Article Text

Abstract
Introduction Whether patients with inflammatory rheumatic and musculoskeletal diseases (RMD) are at higher risk to develop severe courses of COVID-19 has not been fully elucidated. Aim of this analysis was to describe patients with RMD according to their COVID-19 severity and to identify risk factors for hospitalisation.
Methods Patients with RMD with PCR confirmed SARS-CoV-2 infection reported to the German COVID-19 registry from 30 March to 1 November 2020 were evaluated. Multivariable logistic regression was used to estimate ORs for hospitalisation due to COVID-19.
Results Data from 468 patients with RMD with SARS-CoV-2 infection were reported. Most frequent diagnosis was rheumatoid arthritis, RA (48%). 29% of the patients were hospitalised, 5.5% needed ventilation. 19 patients died. Multivariable analysis showed that age >65 years (OR 2.24; 95% CI 1.12 to 4.47), but even more>75 years (OR 3.94; 95% CI 1.86 to 8.32), cardiovascular disease (CVD; OR 3.36; 95% CI 1.5 to 7.55), interstitial lung disease/chronic obstructive pulmonary disease (ILD/COPD) (OR 2.79; 95% CI 1.2 to 6.49), chronic kidney disease (OR 2.96; 95% CI 1.16 to 7.5), moderate/high RMD disease activity (OR 1.96; 95% CI 1.02 to 3.76) and treatment with glucocorticoids (GCs) in dosages >5 mg/day (OR 3.67; 95% CI 1.49 to 9.05) were associated with higher odds of hospitalisation. Spondyloarthritis patients showed a smaller risk of hospitalisation compared with RA (OR 0.46; 95% CI 0.23 to 0.91).
Conclusion Age was a major risk factor for hospitalisation as well as comorbidities such as CVD, ILD/COPD, chronic kidney disease and current or prior treatment with GCs. Moderate to high RMD disease activity was also an independent risk factor for hospitalisation, underlining the importance of continuing adequate RMD treatment during the pandemic.
- epidemiology
- arthritis
- glucocorticoids
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Due to systemic inflammatory conditions and immunomodulating treatment, rheumatic and musculoskeletal disease (RMD) patients might be at increased risk of a more severe course of SARS-CoV-2 infection.
Only limited data on risk factors for a critical course of COVID-19 in patients with RMD are available.
What does this study add?
Age, comorbidities (cardiovascular disease, interstitial lung disease/chronic obstructive pulmonary disease and chronic kidney disease), the use of glucocorticoids for the treatment of RMD and RMD disease activity are independent risk factors for COVID-19 hospitalisation.
How might this impact on clinical practice?
Adequate treatment of RMD with control of disease activity is crucial for the management of our patients during the pandemic.
Patients with RMD with risk factors identified with this analysis should be closely monitored and receive guidance about infection risk minimising behaviour.
Introduction
In Germany, the first cases of SARS-CoV-2 infection (COVID-19) were reported at the end of January 2020.1 Similar to other European countries, SARS-CoV-2 spread rapidly in Germany. The course of infection with SARS-CoV-2 ranges from asymptomatic to fatal. In the general population, higher age, male gender and comorbidities are associated with the severity of SARS-CoV-2 infection.2 3 Since the outbreak of the pandemic, concerns have been raised regarding the probability of developing a severe or even life-threatening course in patients with inflammatory rheumatic and musculoskeletal diseases (RMD).4–6 Patients with RMD are characterised by an overall increase in risk of infection due to the autoimmune disease itself and immunomodulatory drugs.7–9 The risk of infection is dependent on age, functional capacity, comorbidities and immunomodulatory treatment with biological disease-modifying antirheumatic drugs (bDMARDs) and glucocorticoids (GC).10 Immunomodulatory drugs with anti-inflammatory action may limit overwhelming immune responses that appear to be responsible for the severe pulmonary complications in COVID-19.11 12 However, not all immunomodulatory treatments seem to influence the risk for a critical course in the same direction. Whereas registry data had shown a beneficial effect of biological DMARDs regarding the development of sepsis and mortality in patients with rheumatoid arthritis (RA) and serious infections, it had also shown a significantly increased risk conveyed with GCs.13 Data from the COVID-19 Global Rheumatology Alliance (GRA) physician-reported registry indicate that GC ≥10 mg/day are associated with a higher hospitalisation rate with SARS-CoV-2 infection in patients with RMD,14 which underlines the importance of controlling disease activity with DMARDs in order to decrease GC dose.
Furthermore, the recommendations from EULAR and DGRh (German Society for Rheumatology) state that immunomodulating therapy should be maintained during the SARS-CoV-2 pandemic to avoid RMD relapse.15 16
Limited data are available as for whether and to what extent patients with RMD are at an increased risk for SARS-CoV-2 infection11 17 18 and for a more severe course of COVID-19. For this reason, a national registry was established allowing a rapid and timely collection of RMD cases with confirmed SARS-CoV-2 infections in Germany in order to analyse the clinical course of COVID-19 in patients with RMD and to develop guidance for the management of patients with RMD during the COVID-19 pandemic.19 The aim of this analysis was to identify risk factors for hospitalisation, comparing non-hospitalised patients with RMD to hospitalised patients, stratified by the need for invasive ventilation.
Methods
Data source
In March 2020, the German Society for Rheumatology, together with the Justus-Liebig-University Giessen, founded a national registry for patients with pre-existing inflammatory rheumatic diseases (RMD) and SARS-CoV-2 infection confirmed by PCR test. Rheumatologists voluntarily enter the data into an online database with implemented plausibility checks (URL https://www.covid19-rheuma.de).
The ascertained data include SARS-CoV-2 infection-specific items such as symptoms, duration, treatment and outcome, RMD specific items such as diagnosis, physician assessed disease activity (categorised into remission, low, moderate or high disease activity), and treatment of RMD, and general items such as sociodemographic information and comorbidities. Missing data on diagnosis and treatment of RMD and outcome of COVID-19 can be queried by contacting participating physicians. Data collection was done retrospectively. Participating centres consist of academic and non-academic rheumatology departments and private practices in Germany.
The German registry’s content is harmonised with the EULAR COVID-19 database (https://www.eular.org/eular_covid19_database.cfm) to allow joint analysis. The study is registered at EuDRACT 2020-001958-21#.
Statistical analysis
Descriptive statistics were applied to compare non-hospitalised patients with hospitalised patients, either without or with invasive ventilation.
Multivariable logistic regression was used to estimate odds ratios (OR) and 95% CIs for the main outcome parameter of this analysis, which is hospitalisation due to COVID-19 as indicator for severity of the SARS-CoV-2 infection. Simple logistic regressions with one explanatory variable were performed to determine the set of regressors for the multivariable regression. Variables with a p<0.1 were included in the final model. Covariates included in the model were age group, rheumatic disease group (RA, spondyloarthritis, connective tissue diseases (CTDs) and vasculitis, other rheumatic diseases), inflammatory activity of the rheumatic disease, specific comorbidities (cardiovascular disease (CVD), hypertension without CVD, interstitial lung diseases (ILD) or chronic obstructive pulmonary disease (COPD), diabetes mellitus, chronic kidney disease, cancer), prior and/or current use of GC (none, up to 5 mg/day, over 5 mg/day). Spondyloarthritides included psoriatic arthritis (PsA), axial spondyloarthritis (axSpA) and enteropathic arthritis. CTDs and vasculitis included systemic lupus erythematosus, Sjögren’s syndrome, systemic sclerosis, mixed CTDs, overlap syndromes, polymyalgia rheumatica, granulomatosis with polyangiitis (GPA), eosinophilic GPA, microscopic polyangiitis, large vessel vaculitis, Behçet’s disease and other types of vasculitis. For patients belonging to more than one rheumatic disease category, we used the following hierarchy for prioritisation: CTD/vasculitis>RA>spondyloarthritides>other rheumatic diseases. In this way, disjoint categories are created, establishing a clear reference group for interpretation of the regression model and avoiding collinearities. In order to avoid collinearity between CVD and hypertension, hypertension in the model refers to patients who had hypertension but not CVD. Missing values for obesity, disease activity state, GC dose and non-steroidal antirheumatic agents were derived by multiple imputation using full conditional specification.20 Results of the logistic regression analyses for 10 imputed datasets were pooled by Rubin’s rules. Calculations were carried out with the software packages SAS, V.9.4, and R, V.3.6.3.
Results
Patients characteristics
Between March 30 (first patient in) and 1 November 2020 (database lock), 468 patients with RMD and a PCR-confirmed SARS-CoV-2 infection were documented in the German registry, 309 patients were female. Median age was 57 years. Regarding RMD diagnosis, RA was most common with 48%, followed by 14% PsA, and 12% axSpA.
Patient characteristics are shown in table 1, stratified into the three groups: non-hospitalised patients, hospitalised patients without or with need for invasive ventilation. The following numbers of missing values exist: 88 (18.8%) for duration of COVID-19 symptoms, 51 (10.9%) for obesity, 31 (6.6%) for inflammatory activity state, 1 for GC dose (0.6%, among patients receiving GCs) and 33 (7.1%) for non-steroidal antirheumatic drugs. There was no missing data on outcome of SARS-CoV-2 infection, so all patients either fully recovered or died.
Patient characteristics stratified for non-hospitalisation, hospitalisation without ventilation and hospitalisation with invasive ventilation
Of the 468 patients, 136 (29%) were hospitalised of whom 26 (5.5%) needed invasive ventilation. 19 patients died, resulting in a case fatality rate of 4%. Eighteen of these patients died in the hospital, 13 had received invasive ventilation.
Most patients with RMD had comorbidities; only 38% did not have any other chronic condition. The most frequent comorbidity was arterial hypertension, followed by obesity, CVD and diabetes.
Regarding RMD treatment, 19% of the patients did not receive any DMARD. Thirty-six per cent were on bDMARDs and 41% on conventional synthetic (cs)DMARD monotherapy. Thirty-nine per cent of the patients were on GC treatment, most of them (81%) received low dose GCs of ≤5 mg/day.
Comparison of non-hospitalised patients with hospitalised patients without ventilation and hospitalised patients with invasive ventilation
The percentage of men was larger among hospitalised patients with ventilation (50%) compared with those without ventilation (32%) or non-hospitalised (34%) (table 1).
Forty-four per cent of the non-hospitalised patients suffered from RA, compared with 56% and 65% in the hospitalised groups. According to physicians’ assessments, moderate to high RMD disease activity was present in 11% of the non-hospitalised patients, 26% in the hospitalised patients without ventilation and 34% in the ventilated patients.
Regarding RMD treatment, 18% of the non-hospitalised patients did not receive any DMARD compared with 24% and 19% in the hospitalised groups. Tumour necrosis factor inhibitors were documented as RMD treatment in 27% of the non-hospitalised patients, in 12% of the hospitalised group without ventilation and 8% in the ventilated patients. Twenty-seven per cent of the ventilated patients were on B-cell-depletion treatment, whereas only 3% of the non-hospitalised and 6% of the hospitalised patients without ventilation had received B-cell-depleting treatment.
Factors associated with hospitalisation
Results of the univariate analyses comparing non-hospitalised patients with hospitalised patients are shown in table 2.
OR of COVID-19 hospitalisation in univariate analyses of patients with RMD
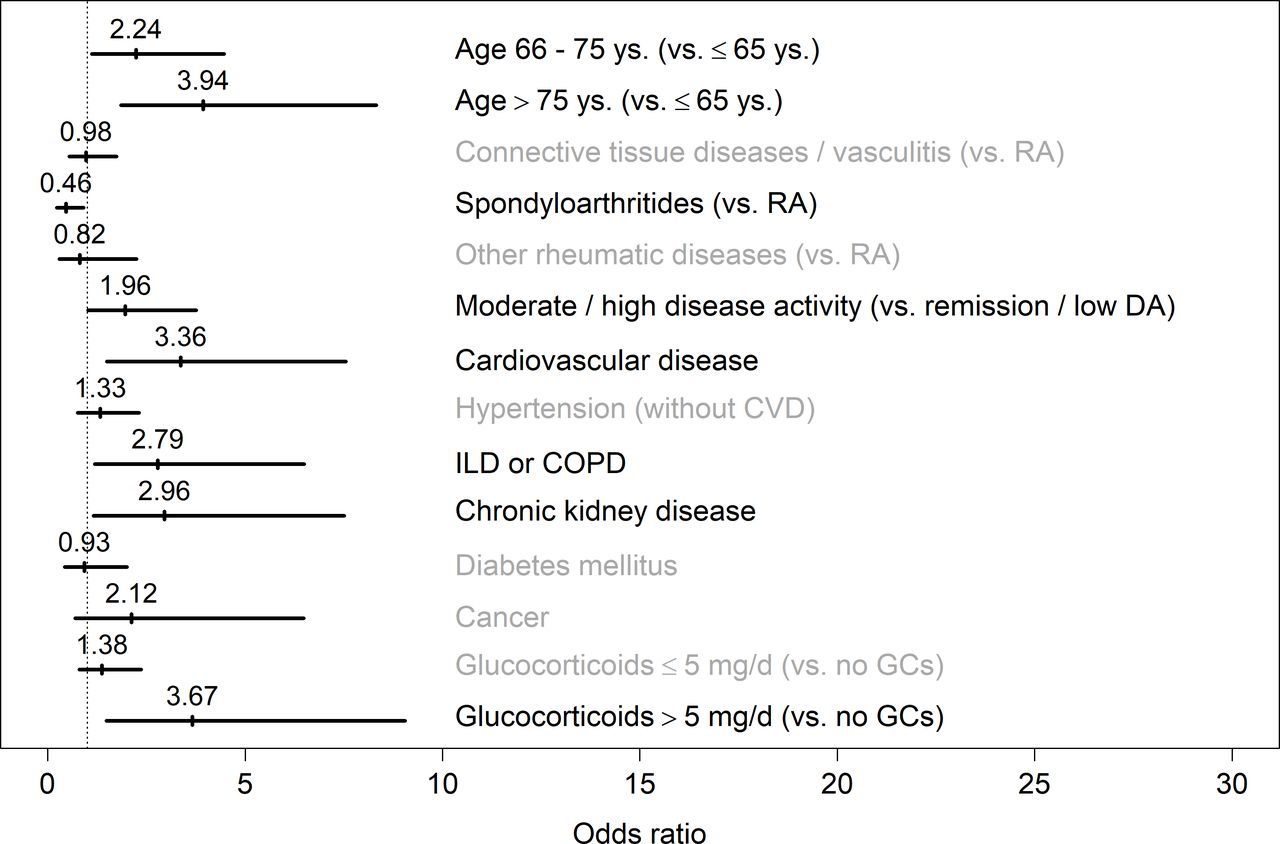
The results of the multivariable model are shown in figure 1 and online supplemental table 1). Age>65 years (OR 2.24; 95% CI 1.12 to 4.47), but even more>75 years (OR 3.94; 95% CI 1.86 to 8.32), CVD (OR 3.36; 95% CI 1.5 to 7.55), lung disease (ILD/COPD) (OR 2.79; 95% CI 1.2 to 6.49) and chronic kidney disease (OR 2.96; 95% CI 1.16 to 7.5) were associated with higher odds of hospitalisation. Patients with spondyloarthritides showed a lower risk of hospitalisation compared with RA (OR 0.46; 95% CI 0.23 to 0.91). Moderate to high RMD disease activity was furthermore significantly associated with hospitalisation (OR 1.96; 95% CI 1.02 to 3.76), as well as treatment with GC in dosages>5 mg/day (OR 3.67; 95% CI 1.49 to 9.05).
Supplemental material

{kind=link}
Multivariable logistic regression was used to estimate ORs and 95% CIs for the main outcome parameter of this analysis, hospitalisation due to COVID-19 versus non-hospitalisation as indicator for severity of the SARS-CoV-2 infection. COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; DA, disease activity; GC, glucocorticoid; ILD, interstitial lung disease; RA, rheumatoid arthritis.
Discussion
In the challenging situation of the SARS-CoV-2 pandemic, physicians and patients need rapid access to the evolving evidence to close the gaps of knowledge which are stressful for patients with chronic conditions. When the pandemic started, it was unclear whether patients with RMD are at an increased risk to get infected or whether they have a higher risk of a severe course of COVID-19. In this analysis, hospitalisation was used as indicator for a more severe course. Older age, CVD, ILD/COPD, chronic kidney disease, treatment with GC at doses of >5 mg/day, and moderate to high RMD disease activity were identified as independent risk factors for hospitalisation.
Our results are in line with the recently published analysis of the GRA.14 In the GRA analysis, the cases from the German registry had not yet been included, so these two cohorts are independent. Similar results have also been found in a meta-analysis on autoinflammatory diseases including RMDs.21
Age seems to be the most important factor associated with a more severe course of COVID192 3 22 23 and this holds also true for patients with RMD as described in our analysis and other reports.24–28
Importantly, moderate to high RMD disease activity was identified as an independent risk factor for hospitalisation. This is an important finding, not only in that this is a risk factor specifically related to RMDs but also with implications for the daily management, reaffirming recent recommendations that state the importance of RMD disease control during the pandemic.15 16
The influence of comorbidities is also widely recognised since the first reports of COVID-19.29 In our cohort, CVD, ILD/COPD and chronic kidney disease were significantly associated with hospitalisation. Interestingly, asthma was not associated with an increased risk as was also described in the UK.3 This is in accordance with an asthma-specific analysis where the authors did not find an association of asthma with hospitalisation.30 This effect is in contrast to other pulmonary comorbidities such as ILD and COPD.
In our cohort, prior or current treatment with GC was associated with a high risk of hospitalisation in accordance with the GRA analysis14 and with previous evidence of an increased infection risk in general.10
The interpretation of the influence of GC treatment on hospitalisation has to be performed with caution. There is a probability of confounding by indication since GC are given under certain circumstances which may influence the outcome itself like a high disease activity of the RMD. Since uncontrolled RMD activity also enhances the risk of infections, our results should not encourage stopping GC treatment. However, GC should be administered in the lowest possible dose, as recommended by the recently published guidance for the management of COVID-19 in RMD,15 16 as already a dose of >5 mg/day was associated with an increased risk of hospitalisation in our study.
Male gender has also been described as an important risk factor for a more severe course and higher mortality.3 23 In our analysis, male gender was not associated with hospitalisation. This was also the case in the GRA analysis.14 However, regarding the results of the descriptive analysis (table 1), male gender was much more common in the group of ventilated patients compared with the other patients. As already described in the general population, male gender might therefore be associated with a worse outcome also in patients with RMD.3 23 31
Comparing the results from RMD with chronic inflammatory bowel disease (IBD), interesting parallels can be found. In the first analysis of the international registry for patients with IBD and confirmed SARS-Cov-2 infection, similar risk factors associated with worse COVID-19 outcome were identified, namely older age, number of comorbidities and use of systemic GC.32
The strengths of our study include the large sample size with PCR confirmed SARS-CoV-2 infections in patients with RMD. As all patients were treated in Germany, both the healthcare system and treatment strategies for COVID-19 were comparable in all cases, reducing confounding due to differences regarding these factors as might be present in analyses including patients from many countries. The completeness of data is high with only a small percentage of missing values. Particularly, the outcome ‘hospitalisation’ was known in all cases, as all cases were documented after full recovery or death of patient.
A limitation of our study is the observational design, which is prone to confounding by indication. For example, it is possible that patients taking GCs might be hospitalised more often because of the potential risk of a more severe outcome of the infection. Also, a potential influence of the SARS-CoV-2 infection on the course of the RMD cannot be assessed based on our data because of the cross-sectional design. Only few details of the RMD are known, as factors like disease duration, functional capacity or treatment history are not captured in the registry.
Although this is one of the largest RMD COVID-19 cohorts published so far, the number of cases was still too low to include specific RMD treatments into the multivariable analysis. With increasing numbers of patients, these analyses will probably become possible in the near future.
Another limitation is that possibly more severe cases were preferably documented, resulting in a selection bias. However, we believe that the conclusions drawn from our model are robust since there is no indication that the impact of age, disease activity, specific comorbidities or GC treatment is influenced by this bias.
In this large German cohort of patients with RMD with SARS-CoV-2 infection, 29% were hospitalised. Age, RMD disease activity, CVD, ILD/COPD and GC treatment starting at doses of >5 mg/day were independently associated with hospitalisation. These risk factors are similar to those found in general COVID-19 cohorts. However, to our knowledge, this is the first analysis identifying moderate to high RMD disease activity as independent risk factor for hospitalisation due to COVID-19. It is important to continue the documentation of patients with RMDs and COVID-19 in order to generate more evidence for counselling and to find the best therapeutic management of our patients.
Acknowledgments
The authors would like to thank all physicians (Boeddecker, Stephanie; Kurthen, Reiner; Mattar, Johannes; Anita Viardot; Brandt-Jürgens, Jan; Rihl, Markus; Menne, Hans-Jürgen; Bremer, Jan-Phillip; Bauhammer, Jutta; Maerz, Vanessa; Dörfler, Rainer; Andriopoulos, Nikolaos; Merwald-Fraenk, Helga; Henes, Jörg; Noethe, Matthias; Wiesent, Franziska; Weigelt, Martin; Hauf, Maura-Maria; Riemekasten, Gabriela; Aries, Peer; Bloching, Hans; Reindl, Christiane; Hein, Liane; Herzer, Peter; Decker, Elvira; Gilly, Jasmin; De Groot, Kirsten; Korsten, Peter; Krusche, Martin; Kovacs, Magdolna; Bösenberg, Ilka; Piechalska, Marta; Saar, Petra; Köchel, Katrin; Maus, Sebastian; Krummel-Lorenz, Brigitte; Lantzsch, Heiko; Raub, Wolfgang; Kittel, Birgit; Röser, Markus; Sievert, Iris; Weiß, Angela; Ospina; Purschke, Michael; Scholz, Michaela; Anders, Nils; Rossmanith, Christopf; Krüger, Klaus; Bruckner, Andreas; Hartmann, Urs; Nerenheim, Anabell; Gniezinski- Schwister, Agnes; Alexander, Tobias; Rockwitz, Karin; Haibel, Hildrun; Schieweck-Güsmer, Andreas; Steinchen, Nicolai; Bender, Nico; Boche, Konrad; Winau, Lea; Bäuerle, Michael; Saech, Jaesmine; Klink, Claudia; Feuchtenberger, Martin; Avemarg, Sarah; Drexler, Elke; Weiner, Stefan; Sonn, Sigrid; Blendea, Daniel; Becker, Klaus; Witt, Matthias; Melzer, Adelheid; Eder, Roman; Fleck, Martin; Löffler, Christian; Hoese, Guido; Schönherr, Jutta; Vallbracht-Ackermann, Inka; Baerwald, Christopf; Sekura, Matthias; Kreutzberger, Rene; Voll, Reinhard; Schiebel, Magnus; Nottarp, Dirk; Zaus, Monika; Wysocki, Nina; Birkner, Gerhard; Krause, Dietmar; Amberger, Christopher; Sensse, Jörg; Grünke, Mathias; Späthling-Mestekemper, Susanna; Werner, Stephanie; Freudenberg, Stefanie; Bellm, Michaela; Willeke, Peter; Röther, Ekkehard; Strunk, Johannes; Veerhoff, Susanne; Welcker, Martin; Schlenker, Ulrike; Karberg, Kirsten; Venhoff, Nils; Schuch, Florian; Alten, Rieke; Hueber, Axel; Albach, Frederik; Hasenkamp, Charlotte; Ochs, Wolfgang; Rudwaleit, Martin; Hein, Reinhard; Büllesfeld, Sarah; Jacobi, Annett M.; Becker, Heidemarie; Hallmann-Böhm, Till; Glaser, Cornelia; Sandrock, Eva; Bohl-Bühler, Reckert; Schübler, Anna-Sophia; Pfeil, Alexander; Schnarr, Sebastian; Brzank, Martin; Iburg, Elke; Schmalzing, Marc; Maier, Ingeborg; Weidner, Sven; Mortsch, Markus; Rissom, Viale; Andreica, Ioana; Wisseler, Hans; Schoo, Ulrich; Hübner, Georg; Burger, Sandra; Claußnitzer, Anne; Olk, Jürgen; Günther, Florian; Voglau, Markus; Kirchgässner, Matthias; Vaith, Peter; Weinerth, Jutta; Mörtlbauer, Harald; Wernicke, Dirk; Göttl, Karl Heinz; Aringer, Marin; Langen, Sabine; Stockdreher, Karin; Hoff, Paula; Kreher, Gabi; Engel, Andreas; Heel, Nicole; Sglunda, Ondrej; Kurzeja, Rolf; Stapfer, Gerald; Märtz, Anette; Thoden, Jan; Georgi, Joachim; Gao, Ino; Pulla, Almut; Reckert, Sabine; Röther, Fabian; Mauß-Etzler, Ursula; Gauler, Georg; Kalthoff, Ludwig; Edelmann, Edmund; Hadjiski, Denitsa; Jandova, Ilona; Grieshaber Bouyer, Ricardo; Metzler, Claudia; Muche, Burkhard; Pick, Dorothea; Schwarze, Ilka; Vinnemeier-Laubenthal, Lisa; Kapelle, Andreas; Knietz, Christian; Igney-Oertel, Annette; Krieger-Dippel, Eveline; Schmitt-Haendle, Matthias; Hermann, Walter; Tatsis, Stefanie; Arndt, Uta; Schlittenhardt, Daniel; Baumann, Christine; Özden, Filiz; Rösel, Maike; Detert, Jacqueline; Braunisch, Matthias; Demtröder, Frank; Nüvemann, Dieter; Steinmüller, Mirko; Hornig, Johannes; Sheikh, Naheed; Broll, Matthias; Meier, Florian; Juche, Aaron; Görl, Norman; Sarholz, Michael; Feine, Miriam; Hendrix, Claudia; Zinke, Silke; Sokoll, Katharina; Blank, Norbert; Surmann, Mechthild; Kaudewitz, Dorothee; Protopopov, Mikhail; Kudela, Holger) and personnel involved in the documentation of the cases in our registry.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
CS and ACR contributed equally.
Contributors RH and UM-L: Substantial contributions to the conception of the work and the acquisition, analysis and interpretation of data for the work, drafting the work. MS: substantial contributions to the conception of the work, statistical analysis and interpretation of data for the work. BFH, AK, H-ML, AP, JR, TS, AS, HS-K and REV: Substantial contributions to the conception of the work and the interpretation of data for the work. Revising the work critically for important intellectual content. CS and ACR: substantial contributions to the conception and design of the work and the analysis, and interpretation of data for the work. Drafting the work. All authors: final approval of the version to be published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding RH was supported by the Justus-Liebig University Giessen Clinician Scientist Programme in Biomedical Research (JLU-CAREER) to work on this registry.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the ethics committee of the Justus-Liebig-University Giessen (#52–50).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.