Article Text

Abstract
Background: It has previously been shown that IgG antibodies from patients with limited cutaneous systemic sclerosis (SSc) bind to specific microvascular endothelial cell antigens. Since patients with limited cutaneous SSc are prone to develop pulmonary arterial hypertension (PAH), and since endothelial cell activation is involved in the pathogenesis of idiopathic PAH (IPAH), a study was undertaken to examine the presence of anti-endothelial cell antibodies in patients with idiopathic or SSc associated PAH.
Methods: PAH was confirmed by right heart catheterisation (mean pulmonary artery pressure at rest >25 mm Hg). Serum IgG and IgM reactivities were analysed by immunoblotting on human macrovascular and microvascular lung and dermal endothelial cells from patients with IPAH (n = 35), patients with PAH associated with SSc (n = 10), patients with diffuse (n = 10) or limited cutaneous (n = 10) SSc without PAH, and 65 age and sex matched healthy individuals.
Results: IgG antibodies from patients with IPAH bound to a 36 kDa band in macrovascular endothelial cell extracts with a higher intensity than IgG from other patient groups and controls. IgG antibodies from patients with IPAH bound more strongly to a 58 kDa band in microvascular dermal endothelial cells and to a 53 kDa band in microvascular lung endothelial cells than IgG antibodies from other patients and controls. IgG antibodies from patients with limited cutaneous SSc with or without PAH, but not from other groups or from healthy controls, bound to two major bands (75 kDa and 85 kDa) in microvascular endothelial cells.
Conclusion: IgG antibodies from patients with idiopathic or SSc associated PAH express distinct reactivity profiles with macrovascular and microvascular endothelial cell antigens.
- AECA, anti-endothelial cell antibodies
- BMPR-II, bone morphogenetic protein receptor type II
- HUVEC, human umbilical vein endothelial cells
- HMVEC-d, human microvascular dermal endothelial cells
- HMVEC-l, human microvascular lung endothelial cells
- IPAH, idiopathic pulmonary arterial hypertension
- PAH, pulmonary arterial hypertension
- SSc, systemic sclerosis
- pulmonary arterial hypertension
- systemic sclerosis
- anti-endothelial cell antibodies
Statistics from Altmetric.com
- AECA, anti-endothelial cell antibodies
- BMPR-II, bone morphogenetic protein receptor type II
- HUVEC, human umbilical vein endothelial cells
- HMVEC-d, human microvascular dermal endothelial cells
- HMVEC-l, human microvascular lung endothelial cells
- IPAH, idiopathic pulmonary arterial hypertension
- PAH, pulmonary arterial hypertension
- SSc, systemic sclerosis
Pulmonary arterial hypertension (PAH) is a rare disease with an incidence rate of one per million in the general population which represents a major cause of progressive right sided heart failure leading to premature death.1 It is defined by increased mean pulmonary artery pressure above 25 mm Hg at rest resulting from chronic obstruction of small pulmonary arteries caused by endothelial and vascular smooth muscle cell dysfunction and proliferation.2
PAH may be idiopathic (IPAH)—either sporadic, familial, or associated with dexfenfluramine therapy.1 It may also be associated with connective tissue diseases such as systemic sclerosis (SSc),3 mixed connective tissue diseases, and systemic lupus erythematosus. Approximately 14% of SSc patients develop PAH, which is responsible for a high mortality rate.3
The recent identification of germline mutations of genes coding for members of the transforming growth factor β (TGF-β) receptor family, the bone morphogenetic protein receptor type II (BMPR-II) in sporadic and familial PAH, focused much attention on the role of cytokines and growth factors in these disorders.4,5 However, no BMPR-II mutations have been detected in patients with SSc, suggesting that other mechanisms could be involved in PAH associated with SSc.6 Indeed, in addition to abnormal TGF-β signalling, altered expression and production of several cytokines and growth factors have been found in severe PAH, highlighting the possible influence of inflammatory mechanisms in this condition.2 Furthermore, the prevalence of anti-endothelial cell antibodies (AECA) in patients with SSc varies from 44% to 84%.7–9 Several studies have indicated that AECA are associated with a higher incidence of vascular manifestations.9,10 We have previously defined more precisely the specificities of those antibodies. IgG AECA from patients with diffuse SSc are common to microvascular and macrovascular endothelial cells and correspond to topoisomerase 1, whereas IgG from patients with limited cutaneous SSc bind to an 80 kDa protein band in microvascular endothelial cells only.11 Since the activation of endothelial cells mediated by AECA can be involved in the pathogenesis of PAH in patients with SSc, we analysed the activities of AECA in patients with PAH associated with SSc and in patients with IPAH.
METHODS
Patients
Patients were screened by Doppler echocardiography and PAH was defined as systolic pulmonary artery pressure >40 mm Hg. PAH, confirmed by right heart catheterisation in all patients, was defined as mean pulmonary artery pressure at rest >25 mm Hg. Sixty five patients were included in the study, comprising 35 with IPAH (20 with sporadic PAH, 10 with dexfenfluramine associated PAH, and five with familial PAH), 10 with SSc associated PAH (SSc-PAH), 10 with limited cutaneous SSc without PAH, and 10 with diffuse SSc without PAH. Patients with limited cutaneous and diffuse SSc fulfilled the criteria of LeRoy and Medsger12 and the American Rheumatism Association,13 respectively. Disease duration was significantly longer in SSc patients than in patients with IPAH (table 1). All patients with diffuse SSc without PAH had interstitial lung disease as assessed by chest high resolution computed tomodensitometry and a vital capacity <80% of predicted values and/or a gas transfer factor of <75% of predicted values. None of the patients was receiving corticosteroids or immunosuppressants and none had cancer or other connective tissue disease. Sixty five unrelated age and sex matched healthy donors were studied as controls. All patients gave their written informed consent.
Clinical and immunological characteristics of patients with IPAH and those with SSc with or without PAH
Ig sources
Serum samples from all patients and healthy controls were aliquoted and stored at −80°C until tested. IgG and IgM antibody concentrations, determined by nephelometry, did not differ significantly (table 1). Three of the 35 IPAH patients had low titres of antinuclear antibodies, whereas five of 10 patients with SSc with PAH and all the patients with SSc without PAH had antinuclear antibodies. A therapeutic preparation of normal human IgG, intravenous immunoglobulin, IVIg (Tegeline, Laboratoire du Fractionnement Biologique et des Biotechnologies (LFB), Les Ulis, France) and normal human polyclonal IgM (LFB) served as internal standards.
Cell culture
Human umbilical vein endothelial cells (HUVEC) were obtained by digestion of umbilical cords with 0.1% collagenase (Sigma, St Louis, MO, USA) as described previously.14 They were cultured in 199 Earle’s salts and HEPES medium (Life Technologies Ltd, Auckland, NZ) supplemented with 20% heat inactivated fetal calf serum (FCS), 2 mM l-glutamine, 100 U/ml penicillin, 100 µg/ml streptomycin, and 0.25 µg/ml amphotericin B at 37°C in 5% CO2. When confluent, the cells were detached using 0.05% trypsin, 2 µM EDTA. After the third passage a HUVEC protein extract was prepared. Human microvascular dermal endothelial cells (HMVEC-d) and human microvascular lung endothelial cells (HMVEC-l) were purchased from Clonetics Corporation (San Diego, CA, USA) after four passages. They were cultured with microvascular endothelial cell growth medium containing 5% FCS, 0.04% hydrocortisone, 0.1% vascular endothelial growth factor, 0.1% human recombinant insulin-like growth factor 1, 0.4% ascorbic acid, 0.1% human epidermal growth factor, and 0.1% GA-1000 (gentamicin sulfate and amphotericin B) (EGM-2-MV Bulletkit, Clonetics Corporation). The endothelial cell phenotype of the three types of cultured cells was confirmed by their typical growth in cobblestone monolayers and labelling of von Willebrand factor by a specific polyclonal rabbit antibody (Dako, Glostrup, Denmark).
Detection of antibody reactivities with nuclear antigens
Anti-centromere and anti-topoisomerase 1 antibodies were detected by indirect immunofluorescence on HEp-2 cells and double immunodiffusion in agar against calf thymus extract, respectively.
Detection of antibody reactivities with cell antigens
Antibody reactivities were analysed using a semi-quantitative immunoblotting technique with normal human endothelial cells and HEp-2 cells. Cellular protein extracts were performed in a buffer containing 4% SDS, 1.45 M 2-mercaptoethanol, 125 mM Tris/HCl pH 6.8, 1 µg/ml aprotinin, 1 µg/ml pepstatin, and 1 µg/ml leupeptin and then sonicated 4×30 s. Equal amounts of solubilised proteins were subjected to preparative SDS-polyacrylamide gel electrophoresis (PAGE) through 10% polyacrylamide gels. The proteins were then transferred onto nitrocellulose membrane for 1 hour at 0.8 mA/cm2 using a semi-dry electroblotter model A (Ancos, Hojby, Denmark). After blocking with PBS-0.2% Tween for 90 minutes, the membranes were incubated with serum samples for 4 hours at room temperature at 200 µg/ml IgG or 20 µg/ml IgM in a Cassette Miniblot System (Immunetics Inc, Cambridge, MA, USA). They were then extensively washed before being incubated with either secondary rabbit anti-human Fcγ or Fcµ antibody coupled to alkaline phosphatase (Dako) for 90 minutes at room temperature. Immunoreactivities were revealed using the nitroblue tetrazolium/5-bromo-4-chloro-3-indolyl-phosphate (NBT/BCIP) substrate (Sigma). Immunoreactivities were quantified by scanning the membranes with a densitometer (Epson Perfection 1200S, Seiko Epson Corporation, Nagano-Ken, Japan). The membranes were then stained with colloidal gold (Protogold, Biocell, Cardiff, UK) and subjected to a second densitometric analysis to quantify transferred proteins. This approach allows the immunoreactivity repertoires to be compared by referring to their respective protein peaks corrected for electrophoretic migration defects by superimposing corresponding protein peaks by means of computer analysis. Standard IgM or IgG preparations were included in each blot to allow the rescaling of the membranes transferred with a given protein extract and to adjust for the intensity of labelling on different membranes.11,14 All experiments were performed twice.
Statistical analyses
Because of the large number of reactivities identified in the blots, the data were submitted to multivariate statistical analysis using IGOR software (Igor Pro 3.16, Wavemetrics Inc, Lake Oswego, OR, USA) with specially designed packages and Systat software (Version 11.0, Systat Software, Point Richmond, CA, USA). Densitometry curves of IgG and IgM reactivities of each patient and control were divided into sections surrounding individual peaks of immunoreactivity on each substrate; 8–10 sections were selected, depending on the protein extract used and number of antibody reactivities identified in the blots. The number of comparisons performed was limited on the basis of clinical relevance and five comparisons were performed for IgG and for IgM reactivities: PAH patients v healthy controls; IPAH patients v healthy controls; IPAH patients v SSc-PAH; SSc-PAH v SSc patients without PAH; and SSc-PAH patients v healthy individuals. In order to compare groups of individuals (groups of patients two by two and patients v controls), for each comparison we calculated the factor scores of each of the subjects after performing factor analysis of the whole data of patients and healthy controls. Factor analysis was performed using the principal component analysis as a method of extraction and factors with eigenvalues >1 were retained.15 Independent factors were obtained using the varimax rotation method. Factor scores of each of the individuals for the retained factors were submitted either to a paired Wilcoxon test to compare the patterns of reactivity of patients to age and sex matched healthy controls, or to a Mann-Whitney test to compare the patterns of reactivity of patients two by two. One to six protein bands made important contributions to the calculation of factors of the factor analysis. The molecular weights of the protein bands contributing to the different factors varied according to the source of antigens tested and the two groups compared.
RESULTS
Serum anti-HUVEC IgG reactivities
The patterns of reactivity of serum IgG antibodies with HUVEC antigens were generally homogeneous in healthy individuals and among patients in each group. However, IgG antibodies from a few individuals in each group bound to a unique band with a higher intensity than IgG antibodies from others. IgG from all healthy individuals and patients in each group bound to one major 36 kDa protein band (figs 1 and 2, table 2). This band was more marked by serum IgG antibodies from patients with IPAH than by serum IgG antibodies from the other disease groups or from healthy controls (fig 2). In addition, IgG antibodies from 17 of the 35 patients with IPAH, but not from other patient groups or healthy controls, bound to a 60 kDa protein band (fig 2, table 2).
Serum IgG reactivities of patients with IPAH, patients with SSc with or without PAH, and healthy individuals with endothelial and HEp-2 cell antigens

Western blotting of IgG with protein extracts of human umbilical vein endothelial cells (HUVEC). Serum IgG from patients with IPAH, SSc-PAH, limited cutaneous SSc without PAH, and age and sex matched healthy controls was immunoblotted at 200 µg/ml with a soluble extract of HUVEC. Normal human polyclonal IgG (intravenous immunoglobulins) and secondary anti-Fcγ antibody tested alone were used as positive and negative controls, respectively.

Densitometric profiles of IgG reactivity of 10 healthy individuals, 10 patients with IPAH, 10 with SSc-PAH, 10 with limited cutaneous SSc (lSSc) without PAH, and 10 with diffuse SSc (dSSc) without PAH with human umbilical vein endothelial cell (HUVEC) antigens. Serum samples were diluted to an IgG concentration of 200 µg/ml. The densitometric pattern of IgG reactivities of each individual is depicted as a full line curve. Grey areas depict the densitometric pattern observed in the presence of the secondary anti-Fcγ antibody alone. Molecular weights are expressed as kDa in the abscissa and optical densities are expressed as arbitrary units (AU) in the ordinates.
Serum anti-HMVEC-d and HMVEC-l IgG reactivities
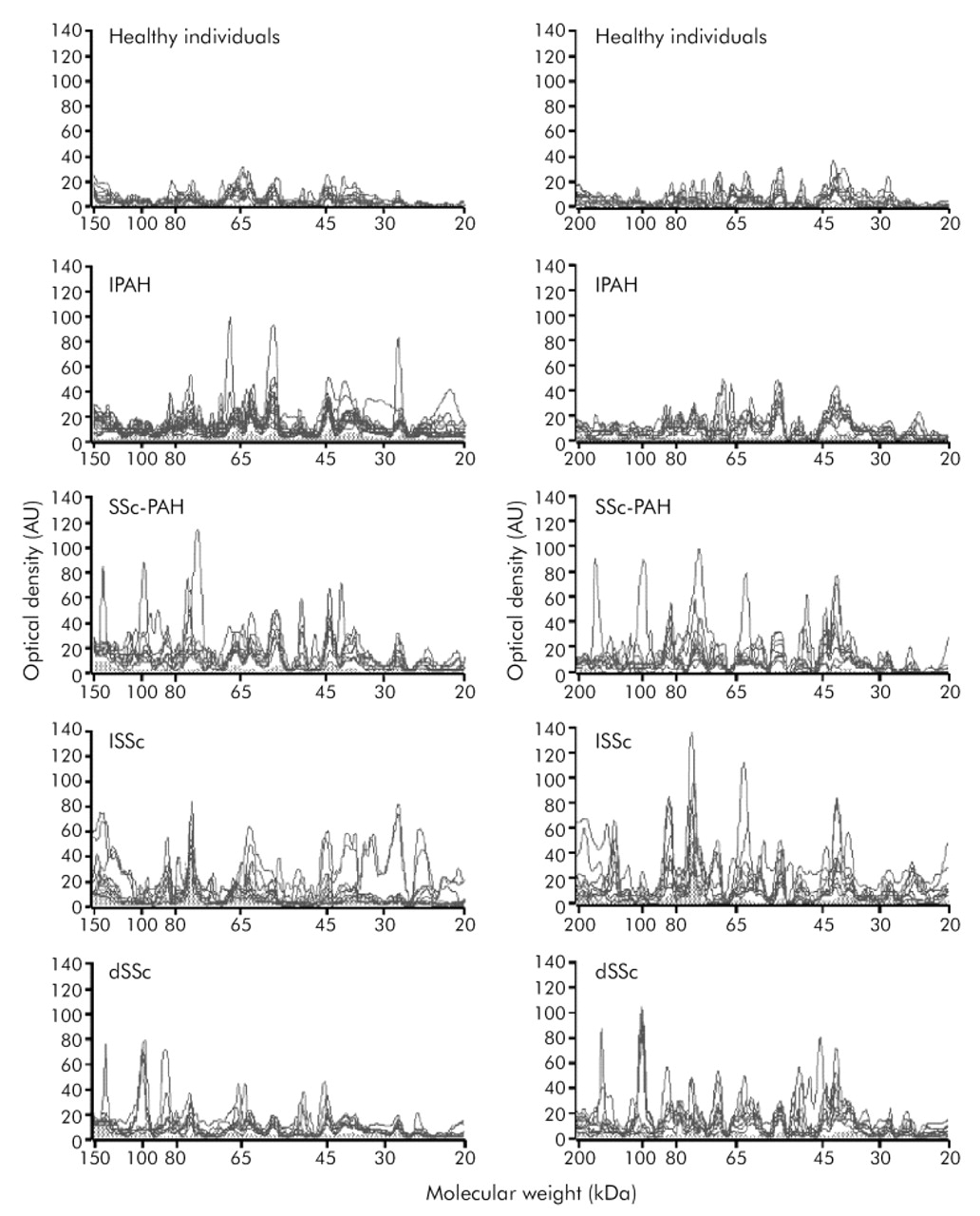
As observed with HUVEC, the patterns of reactivity of IgG antibodies with HMVEC-d and HMVEC-l antigens were generally homogeneous among healthy individuals and in patients with IPAH (fig 3). A 58 kDa protein band in HMVEC-d and a 53 kDa protein band in HMVEC-l extracts were more intensely revealed by IgG antibodies from IPAH patients than by IgG antibodies from controls and patients in other groups. IgG antibodies from SSc-PAH patients and from patients with limited cutaneous SSc without PAH bound to two major protein bands of 75 and 85 kDa that were not recognised by IgG antibodies from other patients or healthy controls. Finally, IgG antibodies from patients with diffuse SSc without PAH bound to a 100 kDa protein band that was not recognised by IgG antibodies from healthy individuals and other patients.

{kind=link}
{kind=link}
{kind=link}
Densitometric profiles of IgG reactivity of 10 healthy individuals, 10 patients with IPAH, 10 with SSc-PAH,10 with limited cutaneous SSc (lSSc) without PAH, and 10 with diffuse SSc (dSSc) without PAH with HMVEC-d (left panels) and HMVEC-l (right panels) antigens. Serum samples were diluted to an IgG concentration of 200 µg/ml. The densitometric pattern of the IgG reactivities of each individual is depicted as a full line curve. Grey areas depict the densitometric pattern observed in the presence of the secondary anti-Fcγ antibody alone. Molecular weights are expressed as kDa in the abscissa and optical densities are expressed as arbitrary units (AU) in the ordinates.
Serum anti-HEp-2 cell IgG reactivities
In order to document the endothelial cell specificity of IgG reactivities, additional experiments were performed using a protein extract of HEp-2 cells, a reference substrate for the identification of antinuclear antibodies. Healthy individuals and patients with IPAH expressed a low number of reactivities, with one major IgG reactivity directed toward a 45 kDa protein band (table 2). In contrast, SSc patients in the different groups expressed a large number of IgG reactivities with two major protein bands of 75 and 85 kDa in SSc-PAH patients and those with limited cutaneous SSc without PAH, and one major protein band of 100 kDa in patients with diffuse SSc (table 2 and fig S1 available online only at http://www.thoraxjnl.com/supplemental)
Comparison of factor scores of serum anti-endothelial cell and anti-HEp-2 cell IgG reactivities
Patients with PAH (IPAH and SSc-PAH) differed significantly from healthy individuals for IgG reactivity with HMVEC-l and HMVEC-d and HEp-2 cell extracts, with the exception of factor 2 (75 and 77 kDa) on HMVEC-l, factor 3 on HEp-2 cells, and HUVEC for all factors (table 3). Interestingly, serum IgG from SSc-PAH patients did not differ from those of healthy controls, with the exception of factor 3 of the factor analysis on HEp-2 cells which corresponded to reactivities at 28 kDa and 45 kDa (table 3).
Comparison of factor scores of serum anti-endothelial and anti-HEp-2 cell IgG and IgM reactivities from patients with PAH and their respective controls
IgG reactivities from SSc-PAH patients were compared with those of patients with IPAH and those of patients with SSc without PAH. No significant difference was found between IPAH and SSc-PAH patients for IgG reactivities with the different sources of antigens tested, with the exception of factor 4 on HMVEC-d and factor 2 on HEp-2 cells, with a 58 kDa band contributing to both factors (table 4). No significant difference was found between SSc-PAH patients and SSc patients without PAH for reactivity with the different sources of antigens tested, with the exception of factor 1 on HMVEC-d (table 4).
Comparison of factor scores of serum anti-endothelial and anti-HEp-2 cell IgG and IgM reactivities from IPAH patients and SSc patients with or without PAH
Serum anti-endothelial cell IgM reactivities
IgM reactivity patterns with HUVEC antigens were relatively homogeneous among healthy individuals, IPAH patients, and those with limited cutaneous SSc and diffuse SSc, with 5–7 reactivities including one major reactivity directed toward a 55 kDa protein band (table 5). IgM from healthy individuals and patients with diffuse SSc without PAH bound to 9–12 protein bands in HMVEC-l and HMVEC-d protein extracts, including one major reactivity directed towards a 65 kDa protein band (table 5). IgM from IPAH patients, SSc-PAH patients, and patients with limited cutaneous SSc without PAH strongly bound to two additional major protein bands of 32 and 48 kDa (table 5), whereas IgM from other patients and controls bound to those bands with low intensity. Similar results to those obtained with HMVEC-l antigens were obtained when testing IgM reactivity patterns of patients and controls against HMVEC-d antigens (fig S2, available online only at http://www.thoraxjnl.com/supplemental).
Serum IgM reactivities of patients with IPAH, SSc with or without PAH, and healthy individuals with endothelial cell antigens
Comparison of factor scores of serum anti-endothelial cell and anti-HEp-2 cell IgM reactivities
IgM reactivities of patients in each group did not differ from those of controls for reactivity with all sources of antigens tested with the exceptions of patients with PAH on factors 2 (63, 68 kDa) and 3 (130 kDa) and SSc-PAH patients on factor 1 on HUVEC antigens (table 3). IgM reactivities from patients in the different groups were then compared two by two. IgM reactivities from SSc patients with PAH and SSc patients without PAH did not differ significantly except for factor 3 of the factor analysis on HUVEC (table 4). A 130 kDa peak contributed the most to this factor. IgM reactivities from IPAH patients and SSc patients with PAH did not differ significantly, whatever the source of antigens tested (table 4).
DISCUSSION
In this study we found that patients with IPAH express specific patterns of IgG reactivity with HUVEC, HMVEC-d and, to a lesser degree, with HMVEC-l and HEp-2 cell antigens, whereas IgG antibodies from patients with SSc with or without PAH bind to HMVEC-d, HMVEC-l and HEp-2 cell proteins but not to HUVEC proteins, although the difference did not reach significance.
To our knowledge, AECA have not been detected previously in patients with IPAH. In many patients with PAH disorganised proliferation of endothelial cells is observed, leading to the formation of plexiform lesions.16 Endothelial dysfunction leads to chronically impaired production of vasodilators, nitric oxide, and prostacyclin, together with overexpression of vasoconstrictors such as endothelin-1, resulting in the narrowing of the pulmonary arterial lumen and endothelial cell proliferation. Stimuli known to promote abnormal endothelial proliferation include hypoxia, shear stress, inflammation, and response to drugs or toxins in genetically susceptible individuals.
AECA have been detected in SSc patients with limited cutaneous or diffuse SSc,7–9 particularly in patients with vascular manifestations such as PAH and digital ischaemia9,10 and in patients with pulmonary fibrosis.17 Using a systematic approach, we have recently shown that IgG antibodies from patients with limited cutaneous or diffuse SSc, with or without anti-topoisomerase 1 antibodies, exhibit specific and mutually exclusive reactivity patterns.11 These results led us to speculate that autoantibodies from these SSc patients specifically bind to different types of endothelial cells and support the classification of AECA according to disease specific target endothelial cells proposed by Praprotnik et al.18
AECA target antigens comprise a wide range of extracellular matrix proteins19 and molecules that adhere to endothelial cells, such as DNA in systemic lupus erythematosus,20 β2-glycoprotein I or phospholipids21 in anti-phospholipid syndrome, myeloperoxidase22 or proteinase 323 in primary systemic vasculitides, and α-enolase in Behcet’s disease.24 Until recently, in patients with SSc none of the AECA target antigens had been identified but some molecular weights have been determined. Ihn et al17 found that AECA from patients with SSc bind to target cytoplasmic antigens of 60, 90, 110, and 140 kDa.17 Hill et al reported that antibodies directed to a 19 kDa protein, associated with limited cutaneous SSc, expressed anti-centromere activity. This observation led them to postulate that these AECA might trigger inflammation of endothelial cells in connective tissue diseases.8,25 Finally, we recently identified DNA topoisomerase 1 as a 100 kDa endothelial cell target for IgG antibodies from patients known to express anti-topoisomerase 1 antibodies as assessed by other techniques.11 In a recent study IgG AECA from patients with diffuse SSc consistently recognised HMVEC-d but only 50% of them bound to HUVEC.26
Very few studies are available in the literature regarding the antigens specifically expressed by endothelial cells. To our knowledge, the only published proteomic analysis of human endothelial cells focused on quiescent HUVEC and identified 53 proteins of suspected endothelial origin.27 In addition to cytoskeleton proteins, proteins involved in cellular mobility, regulation of apoptosis, and senescence have been identified, as well as proteins implicated in clotting or antigen presentation, but we could not find any data on the characterisation of microvascular specific endothelial cell antigens. Our results lead us to infer that some endothelial cell antigens are expressed by microvascular endothelial cells and others such as HEp-2 cells, but not by macrovascular endothelial cells.
Reactivities detected by immunoblotting reflect the specific binding of the various regions of IgM and IgG antibodies to tissue antigens.28 Since the profiles of reactivity were homogeneous among patients in each group and in healthy controls, despite the use of the same endothelial cell sources to test all patients, it is highly improbable that these reactivities reflect alloreactivities.
This study provides evidence, for the first time, that patients with IPAH and PAH associated with SSc express AECA. The target antigens and the potential pathogenetic role of these antibodies remain to be determined. The predictive value of these antibodies in patients at risk of developing PAH, such as SSc patients and those with a familial history of PAH, needs to be investigated.
Acknowledgments
The authors thank Dr Frédéric Batteux who provided the HEp-2 cells and Dr Michèle Uzan who provided normal human umbilical cords.
REFERENCES
Footnotes
-
This work is supported by a grant from the Université Paris Nord (Bonus Qualité Recherche), INSERM (CReS #4CR08F), the Association des Sclérodermiques de France and the Legs POIX, Chancellerie des Universités, Académie de Paris, France. The study was supported in part by the French Network of Pulmonary Arterial Hypertension. M C Tamby is a recipient of a grant from AMPLI (Avenir Mutualiste des Professions Libérales & Indépendantes); Y Chanseaud was funded by the Ministère de l’Enseignement Supérieur et de la Recherche, France and the Laboratoire Français du Fractionnement et des Biotechnologies (LFB); P Garcia de la Peña-Lefebvre received a grant from the Association Claude-Bernard, France; A Servettaz received financial support from the Direction Régionale de l’Action Sanitaire et Sociale de la région Champagne-Ardennes, France.
-
Competing interests: none declared.
-
This work has been presented at the 3rd Annual Meeting of the Federation of Clinical Immunology Societies (FOCIS), 15–19 May 2003, Paris, France; at the 4th Annual Congress of the European League Against Rheumatism (EULAR), 19–21 June 2003, Lisbon, Portugal; and at the 67th ACR/ARHP Annual Scientific Meeting, 24–28 October 2003, Orlando, Florida, USA.