several factors—including immunogenicity—influence pharmacokinetics of adalimumab. The formation of antidrug antibodies (ADAb) leads to lower adalimumab trough concentrations in patients with rheumatoid arthritis (RA) or psoriatic arthritis (PsA),1 ,2 and thus associated with a diminished clinical response.3 A previous paper demonstrated that methotrexate (MTX) had a dose-dependent effect on the percentage of patients that tested positive for ADAb against adalimumab.4 Moreover, prior research has shown that patients with RA concomitantly treated with MTX had higher adalimumab trough concentrations than patients without, which was also dose dependent, resulting in a more frequently achieved European League Against Rheumatism good response status.5 ,6 These studies suggest an additional beneficial effect of concomitant MTX therapy for patients with RA treated with adalimumab. However, in PsA, the benefit of MTX is not yet clear.7 Also, some patients do not tolerate MTX. These patients are either on adalimumab monotherapy or use other concomitant disease-modifying antirheumatic drugs (DMARDs) such as leflunomide, sulfasalazine or hydroxychloroquine. Whether these DMARDs have a comparable effect on adalimumab trough concentrations has, to our knowledge, not yet been studied.
To investigate this, a total of 375 consecutive patients, as described previously (272 patients with RA and 103 patients with PsA), were included from 2004 until 2013 in an observational cohort study at the Jan van Breemen Research Institute|Reade, Amsterdam.2 ,3 Patients started treatment with adalimumab 40 mg every other week. Adalimumab trough concentrations were measured at 0, 4, 16 and 28 weeks of treatment using an ELISA (Sanquin, Amsterdam) as described previously.5 Data were analysed using General Estimating Equation; p values of <0.05 were considered statistically significant. Last observation was carried forward for patients stopping adalimumab therapy prematurely (n=44 RA and n=16 PsA). In addition, in 29 patients (all RA), the dose of adalimumab was increased to 40 mg every week during 28 weeks of follow-up; for these patients, the last available drug concentration before adalimumab dose increase was carried forward.
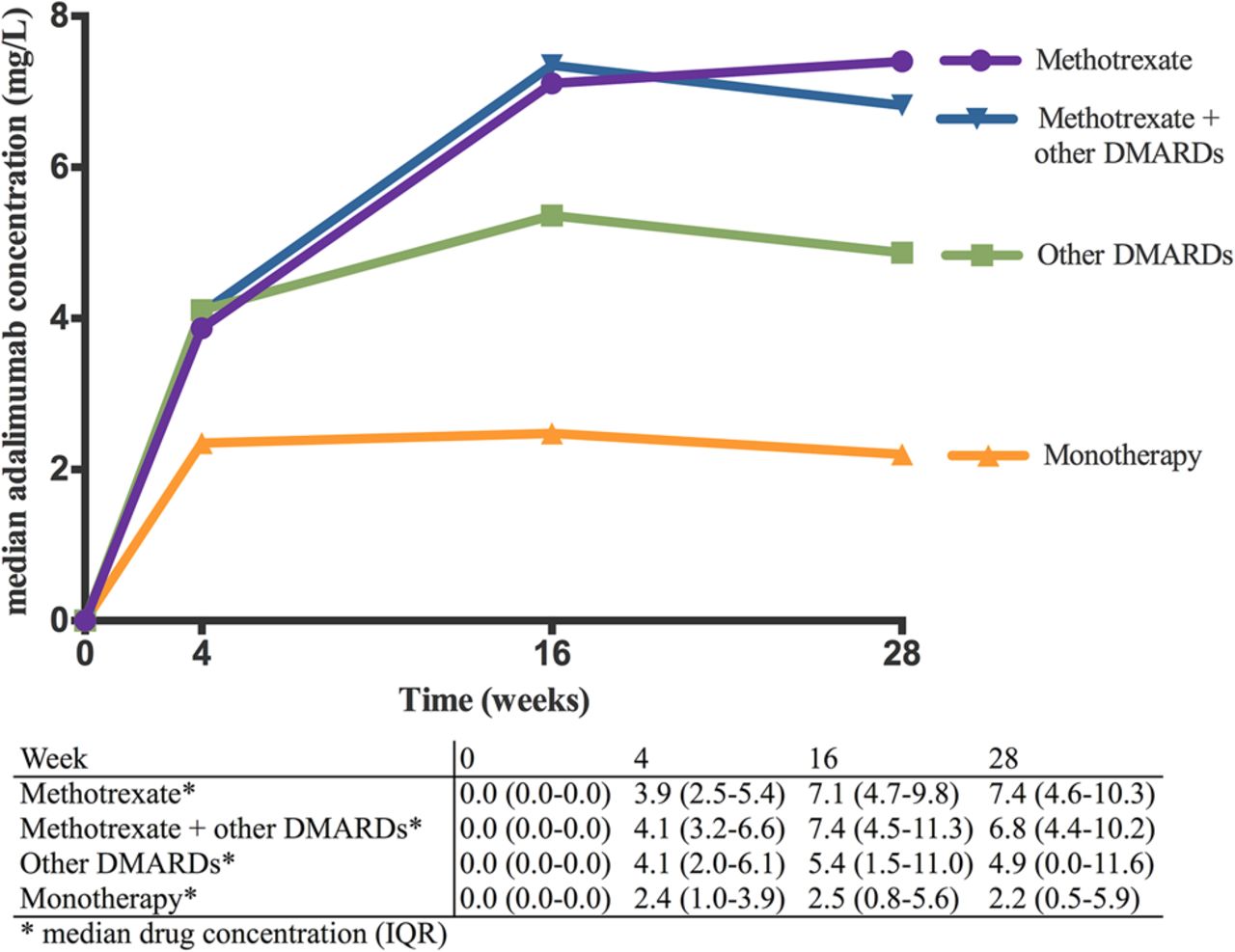
Four groups of adalimumab-treated patients were compared: monotherapy (n=67); concomitant MTX (n=224); concomitant other DMARDs (leflunomide, hydroxychloroquine, sulfasalazine or a combination of these, n=26) and MTX+other DMARDs (n=58). Adalimumab trough concentrations are shown in figure 1. These concentrations were significantly higher in patients with concomitant DMARD treatment compared with monotherapy: monotherapy versus other DMARDs, p=0.011; monotherapy versus MTX, p<0.001; and monotherapy versus MTX+other DMARDs, p<0.001. There was no statistical difference between both MTX groups and the other DMARDs group (p=0.579 (MTX vs other DMARDs) and p=0.352 (MTX+other DMARDs vs other DMARDs)).

{kind=link}
Serum adalimumab trough concentration of patients with rheumatoid arthritis or psoriatic arthritis on adalimumab monotherapy or with concomitant disease-modifying antirheumatic drugs (DMARDs).
In conclusion, adalimumab trough concentrations are the highest in patients concomitantly taking MTX, with or without other DMARDs. Patients on adalimumab monotherapy had the lowest concentrations. Although MTX has the strongest influence on adalimumab trough concentrations, other DMARDs also seem to have a beneficial effect on adalimumab trough concentrations. These results have to be interpreted carefully since only 26 patients were included in the ‘other DMARDs’ group.
These data indicate that in patients intolerant to MTX there might be other options to optimise treatment with adalimumab.
Acknowledgments
This data was presented at the EULAR 2014 congress: Ann Rheum Dis 2014;73(Suppl 2):157. doi:10.1136/annrheumdis-2014-eular.3618).
Footnotes
-
Contributors All authors were responsible for study concept and design, clinical revision and drafting of the manuscript for important intellectual content, and approved the final version of the manuscript to be published. EHV and CLMK were responsible for acquisition of data. EHV, MFP, GW and CLMK were responsible for analysis and interpretation of data. MN and GW obtained funding. GW and CLMK supervised the study.
-
Competing interests MN reports having received consultancy fees from Abbott, Roche, Pfizer, MSD, UCB, SOBI and BMS, payment for lectures from Abbott, Roche and Pfizer. TR reports having received payments for lectures from Pfizer and Abbvie. GJW reports having received a research grant from Pfizer (paid to the institution) and payments for lectures from Pfizer and Amgen. CLMK reports having received payment for lectures from Pfizer and Abbvie.
-
Patient consent Obtained.
-
Ethics approval Medical ethics committee of the Slotervaart Hospital and the Jan van Breemen Research Institute|Reade.
-
Provenance and peer review Not commissioned; externally peer reviewed.