Article Text

Statistics from Altmetric.com
Golimumab, a fully humanised antitumour necrosis factor (anti-TNF)-α monoclonal antibody, has been proven effective in the treatment of both rheumatoid arthritis (RA)1 and ankylosing spondylitis (AS).2 As with other anti-TNF-α inhibitors, golimumab may elicit antidrug antibodies (ADAb), leading to pharmacokinetic changes.3 ,4 With the limited data regarding the immunogenicity of golimumab,1 ,2 ,5 we aim to evaluate the relations among ADAb, serum drug trough levels, therapeutic response and methotrexate (MTX) dosage in golimumab-treated patients.
We initially enrolled 78 biologic-naïve patients who started golimumab therapy at a dosage of 50 mg given subcutaneously once a month. Two patients with AS were lost to follow-up due to skin reactions at the 2nd and 3rd month, respectively. Hence, the remaining 76 patients (33 RA and 43 AS) completed the 24-week treatment course, and were eligible for this study. Serum ADAb levels and drug trough levels were determined at week 24 of golimumab therapy by bridging ELISA and capture ELISA (Progenika Biopharma SA, Derio, Spain), respectively, a modified version of the method used in our previous study.6 A positive ADAb result was defined as a titre >30 arbitrary unit/mL in combination with a golimumab level <5.0 μg/mL. Because all of the enrolled patients were biologic-naïve at the start, their ADAb results before starting golimumab were all presumed to be negative. For the patients with RA, the disease activity and clinical improvement were assessed with DAS28 change and European League Against Rheumatism (EULAR) response. Meanwhile, the Ankylosing Spondylitis Disease Activity Score (ASDAS) and ≥50% improvement in the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI50) were measured in the patients with AS. Blood samples were obtained immediately before golimumab injection at week 24. The ethics committee of our hospital approved this study (CE12205-2), and the written consent was obtained from each participant (table 1).
Baseline demographic data, clinical characteristics and laboratory findings in patients with RA and AS receiving 24 weeks of golimumab therapy†
Our results showed that the proportion (15.2%, 5/33) of ADAb positivity in patients with RA was higher than that (2.1%–8.1%) in other studies.1 ,5 ,7 The possible reasons for this discrepancy included the lower proportion of patients coreceiving MTX therapy, the relatively low MTX dosage, the difference in assays used and the lower sample size in this study. Regarding the drug immunogenicity in AS, ADAb was detectable in only one (2.3%) patient, consistent with previous findings that 4.1% of patients with AS developed ADAb.2 Because the bridging ELISA used in this study cannot detect ADAb in the presence of drug, the drug interference may result in underestimation of ADAb-positivity rate.
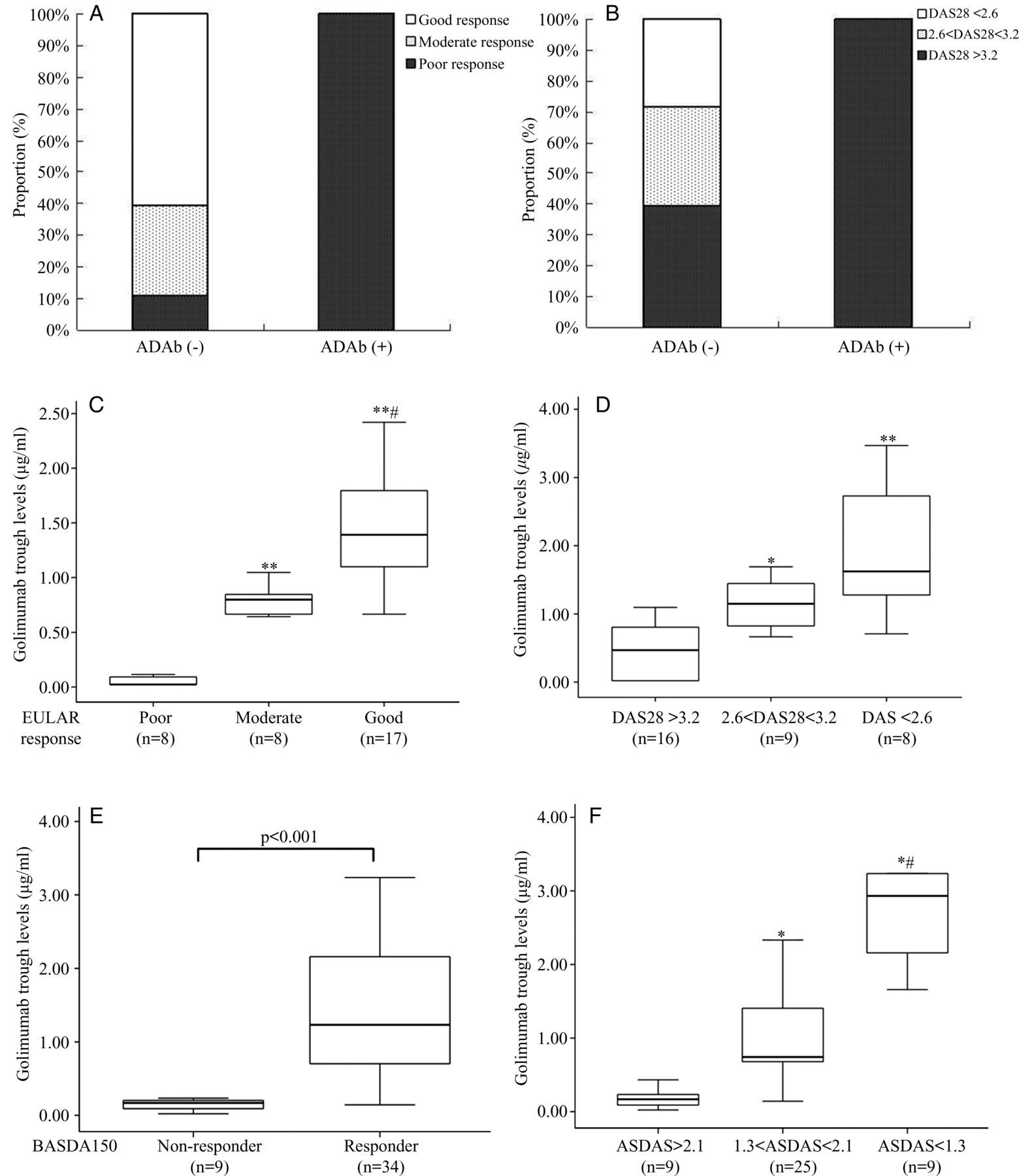
As in other reports,5 ,6 ,8 ,9 our patients with ADAb-positive RA had barely detectable golimumab levels (median=0.022 μg/mL, IQR 0.020–0.022 μg/mL) in contrast with patients who were ADAb negative (median=1.05 μg/mL, IQR 0.69–1.45 μg/mL, p<0.001). Besides, patients who were ADAb positive had significantly higher rates of poor EULAR response or persistent active disease (DAS28>3.2) after 24-week golimumab therapy compared with patients who were ADAb negative (100% vs 10.7%, p<0.001; 100% vs 39.3%, p<0.05, respectively, figure 1A, B).
{kind=link}
The association of antidrug antibodies (ADAb) with EULAR therapeutic responses (A) and with disease activity assessed using DAS28 (B). Comparison of drug trough levels among patients with RA with different EULAR responses (C) and disease activity status achieved at week 24 of golimumab therapy (D). Comparison of drug trough levels between patients with AS with and without BASDAI50 response (E) and disease activity status (ASDAS) achieved at week 24 of golimumab therapy (F). The data were presented as box-plot diagrams, with the box encompassing the 25th percentile (lower bar) to the 75th percentile (upper bar). Good responders were defined as patients who had a decrease in DAS28 from baseline (ΔDAS28)>1.2 and a DAS28 ≤3.2 at evaluation time; moderate responders had either ΔDAS28 >1.2 and a DAS28 >3.2 or ΔDAS28 of 0.6–1.2 and a DAS28 ≤5.1 at evaluation time; and poor responders were those who had either ΔDAS28 <0.6 or a DAS28 >5.1 at evaluation time. In RA patients: #p<0.005, versus moderate EULAR response; *p<0.005, **p<0.001, versus poor EULAR response or persistent active disease (DAS28>3.2). In AS patients: #p<0.005, versus moderate disease activity (1.3≦ASDAS<2.1); *p<0.001, versus high disease activity (ASDAS>2.1). AS, ankylosing spondylitis; ASDAS, Ankylosing Spondylitis Disease Activity Score; BASDAI50, ≥50% improvement in the Bath Ankylosing Spondylitis Disease Activity Index; EULAR, European League Against Rheumatism; RA, rheumatoid arthritis.
Also in consistence with other studies,5 ,6 ,8 serum golimumab levels were significantly associated with therapeutic response (figure 1C, D) and clinical improvement (ΔDAS28) (r=0.594, p<0.001) in patients with RA. Serum golimumab levels were also associated with therapeutic response (BASDAI50) and ASDAS status in patients with AS (figure 1E, F). Interestingly, we demonstrated that golimumab levels were positively correlated with MTX dosages (r=0.566, p<0.005), supporting the pharmacokinetic findings that MTX treatment increased drug levels by approximately 0.6 μg/mL3 and could reduce golimumab clearance by 17.1%.3 ,4
In conclusion, ADAb positivity was significantly associated with low golimumab levels and poor therapeutic response. MTX contributes to reducing golimumab clearance, an effect that is likely mediated by the known impact of MTX on ADAb development. The positive correlation between drug levels and therapeutic response indicates that drug monitoring could be useful for optimising the dosing of biologics in a personalised therapy strategy.6 ,10
Acknowledgments
The authors thank the Biostatistics Task Force of Taichung Veterans General Hospital, Taichung, Taiwan.
References
Footnotes
Y-MC, W-TH and H-HC contributed equally.
Contributors All authors made substantive intellectual contributions to the present study and approved the final manuscript. D-YC conceived of the study, generated the original hypothesis, designed the study, acquired clinical data, analysed data, drafted and revised the manuscript. Y-MC, W-TH and H-HC contributed equally to this work, conceived the study, acquired clinical data, analysed data and drafted the manuscript. C-WH, Y-HC, W-NH and T-YH performed clinical assessments and data acquisition, statistical analysis and drafted the manuscript.
Funding This work was supported by a grant (TCVGH 1037305C) from Taichung Veterans General Hospital.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Institutional Review Board of Taichung Veterans General Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.