Article Text

Abstract
Objective Evaluation of the efficacy and safety of guselkumab, a human monoclonal antibody targeting the interleukin-23p19 subunit, in patients with psoriatic arthritis (PsA) through 1 year.
Methods Adults who met ClASsification criteria for Psoriatic ARthritis, with active disease (≥3 swollen and ≥3 tender joints; C reactive protein ≥0.3 mg/dL) despite standard treatment (31% previously received ≤2 tumour necrosis factor inhibitors (TNFi)), were randomised (1:1:1) to guselkumab 100 mg every 4 weeks (Q4W); guselkumab 100 mg at Week0, Week4, then Q8W; or placebo with cross-over to guselkumab 100 mg Q4W at Week24 (PBO→Q4W) through Week48. Clinical efficacy through Week52 (employing non-responder imputation) and adverse events (AEs) through Week60 were evaluated.
Results Of 381 treated patients, 90% completed the study. Numerical increases in the proportions of patients achieving ≥20% improvement in ACR criteria (ACR20) were observed post-Week24, reaching 73% (94/128) and 60% (76/127) for Q4W-randomised and Q8W-randomised patients, respectively, by Week52. Proportions of patients achieving ACR50/ACR70/skin responses and minimal/very low disease activity were maintained, as were improvements in physical function and health-related quality of life, through Week52 in guselkumab-randomised patients. Response to guselkumab was maintained in both TNFi-naïve and TNFi-experienced patients. Serious AEs and serious infections occurred in similar proportions of guselkumab Q4W-randomised (3% and 0%) and Q8W-randomised (6% and 2%) patients through Week60, with no new safety concerns versus observations through Week24. No guselkumab-treated patient and two patients receiving placebo died; no study participant developed opportunistic infection or inflammatory bowel disease.
Conclusion Guselkumab provided sustained improvement across multiple clinical manifestations of PsA, maintaining a favourable benefit-risk profile, through 1 year regardless of prior TNFi exposure.
- arthritis
- psoriatic
- biological therapy
- tumor necrosis factor inhibitors
- cytokines
Data availability statement
The data sharing policy of Janssen Pharmaceutical Companies of Johnson & Johnson is available at https://www.janssen.com/clinical-trials/transparency. As noted on this site, requests for access to the study data can be submitted through the Yale Open Data Access (YODA) Project site at http://yoda.yale.edu.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Psoriatic arthritis (PsA) is a multifaceted inflammatory disorder, and agents targeting novel disease pathways have the potential to achieve remission or low levels of disease activity across disease domains. Guselkumab is a high-affinity, fully human, anti-interleukin-23p19 subunit monoclonal antibody. Through Week24 of the pivotal phase III DISCOVER-1 study of patients with active PsA, including 31% who were tumour necrosis factor inhibitor (TNFi)-experienced, guselkumab 100 mg given every 4 weeks or 8 weeks demonstrated significant efficacy across multiple domains of PsA, with acceptable and comparable safety profiles.
Key messages
What does this study add?
Results through the completion of DISCOVER-1 demonstrate that the significant improvements in joint and psoriatic skin symptoms, physical function, and health-related quality of life at Week24 afforded by guselkumab 100 mg were maintained through 1 year with continued guselkumab. Improvements were maintained in both TNFi-naïve and TNFi-experienced patients. For both guselkumab dosing regimens, the safety profile through 1 year in patients with PsA was consistent with that observed at Week24 and in guselkumab-treated patients with psoriasis.
How might this impact on clinical practice?
Guselkumab targets a novel disease pathway to provide sustained improvements across the diverse clinical manifestations of PsA, in concert with an acceptable safety profile and regardless of prior receipt of TNFi.
Introduction
There have been breakthroughs in understanding psoriatic arthritis (PsA) immunopathogenesis and the subsequent development of biologic therapies, but agents targeting novel disease pathways have the potential to achieve remission or low levels of disease activity across disease domains in some patients.
Interleukin (IL)-23, an upstream regulatory cytokine, promotes development of downstream effector T helper 17 cells (Th17) cells and their cytokine products, including IL-17.1–4 The IL-23/IL-17 pathway promotes and sustains chronic inflammation in immune-mediated diseases including psoriasis and PsA,5 6 and susceptibility to these conditions is associated with genetic polymorphisms in IL-23 and its receptors.7–11 Guselkumab, a high-affinity monoclonal antibody targeting the human IL-23p19 subunit,12 was approved to treat moderate-to-severe plaque psoriasis in 2017 and recently became the first selective IL-23 inhibitor approved to treat active PsA in several countries.13
Guselkumab demonstrated efficacy through Week24 in both phase III PsA studies (DISCOVER-1,14 DISCOVER-215). We now report 1 year data from DISCOVER-1, conducted in biologic-naïve and tumour necrosis factor inhibitor (TNFi)-experienced patients, the latter representing a growing PsA cohort in clinical practice.
Patients and methods
Patients
DISCOVER-1 enrolled adults with active PsA (≥3 tender and ≥3 swollen joints; C reactive protein (CRP) ≥0.3 mg/dL) despite conventional, non-biologic, disease-modifying antirheumatic drugs (DMARDs), apremilast, or non-steroidal anti-inflammatory drugs (NSAIDs).14 Patients fulfilled ClASsification criteria for Psoriatic ARthritis and had active or a history of plaque psoriasis. Approximately 30% of patients could have received one or two TNFis. All patients provided written informed consent.
Study design
This phase III, randomised, double-blind study, conducted at 86 global sites,14 comprised 6 weeks of screening (commenced: 28 August 2017) and both placebo-controlled (Week0–Week24) and active (Week24–Week52; final dose at Week48) treatment periods. Safety follow-up continued 12 weeks after the final dose (last Week60 visit: 14 November 2019).
Participants were randomised (1:1:1) to subcutaneous injections of guselkumab 100 mg every 4 weeks (Q4W); guselkumab 100 mg at Week0, Week4, then Q8W; or placebo Q4W with cross-over to guselkumab 100 mg Q4W at Week24 (PBO→Q4W). Central randomisation and study blinding procedures were previously reported.14 Patients could continue stable baseline use of methotrexate (≤25 mg/week), sulfasalazine (≤3 g/day), hydroxychloroquine (≤400 mg/day) or leflunomide (≤20 mg/day); oral corticosteroids (≤10 mg/day prednisone or equivalent); and NSAIDs/other analgesics.
DISCOVER-1 (Clinicaltrials.gov identifier-NCT03162796) was conducted per Declaration of Helsinki and Good Clinical Practice guidelines. The protocol was approved by each site’s ethical body.
Procedures
Study visits were scheduled at screening, Q4W from Week0–52 and Week60 (safety follow-up). Independent assessors (distinct from investigator and consistent throughout each patient’s study participation) evaluated joints for tenderness (n=68) and swelling (n=66). Patients reported pain (0–10 cm), global disease activity (0–10 cm) and physical function (Health Assessment Questionnaire-Disability Index (HAQ-DI; 0–3)). Investigators determined global disease activity (0–10 cm), serum CRP and severity of skin symptoms using the Investigator’s Global Assessment of psoriasis (IGA; total score, 0 (cleared) to 4 (severe)) and the Psoriasis Area and Severity Index (PASI; total score, 0–72); in all cases, higher scores indicated worse status. The 36-item Short-Form Health Survey (SF-36) physical and mental component summary (PCS and MCS) scores assessed health-related quality of life (HRQoL); increased scores indicated improved HRQoL.
Suicidal ideation/behaviour or non-suicidal self-injurious behaviour was documented using electronic Columbia-Suicide Severity Rating Scale (eC-SSRS) Questionnaires, an instrument validated to assess these symptoms in clinical and research settings.16 Adverse events (AEs) and routine clinical laboratory parameters were monitored. Guselkumab pharmacokinetic and immunogenicity assessments were previously detailed.14
Outcomes
Outcomes assessed through Week52 included American College of Rheumatology≥20%/50%/70% improvement (ACR20/ACR50/ACR70) responses; IGA (score=0/1 and ≥2-grade improvement) and PASI ≥75%/90%/100% improvement (PASI75/PASI90/PASI100) responses in patients with ≥3% body surface area (BSA) and IGA ≥2 at baseline; HAQ-DI change from baseline and response (reduction ≥0.35 in patients with baseline HAQ-DI ≥0.35); changes from baseline SF-36 PCS and MCS scores; and achievement of minimal disease activity (MDA) or very low disease activity composite end points.17 18
Safety outcomes included AEs, serious AEs (SAEs), AEs necessitating study drug discontinuation, infections, serious infections, injection-site reactions (ISRs; investigator-identified unfavourable sign at injection site), malignancies, major adverse cardiovascular events (MACEs; cardiovascular death, non-fatal myocardial infarction, non-fatal stroke), suicidal ideation/behaviour (per eC-SSRS Questionnaire16 or reported AEs) and laboratory abnormalities per National Cancer Institute Common Terminology Criteria for AEs (NCI-CTCAE).
Data analyses
DISCOVER-1 sample size estimation was previously reported.14 All patients received guselkumab, with no formal hypothesis testing, post-Week24.
Treatment failure rules were applied to clinical efficacy analyses through Week24 as previously reported.14 The analytical plan prespecified summarising observed efficacy data for patients continuing post-Week24 (n=362). We also evaluated clinical efficacy in all treated patients by randomised group (n=381) with post hoc application of missing data imputation rules. In these analyses, missing binary data were imputed as non-response; missing continuous data were generally imputed as no change from baseline after treatment discontinuation or by using multiple imputation (assuming missing at random). Thus, the PBO→Q4W group included 114 patients who crossed over to guselkumab 100 mg Q4W, as well as 12 patients who received only placebo before discontinuing study agent and had missing data imputed at Week52. Imputed results are the focus of this paper; observed ACR responses are also presented.
AEs were summarised for treated patients. To account for the shorter placebo (24 weeks) than active (52 weeks) treatment periods, incidences per 100 patient-years of follow-up (100PY) and exact 95% CIs were determined for AEs, SAEs, AEs causing study agent discontinuation, infections and serious infections. These determinations assumed a constant incidence over time, a customary approach to standardise AE data for comparative purposes. Numbers of patients requiring treatment for an additional AE (number needed to harm (NNH)), were determined for these AE categories as previously detailed,19 with the intent of reporting only positive values, that is, those suggesting excess risk with guselkumab over placebo.
Results
Patient disposition and characteristics
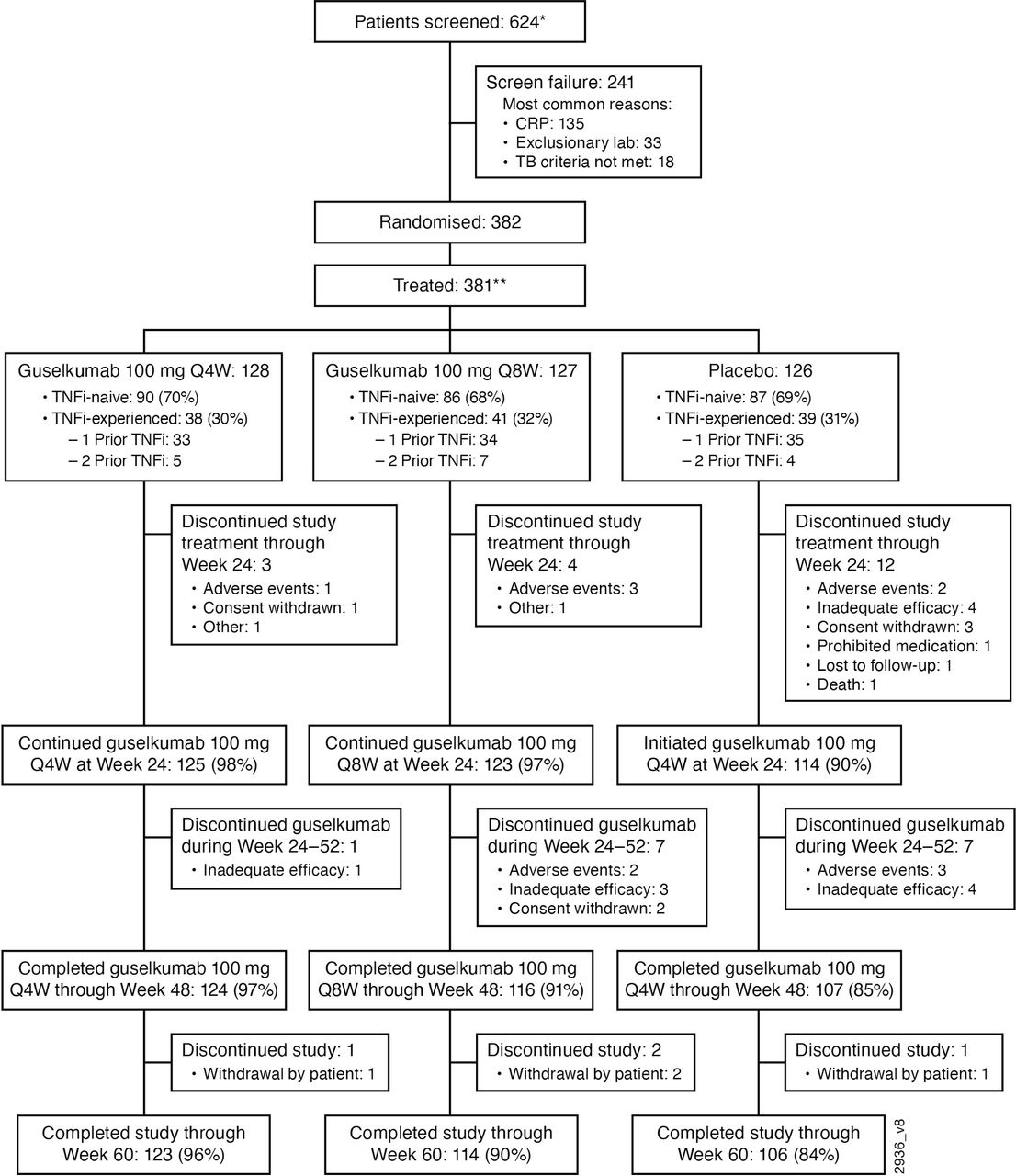
Ninety per cent (343/381) of treated patients completed the study. The most common reasons for discontinuing study agent were inadequate response (3%, 12/381) or AEs (3%, 11/381) (figure 1). Among 255 patients starting guselkumab at Week0, 240 (94%) completed study agent through Week48. The 369 guselkumab-treated patients, including 114 patients who crossed over from PBO→Q4W, were followed an average of 51.6 weeks (combined overall exposure: 365PY).
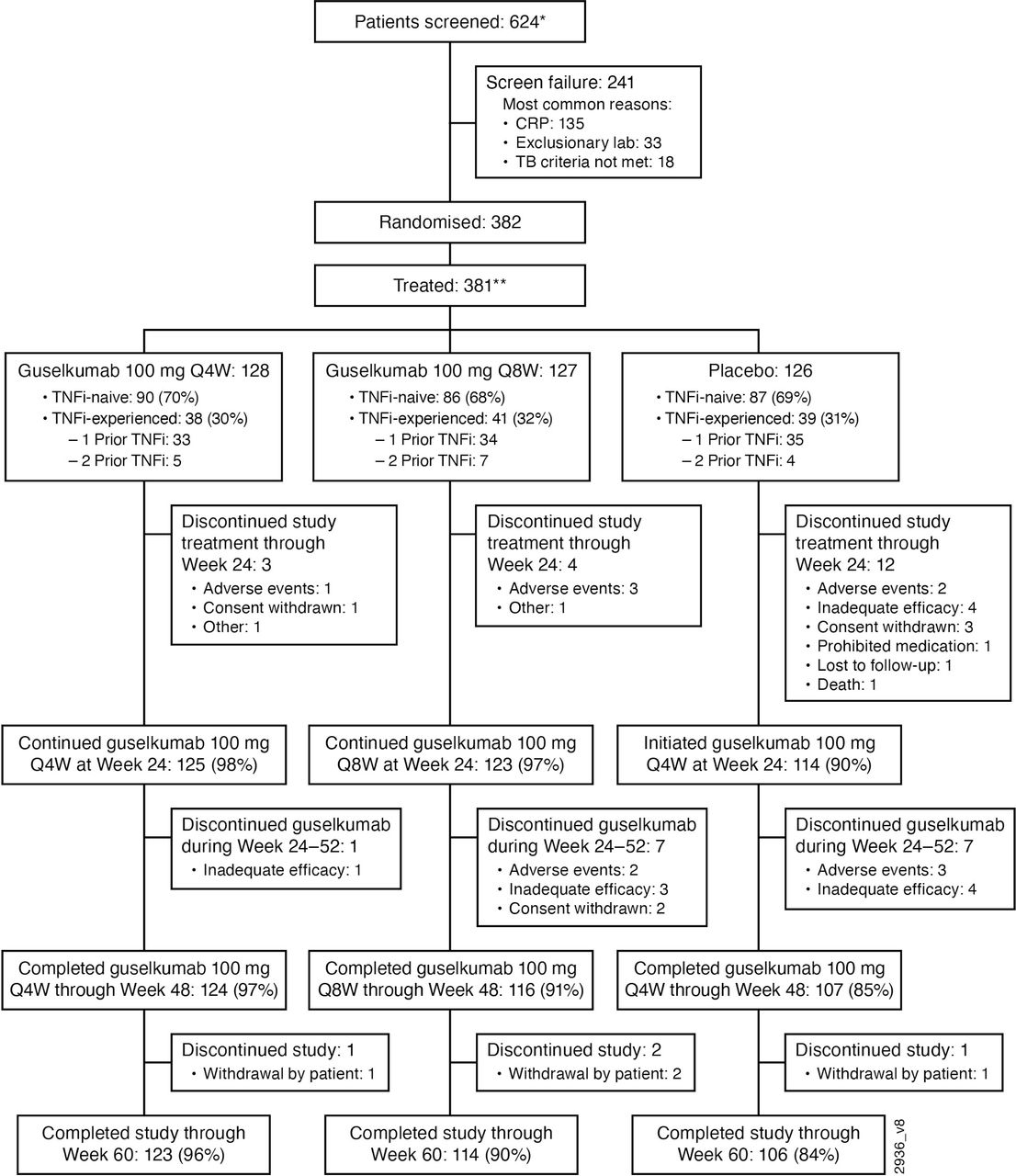
Disposition of patients through Week60 of the DISCOVER-1 rial. CRP, C reactive protein, TB, tuberculosis, TNFi, tumour necrosis factor inhibitor, Q4/8W, every 4/8 weeks. *One patient was accidentally randomly assigned before completion of the screening assessments. Subsequently, this patient did not pass screening and was later re-screened and randomly assigned using a new patient number. **One patient randomised to guselkumab 100 mg Q8W was not treated.
Baseline characteristics and medication use were generally similar across randomised treatment groups.14 Thirty-one per cent (118/381) of participants had previously received one (102 (27%)) or two (16 (4%)) TNFis (figure 1), of whom 37% (44/118) discontinued prior TNFi use due to inadequate response. TNFi-experienced patients appeared to have longer-standing and more active disease, higher levels of systemic inflammation and greater functional impairment than TNFi-naïve patients. Numerically higher proportions of TNFi-experienced than TNFi-naïve patients were obese, had more extensive skin involvement and were taking methotrexate at baseline (table 1).
Summary of baseline patient and disease characteristics for DISCOVER-1 patients by TNFi status
Pharmacokinetics and immunogenicity
Supplemental material
Supplemental material
Efficacy
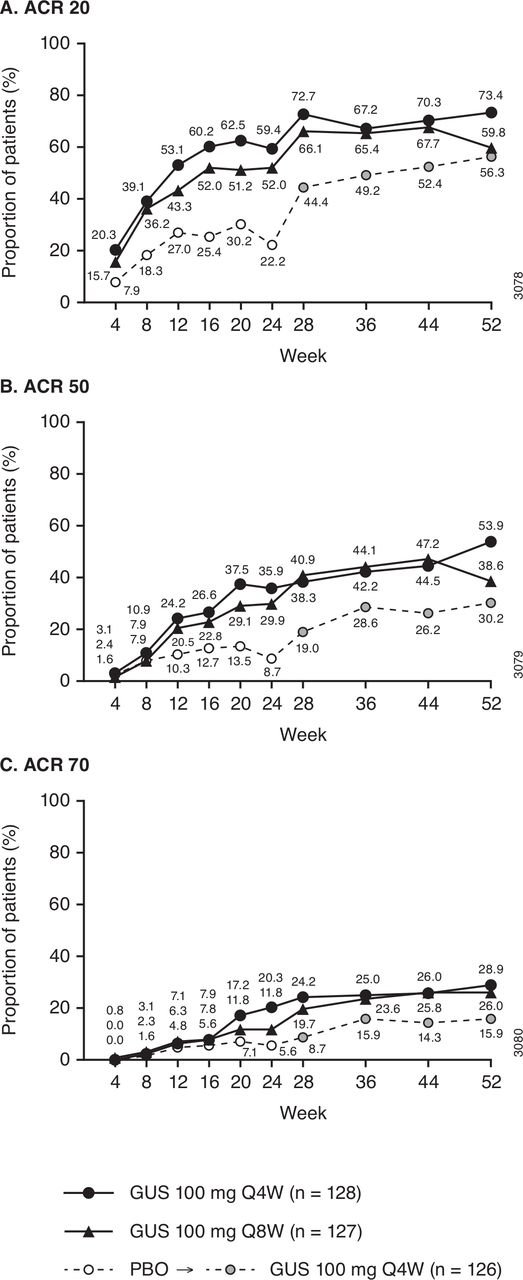
As reported previously, the DISCOVER-1 primary end point was met, with significantly greater proportions of guselkumab Q4W-treated (59%) and Q8W-treated (52%) than placebo-treated (22%) patients achieving ACR20 response at Week24 (both p<0.0001).14 Numerical improvements in ACR20 response rates were observed after Week24 through Week52, when they were 73% (94/128) and 60% (76/127), respectively, in guselkumab Q4W-randomised and Q8W-randomised patients (figure 2A). Approximately half of guselkumab-randomised patients achieved ACR50 and more than a quarter achieved ACR70 responses at Week52 (figure 2B,C). Consistent patterns were seen for observed ACR response rates (online supplemental figure S1).
Supplemental material

Proportions of randomised and treated patients achieving ACR20, ACR50 and ACR70 responses through Week52. ACR20 (A), ACR50 (B), ACR70 (C) response rates derived with application of data-handling rules (see Methods). Previously reported data through Week2414 included for reference. Of 126 patients randomised to receive placebo, 114 crossed over to guselkumab 100 mg Q4W (after Week24 response assessments); the 12 patients who received only placebo before discontinuing study agent were included as non-responders through Week52. ACR20/ACR50/ACR70, American College of Rheumatology ≥20%/50%/70% improvement responses; GUS, guselkumab; PBO, placebo; Q4/8W, every 4/8 weeks.
Across prior TNFi cohorts, the proportions of guselkumab-randomised patients achieving ACR20, ACR50 and ACR70 responses were maintained from Week24 to Week52 (figure 3). Consistent response patterns were also seen in the smaller number of patients who discontinued prior TNFi use because of inadequate response; for example, in guselkumab Q4W-randomised and Q8W-randomised patients, respective Week52 response rates were 82% (14/17) and 60% (9/15) for ACR20, and 47% (8/17) and 40% (6/15) for ACR50.

Proportions of randomised and treated patients achieving ACR20, ACR50 and ACR70 responses through Week52 by prior TNFi use. Response rates derived with application of data-handling rules (see Methods). Panels (A), (C) and (E) summarise response in TNFi-naive patients; panels (B), (D) and (F) summarise response in TNFi-experienced patients. Previously reported data through Week2414 included for reference. Among 87 TNFi-naïve and 39 TNFi-experienced patients randomised to receive placebo, 82 and 32, respectively, crossed over to guselkumab 100 mg Q4W (after Week24 response assessments); the remaining patients (5 TNFi-naïve, 7 TNFi-experienced) who received only placebo before discontinuing study agent were included as non-responders through Week52. ACR20/ACR50/ACR70, American College of Rheumatology ≥20%/50%/70% improvement responses; GUS, guselkumab; PBO, placebo; Q4/8W, every 4/8 weeks; TNFi, tumour necrosis factor inhibitor.
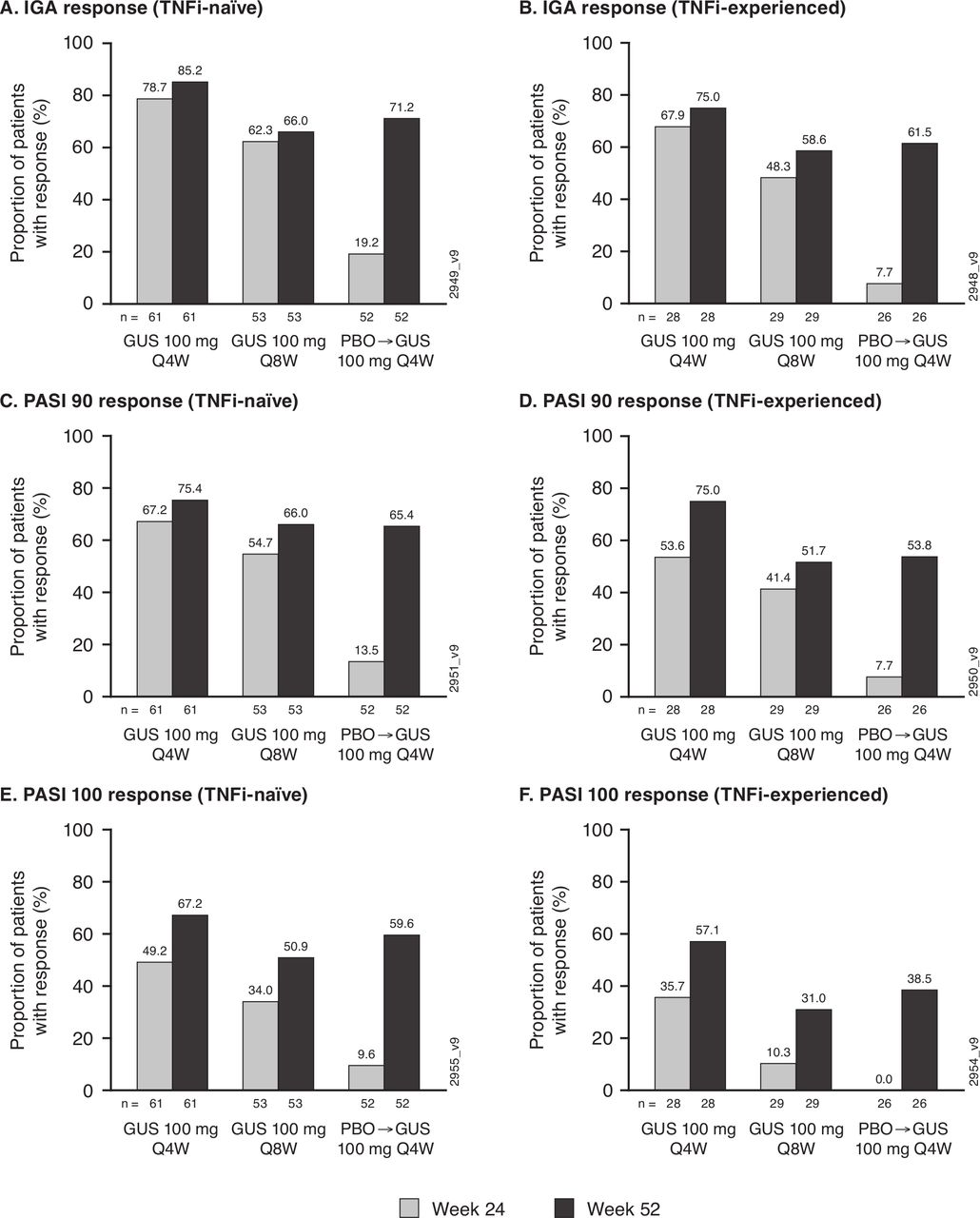
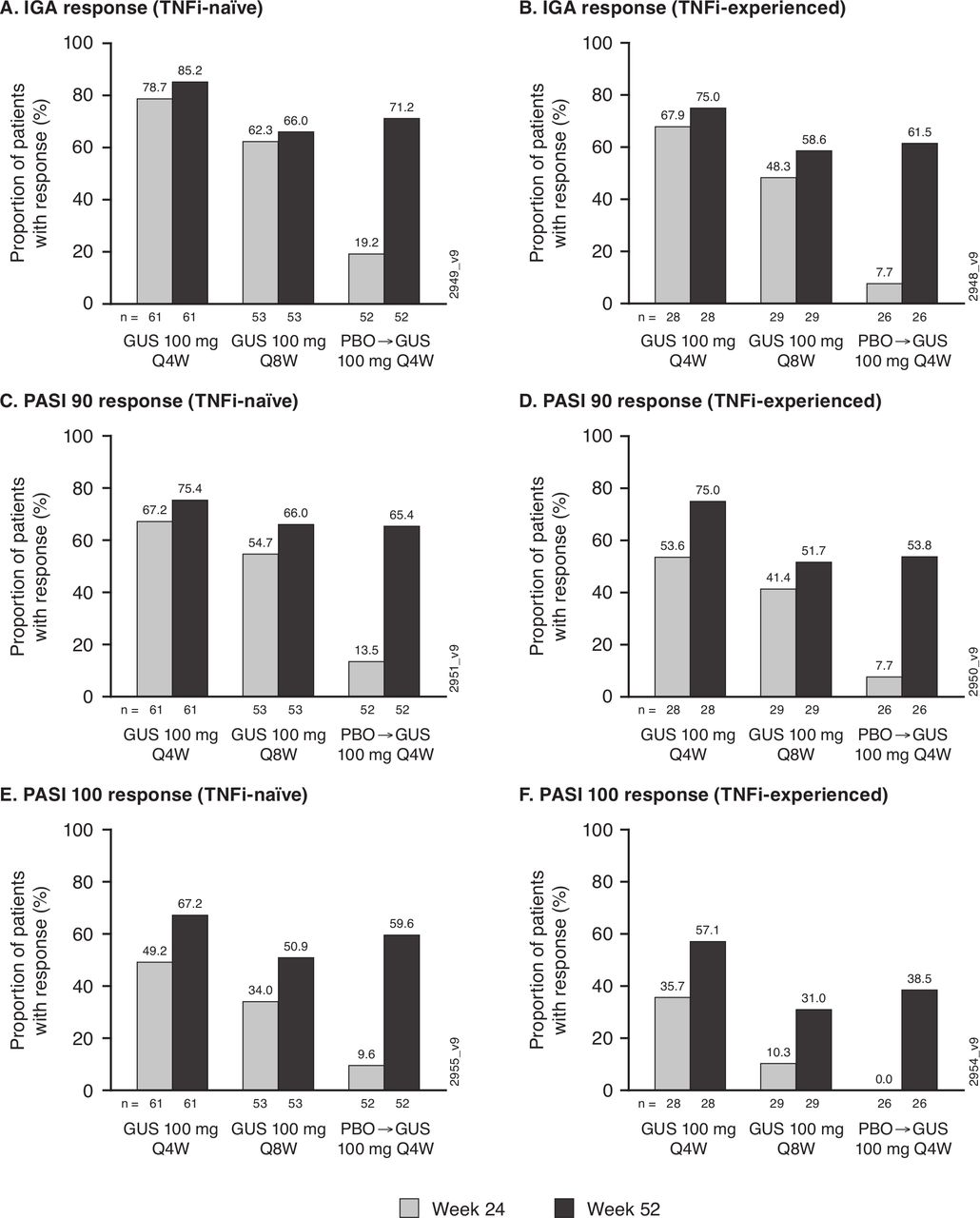
At baseline, nearly two-thirds of participants had ≥3% BSA psoriasis involvement and IGA ≥2 (table 1). An IGA 0/1 response, indicating clear/almost clear skin, was achieved by 82% (73/89) and 63% (52/82), including 66% (59/89) and 49% (40/82) of patients with IGA 0 (clear skin), respectively, of these guselkumab Q4W-randomised and Q8W-randomised patients at Week52. Respective PASI 90 (75% and 61%) and PASI100 (64% and 44%) response rates also indicated maintenance of skin response through Week52 (figure 4). Robust skin response rates were maintained at Week52 regardless of prior TNFi use (figure 5).

Proportions of randomised and treated patients with ≥3% BSA psoriasis and IGA ≥2 at Week 0 achieving skin responses through Week 52. IGA 0/1 + ≥2-grade decrease from baseline (A), IGA 0 (B), PASI 90 (C), PASI 100 (D) and PASI 75 (E) response rates derived with application of data handling rules (see Methods). Previously reported Week24 data14 included for reference. Of 78 patients randomised to receive placebo who had ≥3% BSA psoriasis involvement and IGA ≥2 at baseline, 68 crossed over to guselkumab 100 mg Q4W (after Week24 response assessments); the 10 patients who received only placebo before discontinuing study agent were included as non-responders at Week52. BSA, body surface area; GUS, guselkumab; IGA, Investigator’s Global Assessment; PASI, Psoriasis Area and Severity Index; PBO, placebo; Q4/8W, every 4/8 weeks.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportions of randomised and treated patients with ≥3% BSA psoriasis and IGA ≥2 at Week0 achieving IGA (IGA 0/1 +≥2-grade decrease from baseline), PASI 90 and PASI 100 responses at Week24 and Week52 by prior TNFi use. Panels (A), (C) and (E) summarise response in TNFi-naïve patients; panels (B), (D) and (F) summarise response in TNFi-experienced patients. Response rates derived with application of data handling rules (see Methods). Among 52 TNFi-naïve and 26 TNFi-experienced patients randomised to receive placebo, 47 and 21, respectively, crossed over to guselkumab 100 mg Q4W (after the Week24 response assessments); the remaining patients (five in each TNFi subgroup), who received only placebo and discontinued from the study, were included as non-responders at Week52. BSA, body surface area; GUS, guselkumab; IGA, Investigator’s Global Assessment; PASI, Psoriasis Area and Severity Index; PBO, placebo; Q4/8W, every 4/8 weeks; TNFi, tumour necrosis factor inhibitor.
Improvements in physical function at Week24 were sustained in guselkumab Q4W-randomised and Q8W-randomised patients (HAQ-DI least squares (LS) mean changes at Week52: −0.5 and −0.4, respectively). Nearly 60% of guselkumab-randomised patients with a baseline HAQ-DI score ≥0.35 saw clinically meaningful improvement (≥0.35) at Week52. Proportions of guselkumab-randomised patients achieving HAQ-DI ≥0.35 improvement were comparable between prior TNFi cohorts and maintained through Week52 (table 2).
Summary of patient-reported and composite outcome measures through Week52 of the DISCOVER-1 tTrial
Physical aspects of HRQoL continued to numerically improve through Week52 among guselkumab Q4W-randomised and Q8W-randomised patients (SF-36-PCS LSmean changes: 8.6 and 6.6, respectively). Improvements in mental components of HRQoL were maintained through Week52 (SF-36 MCS LSmean changes: 4.3 and 4.4, respectively) (table 2).
When efficacy was assessed with a validated composite index, 39% of 128 guselkumab Q4W-randomised and 30% of 127 guselkumab Q8W-randomised patients achieved MDA at Week52 (table 2). Although attained by numerically higher proportions of TNFi-naïve patients, MDA response rates continued to numerically improve through 1 year in both TNFi-exposure cohorts.
Across clinical outcomes, response rates seen in the PBO→Q4W group at Week52, including ACR20: 56%; IGA 0/1: 68%; HAQ-DI response: 45.5%; and MDA: 25%, were consistent with other guselkumab-treated patients after a similar period of treatment (table 2; figures 2–5 and online supplemental figure S1).
Safety
Through Week60, 63% of 369 guselkumab 100 mg-treated patients had AEs, occurring in similar proportions of guselkumab Q4W-randomised and Q8W-randomised patients (table 3). For each AE category assessed, all NNH statistics comparing guselkumab to placebo were negative.
Summary of patients with AE categories of interest through Week60 of the DISCOVER-1 rial
Consistent with the placebo-controlled period,14 the most commonly reported AEs through Week60 were nasopharyngitis (11% and 16%, respectively, in Q4W-randomised and Q8W-randomised patients), upper respiratory tract infection (12% and 8%), increased alanine aminotransferase (ALT) (both 7%) and increased aspartate aminotransferase (AST) (5% and 9%).
No guselkumab-treated patient died or had a MACE. One placebo-treated patient, who was receiving prednisone and methotrexate at baseline, died of cardiac failure,14 and another who received placebo plus methotrexate died of pneumonia.
Through Week60, 4% (16/369) of guselkumab-treated patients had SAEs (table 3). Eight of 16 (50%) guselkumab-treated patients with SAEs were receiving methotrexate, two (12%) received leflunomide and six (38%) did not use any non-biologic DMARD. All SAEs were singular events. Most SAEs resolved by Week60; exceptions were plasma cell myeloma as previously reported14 and acute venous iliofemoral thrombosis diagnosed at Week36 in an elderly individual receiving guselkumab 100 mg Q4W. Aside from the case of multiple myeloma (see below), no SAE required guselkumab discontinuation.
Regarding malignancies, beyond the previously reported multiple myeloma (diagnosed 15 days after one dose of guselkumab 100 mg in a Q8W-randomised patient),14 a single patient had two malignancies reported at Week36, 12 weeks after crossing over from PBO→Q4W (squamous cell skin carcinoma and malignant melanoma in an elderly individual with personal history of squamous cell carcinoma in situ and family history of melanoma). Study agent was discontinued, the melanoma was treated with wider excision and both AEs were considered resolved.
Few guselkumab-treated patients (2%) discontinued study agent due to AEs. No serious infections were reported through Week24;14 1% (4/369) of guselkumab-treated patients had serious infections during Weeks24–60 (table 3). All serious infections resolved, and none necessitated study agent discontinuation. No patient had uveitis, active tuberculosis, or an opportunistic infection. One guselkumab-treated patient, with a history of asthma and concomitant inhaled corticosteroid use, had a mild, non-serious case of oral thrush. No AE of inflammatory bowel disease was reported in a guselkumab-treated patient, and no events of suicidal behaviour or self-injurious behaviour without suicidal intent were reported (see online supplemental file).
Through Week60, ISRs occurred in four (3%), two (2%) and two (2%) patients in the guselkumab Q4W, guselkumab Q8W and PBO→Q4W groups, respectively. All ISRs were mild; none required study agent discontinuation. No anaphylactic, serum sickness or serum sickness-like reaction was reported.
Relatively few patients had clinically meaningful postbaseline abnormalities in laboratory values through Week60 (online supplemental table S1). For neutrophil, leucocyte and platelet counts, no further mean decreases after Week24 and no dose-related trends were observed through 1 year of guselkumab. NCI-CTCAE grade ≥2 decreased neutrophil counts generally (see online supplemental table S1 for exceptions) were not associated with infections, resolved spontaneously without treatment and did not necessitate study agent discontinuation. With one exception (see online supplemental table S1), NCI-CTCAE grade ≥2 elevations in ALT or AST concentrations in guselkumab-treated patients were not associated with total bilirubin elevations. No elevation satisfied the criteria for Hy’s Law (total bilirubin >2 × upper limit of normal (ULN) and either ALT or AST ≥3 × ULN) in guselkumab-treated patients through Week60. The majority of ALT and AST elevations were transient, resolved and did not require study agent discontinuation. Among patients with baseline values at or below the ULN, ALT and AST concentrations increased to above the ULN in 32% (64/200) and 27% (54/200), respectively, of guselkumab-treated patients receiving methotrexate and in 26% (43/167) and 24% (40/166), respectively, of those not receiving methotrexate, at baseline. Total bilirubin increases in guselkumab-treated patients were NCI-CTCAE grade ≤2, not associated with direct bilirubin elevation, and generally <2 × ULN (see online supplemental table S1 for exceptions).
In guselkumab-treated TNFi-naïve (n=258) and TNFi-experienced (n=111) patients, 62% and 64%, respectively, reported ≥1 AE, 3% and 6% had SAEs, 0.4% and 3% had serious infections, 3% and 2% had AEs that led to treatment discontinuation, 7% and 4% had AEs of increased ALT levels, and 7% and 3% had AEs of increased AST levels through Week60.
Discussion
PsA, a clinically diverse, chronic, inflammatory disorder driven by excess IL-23/Th17-mediated cytokines, commonly requires targeted treatment to attain minimal disease activity. Guselkumab, a fully human monoclonal antibody, potently binds the IL-23p19 subunit. In this guselkumab evaluation, the significantly better response rates observed at Week24 across arthritis/psoriatic skin symptoms, patient-reported outcomes and composite end points were maintained, and often numerical improvements continued, through Week52. Approximately two-thirds of guselkumab-randomised patients achieved ACR20, approximately half achieved ACR50 and more than a quarter achieved ACR70 responses at Week52. Increases in ACR50 and ACR70 response rates suggested achievement of stringent treatment targets may continue over time. Taken together, findings—which were conservatively determined by imputing missing data—indicate guselkumab 100 mg Q4W or Q8W provided meaningful and sustained clinical improvements in PsA through 1 year.
TNFi, the current standard of care for severe disease and difficult-to-treat soft tissue manifestations20 when non-biologic treatments are ineffective,21 22 may be of limited use in patients with inadequate/loss of response or AEs.23 Guselkumab 100 mg Q4W and Q8W have been shown to effectively treat such manifestations,15 with maintenance of dactylitis and enthesitis resolution rates through 1 year.19
Nearly a third of DISCOVER-1 participants previously received one or two TNFis, permitting guselkumab efficacy and safety evaluations across TNFi-exposure cohorts. At baseline, the smaller TNFi-experienced cohort was characterised by longer-standing and more active joint disease, higher levels of systemic inflammation, greater functional impairment, and more patients with extensive skin involvement and methotrexate use, than TNF-naïve patients. Nonetheless, improvements in joint and skin symptoms were maintained, and in some cases response rates continued to numerically improve, through 1 year in both TNFi-exposure cohorts. Moreover, more than half of both TNFi-naïve and TNFi-experienced patients receiving guselkumab Q4W or Q8W maintained clinically important improvements in physical function,24 and many achieved MDA, at 1 year.
Guselkumab’s novel mechanism, that is, binding to IL-23’s p19 subunit but not the p40 subunit it shares with IL-12, has demonstrated a favourable benefit-risk profile in patients with psoriasis through up to 4 years of treatment.25 26 The favourable benefit-risk profile suggested by DISCOVER-1 safety data through Week2414 was supported by findings through Week60, representing 365PY, and was consistent across TNFi-exposure cohorts. Relative to time-adjusted AE incidences (per 100PY) associated with placebo through Week24, guselkumab treatment through 1 year did not increase SAEs or serious infections. In fact, all NNH values comparing AE incidences for guselkumab versus placebo were negative. The one case of melanoma occurred in an individual with personal and family history of skin cancer. Reassuringly, no patient with psoriasis developed melanoma through 1 year of guselkumab treatment, and no new safety concerns were seen through 4 years, in the phase III VOYAGE-1 and VOYAGE-2 trials.26–28 No guselkumab-treated patient developed active tuberculosis, opportunistic infection or inflammatory bowel disease. These safety findings mirrored those through 1 year of the phase III, active-comparator, ECLIPSE study of guselkumab versus secukinumab in patients with psoriasis, in which no guselkumab-treated patients reported AEs of inflammatory bowel disease or opportunistic infection,29 and were consistent with the long-term guselkumab safety profile established in psoriasis.25 26 Thus, this anti-IL-23p19 inhibitor may offer a valuable alternative treatment option for both TNFi-naïve and TNFi-experienced individuals with PsA.
Approximately 94% of guselkumab-randomised patients completed study agent through 1 year. This robust patient retention is consistent with the 91% of patients with psoriasis completing guselkumab 100 mg Q8W through 1 year in VOYAGE-1.28 Real-world data for guselkumab treatment persistence in psoriasis are currently limited. In a single-centre retrospective chart review, 92% (11/12) of patients with psoriasis continued guselkumab at study completion, during which time guselkumab treatment duration averaged 6 months.30 Real-world retention of patients with PsA receiving injectable TNFi or anti-IL-12/23 biologics has been reported as 44% at 1 year and 20% at 2 years.31 32
Clinical efficacy, safety and patient retention through 1 year of DISCOVER-1 are consistent with 1-year findings from the larger DISCOVER-2 trial of 739 biologic-naïve patients with PsA, in which significant improvements in arthritis symptoms, skin disease, dactylitis and enthesitis (pooled across studies), physical function, and physical aspects of HRQoL seen at Week24 were maintained by both guselkumab 100 mg Q4W and Q8W, and 94% of guselkumab-randomised patients also completed study agent, through 1 year.19 The DISCOVER trials are the first to document retention of patients with PsA receiving an IL-23p19 inhibitor through 1 year. While DISCOVER-1 did not evaluate radiographic progression, guselkumab 100 mg Q4W significantly inhibited structural damage progression at Week24 of DISCOVER-2,15 and low, comparable levels of progression were seen with 1 year of guselkumab 100 mg Q4W or Q8W in that study.19
Results of DISCOVER-1 are limited by the 1-year study period, a relatively short time frame for assessing patient retention, maintenance of effect and tolerability in a chronic lifelong disorder. Conclusions drawn are also limited by the lack of placebo control beyond Week24. Reassuringly, guselkumab safety observed in this study, and through 1 year of DISCOVER-2,19 are consistent with safety profiles established for longer periods of treating patients with psoriasis with IL-23p19 inhibitors.25 26 33 Forthcoming 2-year findings from DISCOVER-2 will extend knowledge about the benefit-risk profile of this first-in-class biologic in PsA.
Thus, DISCOVER-1 findings indicate that guselkumab 100 mg provided meaningful and sustained improvements across multiple clinical manifestations of PsA, alongside a favourable benefit-risk profile, regardless of dosing interval or prior TNFi use.
Data availability statement
The data sharing policy of Janssen Pharmaceutical Companies of Johnson & Johnson is available at https://www.janssen.com/clinical-trials/transparency. As noted on this site, requests for access to the study data can be submitted through the Yale Open Data Access (YODA) Project site at http://yoda.yale.edu.
Ethics statements
Patient consent for publication
Ethics approval
The governing ethical bodies for each of the 86 participating sites approved the DISCOVER-1 Study protocol.
Acknowledgments
The authors thank Diane D Harrison MD MPH (consultant funded by Janssen) for substantive manuscript review, Michelle Pupek BS (Janssen employee) for programming support and Michelle L Perate MS (Janssen employee) for assistance with manuscript preparation and submission. Part of this work was previously presented at the EULAR 2020 E-Congress: McInnes IB, Rahman P, Gottlieb AB, et al. Efficacy and safety of guselkumab, a monoclonal antibody specific to the p19-subunit of interleukin-23, through week 52 of a phase 3, randomized, double-blind, placebo-controlled study conducted in biologic-naïve patients with active psoriatic arthritis. Ann Rheum Dis 2020;79 (Suppl 1):1148.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors Substantial intellectual contribution to conception and design, or acquisition of data, or analysis and interpretation of data: CTR, PSH, W-HB, ERS, ECH, APK, SDC, FZ, RAS, XLX, QCZ, SS, YJ, PA, BZ, YZ, MS, CSK, AD. Drafting the article or revising it critically for important intellectual content: CTR, PSH, W-HB, ERS, ECH, APK, SDC, FZ, RAS, XLX, QCZ, SS, YJ, PA, BZ, YZ, MS, CSK, AD. Final approval of the version to be published: CTR, PSH, W-HB, ERS, ECH, APK, SDC, SDC, FZ, RAS, XLX, QCZ, SS, YJ, PA, BZ, YZ, MS, CSK, AD. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: CTR, PSH, W-HB, ERS, ECH, APK, SDC, FZ, RAS, XLX, QCZ, SS, YJ, PA, BZ, YZ, MS, CSK, AD.
Funding Janssen Research & Development, LLC funded this study.
Competing interests CTR has received research funding from AbbVie, Amgen and UCB; and serves as a consultant for AbbVie, Amgen, Janssen, Eli Lilly, Novartis, Pfizer and UCB. PSH has received grants and research support paid to Leeds Teaching Hospitals Charitable Foundation from AbbVie, Janssen and Novartis; and honoraria or consultation fees paid to Leeds Teaching Hospitals Charitable Foundation from AbbVie, Amgen, Pfizer, and UCB and to himself from Celgene and Galapagos. W-HB has received honoraria as a speaker or advisor from AbbVie, Almirall, Celgene, Eli Lilly, Janssen, Leo, Novartis and UCB; and he has received a research grant from Pfizer to investigate the role of JAK inhibition in psoriasis. ERS has received honoraria as speaker or advisor from AbbVie, Amgen, BMS, Celgene, Janssen, Eli Lilly, Novartis, Pfizer, Roche, Sanofi, and UCB, and received research grants from Glaxo, Novartis, Pfizer and Roche. ECH, APK, SDC, FZ, RAS, XLX, QCZ, SS, PA, BZ, YZ, MS and CSK are employed by Janssen (a subsidiary of Johnson & Johnson) and own Johnson & Johnson stock and/or stock options. YJ is a consultant funded by Janssen Research & Development. AD has received grants and research support paid to his university from AbbVie, Eli Lilly, GlaxoSmithKline, Novartis, Pfizer and UCB; and honoraria or consultation fees from AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Janssen, Novartis, Pfizer and UCB.
Provenance and peer review Not commissioned; externally peer reviewed.