Article Text

Statistics from Altmetric.com
Detection of antinuclear antibodies (ANAs) is of paramount importance for diagnosis and assessment of autoimmune diseases (ADs), but may vary depending on the method used. Therefore, we aimed to compare three different line immunoassays (LIAs) for ANAs testing in order to simultaneously evaluate their concordance with the results obtained by a well known and widely used ELISA. Sera from women with established systemic lupus erythematosus (SLE, n=62) and Sjogren’s syndrome (SS, n=28) were examined. Patients with SLE had an average age of 48.7 years (IQR 36.8–57.0) with a disease duration of 14.8 years (IQR 9.0–18.0). Patients with SS had an average age of 62.1 years (IQR 55.5–71.0) with a duration of disease of 13.1 years (IQR 8.3–17).
Table 1 shows the results from the two-by-two comparison for the four techniques. Different levels of agreement were observed among the assays. In general, they were deficient. The analysis showed only one ‘strong’ level of agreement between ELISA and IMTEC-ANA-LIA Maxx for anti-Ro measurement. Out of 39 comparisons, 14 did not present any level of agreement, 12 presented a weak agreement and only four had a moderate degree of agreement. ImmcoStripe ANA Advanced LIA was the most discordant technique, showing no level of agreement for 10 out of 21 comparisons performed. The best agreement was between ELISA and IMTEC-ANA-LIA Maxx, with Kappa values above 0.379.
Cohen’s kappa-test comparison among four methods for ANAs detection
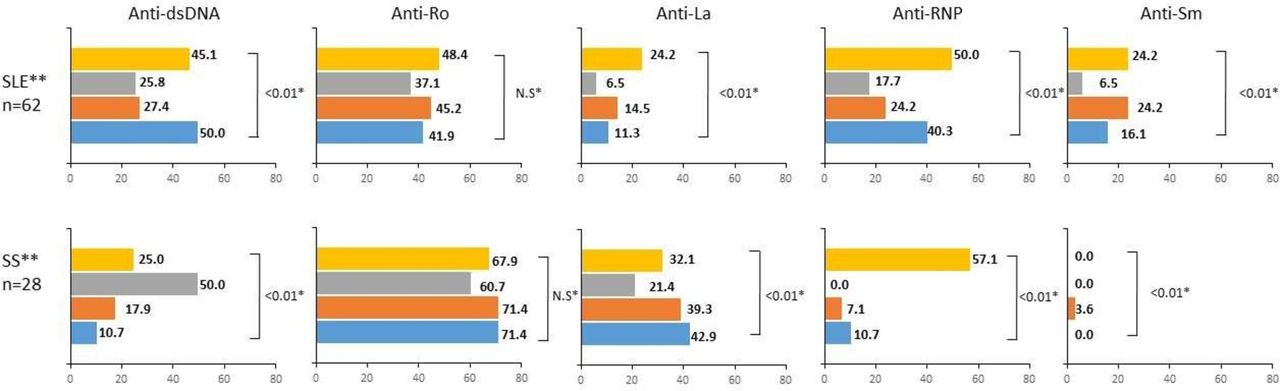
Differences in the substrates and autoantibodies affinity may account for the poor agreement. In patients with SLE, a great discrepancy was observed for anti-Sm frequency which diverged from 6.5% to 24.2% (figure 1, p value<0.01). Antigens used for anti-Sm detection are of different nature in each assay, accounting for such discordance. ELISA uses a native protein extracted from calf, whereas IMTEC-ANA-LIA Maxx uses a synthetic peptide from protein D1; ANA-Profile 23 uses a human extraction enriched with protein D1, and ImmcoStripe ANA Advanced LIA employs a recombinant protein from Escherichia coli. These antigens are all extracted from different sources; thus, they might differ in their post-translational modification, their conformational state and even in their amino acid sequences.

{kind=link}
Frequency of autoantibodies in patients with SLE and SS tested by four different assays. Bars indicate the percentage of positivity of the autoantibody tested by ImmcoStripe ANA Advanced LIA (yellow), Ana-Profile 23 (grey), IMTEC-ANA-LIA Maxx (orange) and ELISA (blue). Frequencies were very heterogeneous among the different assays. Only for anti-Ro detection, the frequencies measured were not statistically different among the four tests. For the three LIAs, anti-Ro frequencies represent the cumulative frequencies for anti-Ro52 and anti-Ro60. For ImmcoStripe ANA Advanced LIA, anti-RNP bar represents the cumulative values for anti-U1snRNPC, anti-U1snRNPA and anti-U1snRNP68. *Differences in proportion of positivity among the assays were evaluated by Q-Cochran test. Values shown represent the p value. **Patients fulfilled the American College of Rheumatology classification criteria for SLE8 and the American College of Rheumatology/European League Against Rheumatism classification criteria for primary SS.9 ANA, antinuclear antibody; LIA, line immunoassay; RNP, ribonucleoprotein; SLE, systemic lupus erythematosus; SS, Sjogren’s syndrome; NS, not significant.
Anti-Ro detection was the most convergent antibody among the four assays, presenting a strong agreement between ELISA and IMTEC-ANA-LIA Maxx. Even though the target antigen employed in these two assays is different, the agreement was more than 90%. Indeed, ELISA has a native Ro antigen with both proteins Ro52 and Ro60 combined, whereas IMTEC-ANA-LIA Maxx has the purified native Ro60 in one band and a recombinant Ro52 in another one. Among the other assays for Ro detection, agreement was variable with percentages higher than 63%, regardless of the antigen employed.
Discordances have already been described when comparing other autoantibodies testing methodologies, such as ANAs screening by indirect immunofluorescence assay through different kits or among different laboratories1 2 ; ELISAS versus LIAs3 and LIAs from three different manufactures.4 5 In our study, the confirmation performed for anti-dsDNA antibodies by Crithidia luciliae indirect immunofluorescence test (CLIIFT) resulted disappointing, since the level of agreement between the four assays and the ‘gold standard’ technique did not surpass the ‘minimal’ level. In fact, out of 22 sera positive for anti-dsDNA by ELISA, only seven were positive by CLIIFT, confirming ELISA as highly sensitive but less specific than CLIIFT.6 As mentioned, different populations of anti-DNA antibodies due to affinities of the targeted antibodies for dsDNA and substrate differences account for such discrepancies.
Due to the huge heterogeneity in the results, further efforts to standardise autoantibodies detection techniques need to be performed, emphasising in homogenisation of the antigens preparation allowing reproducibility of both population of patients and at individual patient level.
Footnotes
Handling editor Josef S Smolen
Contributors YP, DMM, YAA, JMA and CRS contributed to the design, the analysis of the results and to the writing of the manuscript. YP, DMM, YAA, CR and CRS performed the experiments.
Funding This work was supported by the Universidad del Rosario, grant number IV-FBG001.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Universidad del Rosario.
Provenance and peer review Not commissioned; internally peer reviewed.