Article Text

Statistics from Altmetric.com
Polyarthropathy associated with human parvovirus B19 (B19) is usually transient, but often resembles rheumatoid arthritis (RA).1-3 However, B19 DNA screened by polymerase chain reaction (PCR) may be positive not only in autoimmune diseases, but also in non-arthropathy.4 To study whether or not RA occurs after acute B19 infection, we conducted a prospective study of patients with acute onset polyarthritis. Sixty seven cases showing acute inflammatory polyarthritis from January 1990 to June 1990 were examined and followed up for six years. Among them, 12 (9 female and 3 male) exhibited IgM anti-B19 antibodies.5 PCR, followed by a Southern blot analysis6 also showed the presence of B19 DNA in all 12 cases with IgM anti-B19 antibodies, but did not in the remainder. Initially, rheumatoid factor (RF) was negative in all B19 positive cases except one, but became positive in four, two to four months after the infection (table 1). Among RF positive cases, three (MI, RM, and TY) developed active polyarthritis with destructive changes in the joints including fingers, wrists or elbows, and rheumatoid nodules. These patients were diagnosed as typical RA fulfilling the 1987 American College of Rheumatology (ACR) criteria for the diagnosis of RA7 as shown in table 2. No cases in the B19 negative group met the ACR criteria for RA during six years of follow up.
Prevalence of joint involvement and RF after the initial episode
Profile of patients who developed RA after acute B19 infection
Figure 1 shows that B19 DNA was no longer detected in blood samples from the patients MI, RM, and TY four months after the initial episodes. It was, however, positive in bone marrow and synovial tissue. Both in situ hybridisation (ISH) and immunofluorescence (IF) study8 ,9 also revealed the presence of B19 DNA/RNA as well as VP-1 antigen in mononuclear cells of bone marrow samples (fig2). Examination of peripheral mononu-clear cells by the stimulation with B19 antigen, showed significantly higher proliferative responses to recombinant VP-1 in patients MI, RM, and TY compared with others (p<0.002).


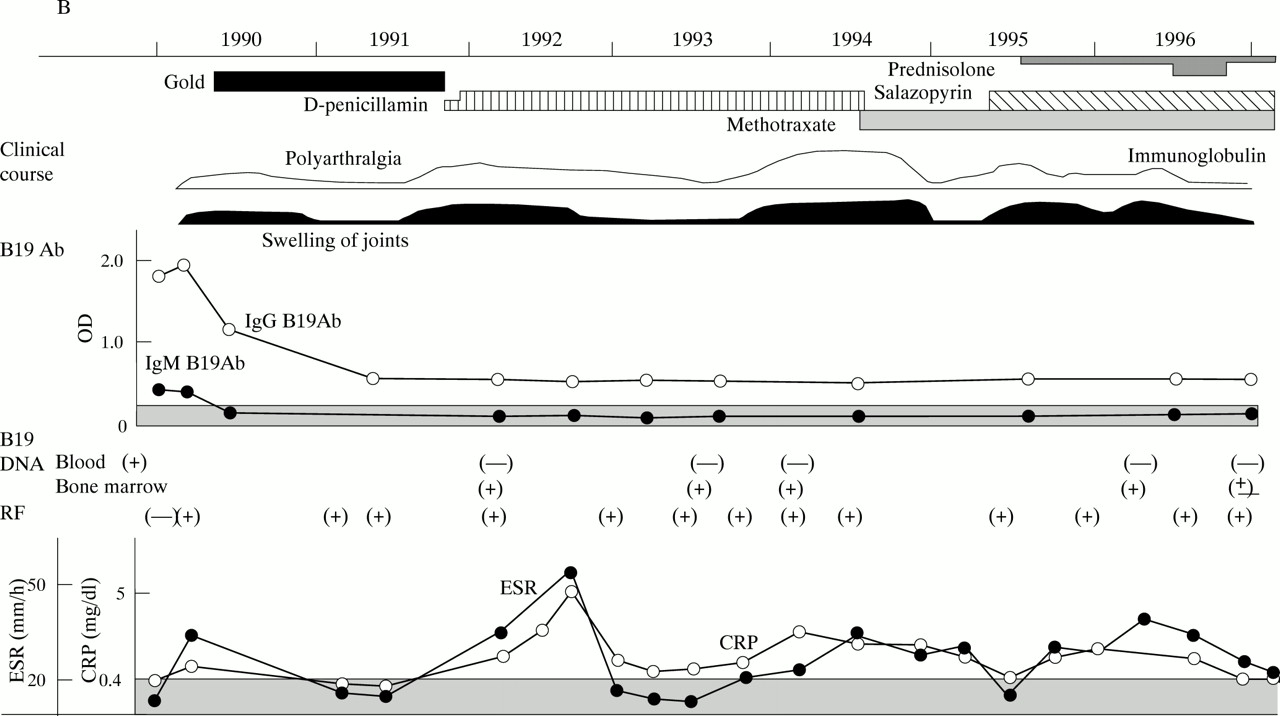
Clinical course of patients MI (A) and RM (B). MTX; methotrexate, CRP; C reactive protein, ESR; erythrocyte sedimentation rate, RF; rheumatoid factor.

{kind=link}
{kind=link}
{kind=link}
B19 DNA/RNA and VP-1 detected by ISH and immunostaining. Bone marrow cells from patient RM (A) or patient KT with anaemia in control group (B) were hybridised with digoxigenin labelled B19 probe, a 480 base pair fragment between nucleotides 590 and 1090 of B19. B19 DNA/RNA positive signals (brown) are indicated by arrows. B19 DNA/RNA in bone marrow cells from patient MI were hybridised with 36S-dCTP labelled B19 probe, a 480 base pair fragment between nucleotides 590 and 1090 of B19 in 1994 (C) and after immunoglobulin therapy in 1995 (D). Bone marrow cells from patient RM in 1993 (E) and patient YK in control group (F) were stained with monoclonal anti-VP-1, PAR 3,8 followed by FITC labelled (Fab)′2 fragments of antimouse γ.
Clinically, three patients with RA were in an active stage and, therefore, treated with a high dose (20 g/day) of gammaglobulin for 10 days (fig 1) after a variety of anti-rheumatic drugs including gold, D-penicillamine or methotrexate became ineffective. The treatment caused a reduction in multiple joint pain and swelling, and a decrease in the C reactive protein value (from 0.8 to 0.3 for patient MI and from 3.6 to 2.0 for patient RM). The number of VP-1 positive cells in bone marrow markedly decreased after the treatment (from 3.6% or 2.6%, to undetectable values or 0.5% in MI and RM respectively).
The prevalence of IgM anti-B19 antibodies in this area was below 0.1% at the time of the study, and so far we have not obtained the evidence of B19 DNA/RNA and VP-1 antigens in the bone marrow samples from patients with haematological diseases, when screened by ISH and IF. The patients in this study developed RA with destructive changes in the joints after acute B19 infection, and had the evidence of persistent activation of B19 in vivo, as demonstrated in a subject with recurrent episodes of B19 infection.10 The decrease of B19 positive cells in bone marrow and their clinical improvement subsequent to intravenous immunoglobulin therapy also supports our view of a relation between B19 infection and polyarthritis, as indicated in the case with a recovery from B19 associated pure red cell aplasia after immunoglobulin therapy.11 Furthermore, the transfection of NS-1 gene of B19 has been shown to induce an increased IL6 production in vitro.12 Our results indicate that B19 should be investigated in association with the aetiopathogenesis of RA.