Article Text

Abstract
Background Exercise is considered important in the management of patients with rheumatic diseases, but the effect of high intensity exercises on disease activity is unknown.
Objective To investigate the effectiveness of high intensity exercises on disease activity in patients with axial spondyloarthritis (axSpA).
Method Assessor blinded multicentre randomised controlled trial. 100 patients (aged from their 20s to their 60s) with axSpA were randomly assigned to an exercise group or to a no-intervention control group. The exercise group performed cardiorespiratory and muscular strength exercises at high intensity over 3 months. The control group received standard care and was instructed to maintain their usual physical activity level. Primary outcome was disease activity measured with the Ankylosing Spondylitis (AS) Disease Activity Scale (ASDAS, higher score=worst) and the Bath AS Disease Activity Index (BASDAI, 0–10, 10=worst). Secondary outcomes were inflammatory markers, physical function and cardiovascular (CV)-health. There was patient involvement in the design and reporting of this study.
Results 97 of the 100 (97%) randomised patients completed the measurements after the intervention. There was a significant treatment effect of the intervention on the primary outcome (ASDAS: −0.6 [–0.8 to –0.3], p<0.001 and BASDAI: −1.2 [–1.8 to –0.7], p<0.001). Significant treatment effects were also seen for inflammation, physical function and CV-health.
Conclusion High intensity exercises reduced disease symptoms (pain, fatigue, stiffness) and also inflammation in patients with axSpA. It improves patients’ function and CV health. This debunks concerns that high intensity exercise might exacerbate disease activity in patients with axSpA.
Trial registration number NCT02356874.
- exercise
- exercise rehabilitation
- randomised controlled trial
Statistics from Altmetric.com
Introduction
Axial spondyloarthritis (axSpA) is a chronic inflammatory rheumatic disease affecting people at young age with a prevalence of 0.3%–1.4%.1 The leading features of the disease are inflammatory back pain, reduced joint mobility and disability.1 Furthermore, during the last decade increasing evidence has shown that inflammatory rheumatic diseases also are associated with an increased risk of cardiovascular (CV) diseases.2
Exercise is an important part of the management for patients with inflammatory rheumatic diseases,3 and low dose (frequency, Intensity, time and type) exercises are commonly used to relieve pain and increase joint mobility.4 5 High intensity exercise has been largely eschewed by clinicians in this field as some experts raised concerns that high intensity exercises may flare-up disease activity.6–8 However, particularly as people living with axSpA have high risk of CV disease,9 cardiorespiratory and strength exercises (which also have CV disease risk-reducing potential),10 should be evaluated as a treatment option for this patient group.
Exercise has a small beneficial effect on disease activity in patients with inflammatory rheumatic disease.4 5 11 12 However, we feel the studies included in those meta-analyses had exercise programmes of relatively low dose. Our innovation was to examine the effects of a 12 weeks high intensity cardiorespiratory and strength exercise programme on disease activity and CV-health in patients with axSpA.
Methods
Design
The exercise for spondyloarthritis (ESPA)-study was designed as a 3 month assessor-blinded two-armed multicentre randomised controlled trial (RCT) comparing the effects of 12 weeks of high intensity exercises with standard care (non-intervention). The trial was conducted at rheumatology departments, three in Norway (Diakonhjemmet Hospital, Martina Hansen Hospital and the University Hospital of North Norway), and one in Sweden (Sahlgrenska University Hospital). All procedures followed the Declaration of Helsinki.
Participants
Patients were recruited from outpatient rheumatology departments as well as through advertisement in various social media-channels. Pre-screening was administered by telephone. The inclusion criteria were fulfilment of the Assessment of SpondyloArthritis International Society (ASAS) criteria for axSpA,13 age 18–70 years, no change in tumor necrosis alpha (TNF)-inhibitor use during the last 3 months, moderate to high disease activity at pre-screening (Bath ankylosing spondylitis (AS) Disease Activity Index (BASDAI)≥3.5),14 and not performed regular cardiorespiratory or strength exercises (>1/week the last 6 months). Exclusion criteria were established or symptoms of CV disease (online supplementary file 1), other comorbidity involving reduced exercise capacity, inability to participate in supervised sessions and pregnancy.
Supplementary file 1
Exercise intervention
The exercise programme (online supplementary file 2) followed the American College of Sports Medicine recommendations for cardiorespiratory and muscular strength exercises15 and lasted for 12 weeks. Two times per week the sessions were supervised by a physiotherapist and consisted of high intensity cardiorespiratory16 and strength exercises. In addition, the exercise group performed an individual cardiorespiratory exercise session once a week. In total, the intervention group had three training sessions per week. The supervised sessions took place either at the hospital, or at a fitness centre. The physiotherapists were experienced clinicians in rheumatology and were trained in the exercise protocol through participation in workshops. As a general rule, some pain (≤5 on a scale from 0 to 10) was tolerated during the exercises. However, if the pain got worse the day after, the exercises were adapted. The control group received standard care and was asked to maintain their usual physical activity level.
Supplementary file 2
Registration of adherence and safety
Exercise adherence was recorded by the physiotherapist and was also self-reported in an exercise diary, and the highest number of completed sessions was registered. The control group did not record exercise, but were asked about exercise habits during the intervention period retrospectively in a questionnaire.
Safety was considered as absence of disease flare-ups after the intervention period, and was defined in terms of stable or decreased disease activity (Ankylosing Spondylitis Disease Activity Score [ASDAS] and BASDAI), and acute phase reactants (C reactive protein [CRP] and erythrocyte sedimentation rate [ESR]). Further, measures of safety included adverse events reported by the physiotherapists.
Outcomes
Outcomes were assessed at baseline and immediately after the intervention and included questionnaires addressing demography, comorbidities, medical and general health and physical activities, a clinical examination and blood samples. A physiotherapist (SHS) blinded to group allocation conducted the clinical examination at all four study centres and it was performed in the following order; measurement of resting HR and blood samples, followed by flexibility measurements and finally the treadmill test.
Primary outcome
The primary outcome was disease activity assessed by ASDAS and BASDAI. The ASDAS has been recommended for assessing disease activity in patients with axSpA since it was launched17 and the BASDAI has been used for many years in clinical practice and in research,14 and therefore both were included as primary outcome measures. The ASDAS is a composite score of CRP and four patient reported variables, all reported on a 11-point numeric rating scale (NRS): (1) neck/back/hip pain, (2) peripheral joint pain, (3) duration of morning stiffness and (4) patient global assessment. Cut-offs are defined as inactive disease <1.3, low disease activity 1.3–2.1, high disease activity 2.1–3.5 and very high disease activity >3.50.18 The BASDAI is a patient reported index of five symptoms (fatigue, neck-back-hip pain, peripheral joint pain, tenderness and degree/length of morning stiffness).14 Each question was answered on an 11 point NRS, and a sum score from 0 to 10 (10=worst) was calculated.
Secondary outcome measures
Physical function was assessed with the Bath AS Functional Index (BASFI), which is a disease specific index of 10 questions answered on an 11 point NRS, and a sum score from 0 to 10 (10=worst) was calculated.19 Spinal mobility was assessed by the Bath AS Metrology Index (BASMI), including five measurements of spinal mobility.20 The scores range from 0 to 10, with the mean of the five scores producing a BASMI-score from 0 to 10 (10=worst).
Cardiorespiratory fitness was assessed with a maximal test on a treadmill involving walking uphill until exhaustion according to the modified Balke protocol (online supplementary file 3). Based on the workload at the end of the test, peak oxygen uptake (VO2peak mL/kg/min) was estimated.21 Estimating VO2peak from a maximal test is considered the next most accurate test for cardiorespiratory fitness after direct measurement of VO2peak.22 However, it is reported to overestimate.21
Supplementary file 3
Muscle mass was measured with a whole body dual-energy X-ray absorptiometry (DXA) scan of lean body mass. DXA is recognised as a validated reference method for assessment of lean body weight23 and was available at two study centres.
Body weight was measured in light clothing to the nearest 0.1 kg, body height was self-reported and body mass index (BMI) (kg/m2) was calculated. Waist circumference was measured with a measuring tape at the height of umbilicus in a supine position.
Blood samples were drawn after at least 4 hours fasting and analysed for CRP and ESR according to current procedures at the study centres. Resting HR was assessed after at least 5 min in supine position.
The ASAS20/40 was used to calculated improvement.24 ASAS20 is defined as a relative improvement of ≥20% and an absolute improvement of ≥1 unit in at least three of the four following domain; patient global assessment, pain, physical function and morning stiffness, and no worsening of ≥20% and ≥1 unit in the remaining domains. ASAS40 response is defined as a relative improvement of ≥40% and an absolute improvement of ≥2 unit in at least three of the four domains that are defined for ASAS20, and no worsening at all in the fourth domain.24
Sample size
The estimation of sample size was based on a pilot study showing a mean treatment effect of 0.7 points in the ASDAS score.25 Further, in a cross-sectional study, the SD of the ASDAS score was found to be 1.0.26 With 80% power and a 5% significant level, we estimated non-compliance to be 10% and the drop-out rate to be 20%. Based on this, we calculated that 100 patients were needed.
Randomisation and blinding
The randomisation sequence was computer generated by a statistician, and concealed for the assessor. The randomisation was stratified according to the study clusters and a block randomisation with a block size of four was used to ensure adequate number of patients in the exercise group. Allocation was administered after baseline testing by the physiotherapist who supervised the exercises in order to keep the outcome assessor blinded for group allocation. All clinical examinations were performed by an assessor unaware of the group assignment. Blinding of the participants and the physiotherapist supervising the exercise sessions was not possible. The main statistical analyses were performed blinded to group allocation.
Patient involvement
Three patient representatives from the patient panel at DS participated in regular workshops during the accomplishment of this RCT. They were involved in development of research questions, choice of outcome measures, the recruitment process and implementation of the trial. We presented our preliminary results to patients' representative and discussed them before the results were written up.
Statistical analyses
Baseline characteristics were summarised using mean and SD or frequency and percentages. The main statistical analyses were performed on the intention-to-treat (ITT) population. Analysis of covariance (ANCOVA) on the post-intervention values was used to assess the group differences with p values, mean difference and 95% CI. Baseline values and study centre were included as covariates. Normality assumptions of the ANCOVA models were assessed by pp-plots of the residuals. The residuals for ESR and CRP were not normally distributed, and group differences in change from baseline were analysed with the Mann-Whitney U test.
For continuous variables, the standardised mean difference (SMD) with 95% CI was calculated based on final scores for each group at 3 months using Review Manager V.5.3 software. SMDs between 0.2 and 0.4 are considered as a small effect size, from 0.5 to 0.7 as a medium effect size, and ≥0.8 as a large effect size.27
Absolute increased benefit (AIB) was calculated as the difference in the proportion of participants achieving 20% and 40% ASAS improvement criteria. In addition, the number of patients who must be treated in order to obtain the benefit of interest in one additional patient (numbers needed to treat [NNT]) was calculated. AIB and NNT with 95% CI were calculated using GraphPad.28
A per protocol analysis on patients in the exercise group that followed ≥80% of the exercise protocol and patients in the control group that exercised ≤1 per week were also evaluated for all outcomes.
Statistical analyses were performed using SPSS V.21. P values <0.05 were considered statistically significant.
Results
Participants
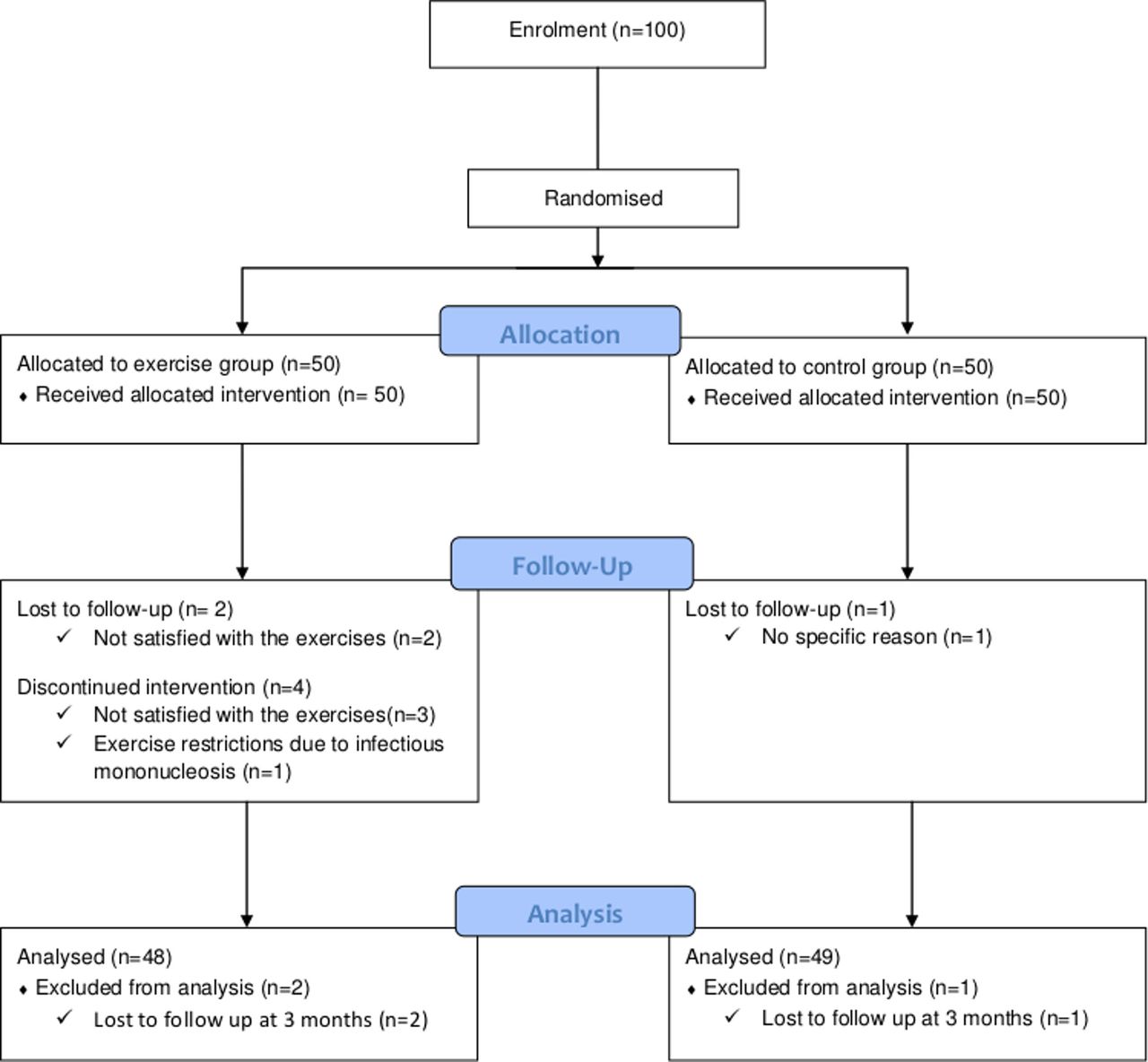
A total of 100 patients with axSpA were included between August 2015 and September 2016 (figure 1). Three patients were lost to follow-up, hence 97 (97%) of the randomised patients are included in the analyses. There were no significant differences between the groups in personal or disease characteristics at baseline (table 1).
Baseline descriptive of all patients, the exercise group and the control group
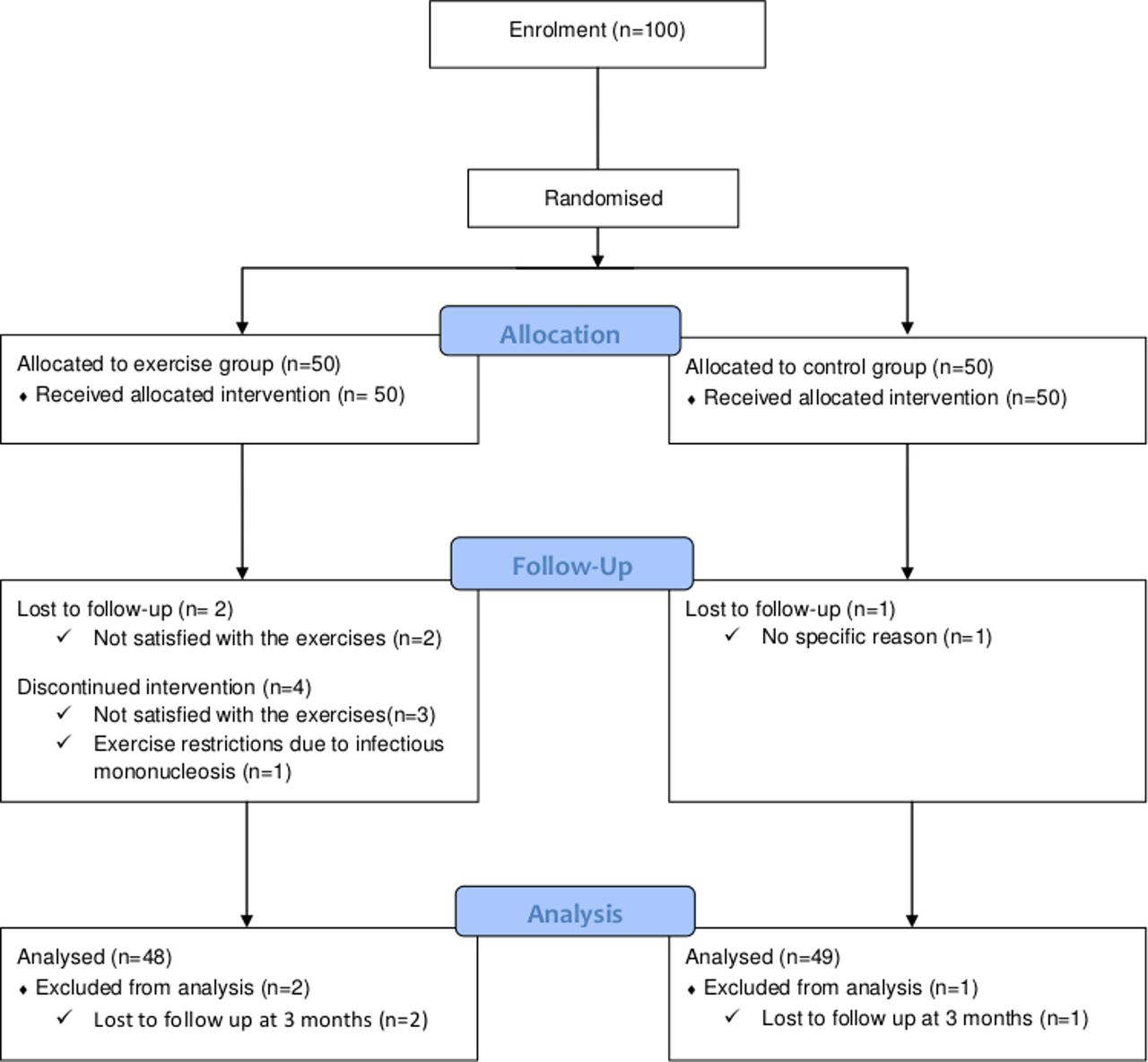
Flow of participants throughout the trial.
Primary outcomes
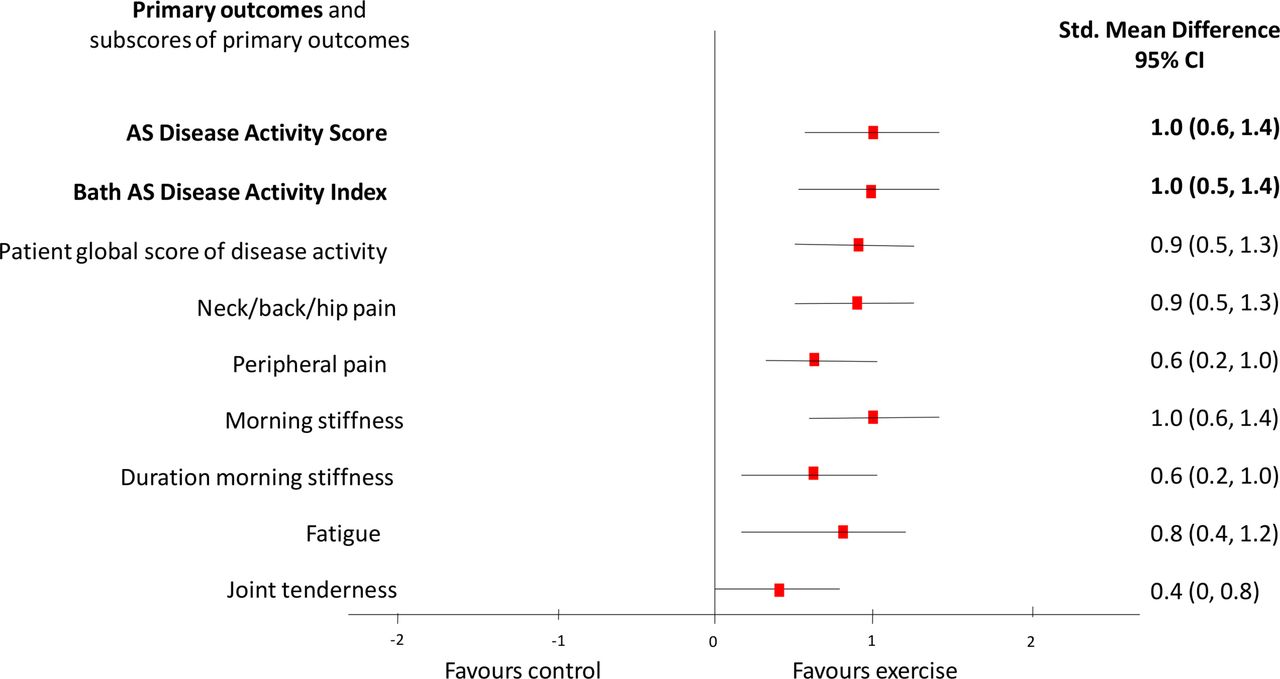
For ASDAS, there was a significant treatment effect (table 2), which corresponds to a 23% difference in change between the groups (27% vs 4%). Similarly, for BASDAI, there was a significant treatment effect (table 2), corresponding to a 24% difference in change between the groups (33% vs 9%). Effects sizes for primary outcomes with sub-scores are shown in figure 2 (CRP is not included due to skewed distribution).
{kind=link}
{kind=link}
Forest plot of the effect of high intensity exercises on primary outcomes, the disease activity indexes with sub-scores. Data are shown as standardised mean difference (SMD, effect sizes) with 95% CI. SMDs between 0.2 and 0.4 are considered as a small effect size, from 0.5 to 0.7 as a medium effect size, and ≥0.8 as a large effect size. AS; ankylosing spondylitis.
Primary outcomes. Effect of high intensity exercises on disease activity. Values are shown as mean with SD unless stated otherwise
At 3 months, 25 (52%) patients in the exercise group and five (10%) patients in the control group had achieved 20% improvement, which gives an AIB (95% CI) of 42% (25% to 58%) and NNT (95% CI) was 3 (2 to 4). Eighteen (38%) patients in the exercise group achieved 40% improvement versus two (4%) in the control group, which gives an AIB (95% CI) of 33% (19% to 48%) and the NNT (95% CI) was 3 (2 to 5).
Secondary outcomes
Secondary outcomes are shown in table 3. There was 8.2% difference in change in VO2peak between the groups (p<0.001), with comparable end criteria. Significant treatment effects were seen on physical function, 27% difference in change in favour of the exercise group (38% vs 11%) and for flexibility, 10% difference (14% vs 4%). A significant treatment effect was seen on waist circumference (p=0.004), but no between-groups differences were found in change of BMI or ESR. A per protocol analysis showed a trend towards a beneficial effect on lean body mass (mean group difference [95% CI], 998 g [−50 to 2025], p=0.061).
Effects of exercise on secondary outcomes. Values are shown as mean with SD unless stated otherwise
Adherence
Thirty-eight (76%) patients in the exercise group followed ≥80% of the prescribed exercise protocol (≥29 of 36 sessions). Four (8%) patients discontinued the exercise programme after having attended just a few sessions. In the control group, five (10%) patients had performed cardiorespiratory or strength exercises (≥2/week) during the intervention period. Per protocol analysis (eg, [n=38], CG; [n=44]) did not change any of the results.
Adverse events and safety
One patient in the exercise group experienced chest pain and nausea during the exercises, and completed the intervention at moderate intensity after advice from a cardiologist. Two patients reported persistent pain during exercise, but the safety of the exercise programme was proven by the beneficial group-effect on disease activity.
Discussion
We believe this to be the first RCT to examine the effects of high-intensity exercise in a large sample of patients with axSpA. We report that high-intensity exercise improves disease activity in patients with axSpA. The exercise group reduced disease activity (symptoms and inflammation) and improved their VO2peak significantly compared with the control group. The results are important, as they prove the efficacy and safety of high-intensity exercises, and patients with axSpA can thereby take advantage of the CV-health effects of such exercises.
Comparisons with other studies
A 2017 systematic review also concluded that regular exercises reduced disease activity in patients with axSpA.4 The effect sizes reported in the review were smaller, which may be explained by higher exercise intensity in our study. The dose of exercise, and especially the intensity, is decisive for the physiological responses,15 and high intensity exercises are needed to modify inflammation and improve CV disease risk profile.29
Studies of high intensity exercise for inflammatory rheumatic diseases are sparse. A small cross-over study in patients with rheumatoid arthritis supports the results of our study, concluding that disease activity and inflammation (CRP) were reduced or stable, and they also found beneficial effects on CV disease risk factors.30
The treatment effect in ASDAS score was lower than the clinically important improvement defined for pharmacological treatment (1.1 point).31 A reason for this may be that about 40% of the study population was on stable TNF-inhibitor treatment. Yet, the effect sizes for the primary outcomes were large and the number needed to treat was only three patients. TNF-inhibitors are shown to be effective in patients with axSpA,32 but it is a costly treatment not available for all patients. It is therefore promising that the exercise intervention in this study gave similar effects as shown for TNF-inhibitors.33 34 Further, exercise is a low-cost treatment that do not result in harmful effects. Moreover, it has been reported that the use of TNF-inhibitors can increase adherence to exercise.35 The optimal treatment for patients with axSpA is therefore likely to be a combination of pharmacological treatment and exercise.
Possible explanations and implications
In patients with axSpA, disease activity is expressed as an index of inflammation and symptoms, for example, pain can be caused by joint and tissue damage due to current or previous inflammation.36 The results showed a significant beneficial effect on CRP that might be explained by the anti-inflammatory effect of exercise.37 However, since the inflammatory burden for patients in this study was moderate, the observed effect on disease activity may also be caused by effect of exercise on clinical symptoms.8
In addition to the disease-modifying effects, high intensity exercises also have the potential to prevent co-morbidities, especially CV diseases.15 It is established that patients with axSpA have an increased risk of CV diseases,9 and observational studies have shown lower cardiorespiratory fitness in this group than in the general population.38–41 In the present study, the mean treatment effect of 2.7 mL in VO2peak indicates large health gain, as it has been reported that every 1 mL increase is associated with a 15% decrease in CV death.42 Together with significant reduction in abdominal fat and inflammation, the exercise programme in this study resulted in a considerably more beneficial CV disease risk-profile.
Thus, the disease modifying effects and the beneficial effect on CV-health indicate that exercise programmes for patients with axSpA should follow general guidelines for improving cardiorespiratory fitness and muscular strength.
Strengths and limitations
Strengths of the study include the RCT design, blinding of assessor, objective measurements for disease activity, ITT-analysis and a low drop-out rate. Furthermore, the exercise was individually adapted, and adherence to the protocol was confirmed by the improvement in VO2peak and lean body mass. Importantly, the intervention was carried out by clinicians, indicating that similar effects can be expected in clinical practice.
Due to the demanding exercise programme, we may have recruited motivated patients. Nevertheless, the majority of the predominantly middle-aged patients were recruited at outpatient clinics, and almost half of them were treated with TNF-inhibitors. These factors speak to the external generalisability of the results.
A limitation was the lack of blinding of participants. The exercise group received more attention as they had weekly contact with a physiotherapist, and a psychological effect on patient reported outcomes cannot be ruled out.43 Another limitation is that we did not study long-term effects. We considered exercise effects as acute effects because of their known anti-inflammatory response.37 Hence, we considered the most relevant time point to be the end of the intervention.
We conclude that high intensity exercise should be strongly considered as a part of treatment of axSpA. Future studies should examine the effects of longer exercise interventions with longer follow-up. It is also time to refine the high intensity exercise programme in clinical practice.
What are the findings?
A 3 months programme of high intensity cardiorespiratory and strength exercises reduced disease activity and improved both physical function and cardiovascular health in patients with axial spondyloarthritis.
How might it impact on clinical practice in the future?
We recommend exercise as an important part of the management in patients with spondyloarthritis.
Acknowledgments
We thank the patient representatives for their contribution in the study as well as all the patients who participated in the study. We thank Inger Gjertsson for her contribution in the Swedish study centre. Further, we also thank the physiotherapists Emma Klittmar, Linn A Haukland, Mary E Deighan Hanssen and Kim Reier Nielsen Martinsen for their help with exercise supervision.
References
Footnotes
Contributors SHS designed the trial, recruited participants, collected, analysed and interpreted data and wrote the report. AB recruited participants, interpreted data and reviewed the manuscript. IJB and SP designed the trial, recruited participants, interpreted data and reviewed the manuscript. SR collected data and reviewed the manuscript. AGS designed the trial and reviewed the manuscript. KBH designed the trial and reviewed the manuscript. MWJ and EP recruited participants, supervised the exercise group and reviewed the manuscript. HD designed the trial, analysed and interpreted data and wrote the report. All authors have approved the final draft to be published.
Funding This trial was supported by The Norwegian Fund for Post-Graduate Training in Physiotherapy and the Norwegian Rheumatology Association.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study protocol and consent documents were approved by the Regional Committee for Medical and Health Research Ethics (REK South East 2015/86) in Norway and the Regional Ethical Review Board Gothenburg in Sweden (032-16).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors agree to share anonymised data upon reasonable request.