Article Text

Abstract
Aim To present a systematic literature review (SLR) on efficacy, immunogenicity and safety of vaccination in adult patients with autoimmune inflammatory rheumatic diseases (AIIRD), aiming to provide a basis for updating the EULAR evidence-based recommendations.
Methods An SLR was performed according to the standard operating procedures for EULAR-endorsed recommendations. Outcome was determined by efficacy, immunogenicity and safety of vaccination in adult patients with AIIRD, including those receiving immunomodulating therapy. Furthermore, a search was performed on the effect of vaccinating household members of patients with AIIRD on the occurrence of vaccine-preventable infections in patients and their household members (including newborns). The literature search was performed using Medline, Embase and the Cochrane Library (October 2009 to August 2018).
Results While most investigated vaccines were efficacious and/or immunogenic in patients with AIIRD, some were less efficacious than in healthy control subjects, and/or in patients receiving immunosuppressive agents. Adverse events of vaccination were generally mild and the rates were comparable to those in healthy persons. Vaccination did not seem to lead to an increase in activity of the underlying AIIRD, but insufficient power of most studies precluded arriving at definite conclusions. The number of studies investigating clinical efficacy of vaccination is still limited. No studies on the effect of vaccinating household members of patients with AIIRD were retrieved.
Conclusion Evidence on efficacy, immunogenicity and safety of vaccination in patients with AIIRD was systematically reviewed to provide a basis for updated recommendations.
- infections
- vaccination
- autoimmune diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Patients with autoimmune inflammatory rheumatic diseases (AIIRD) are at increased risk of vaccine-preventable infections and associated complications.
Vaccination may be less efficacious in (subgroups of) patients with AIIRD and could potentially lead to exacerbation of underlying disease.
Evidence-based recommendations of the EULAR for vaccination of adult patients with AIIRD were published in 2011.
What does this study add?
This systematic literature review summarises available evidence on efficacy, immunogenicity and safety of vaccination in AIIRD since October 2009, providing a basis for updated EULAR recommendations.
How might this impact on clinical practice?
The aim of the updated recommendations is to aid health professionals dealing with questions regarding vaccination in patients with AIIRD, whereby reducing infection-related morbidity and mortality.
Introduction
Infectious diseases and associated complications comprise an important cause of morbidity and mortality in patients with autoimmune inflammatory rheumatic diseases (AIIRD). Increased susceptibility to infectious diseases in these patients is most likely due to an immunomodulating effect of the disease itself and/or by use of immunosuppressive medications.1
Vaccination is generally regarded as a safe, efficacious and low-cost method for preventing certain infections. However, vaccination may be less efficacious in (subgroups of) patients with AIIRD, as a result of their immunosuppressed state, and, moreover, could potentially lead to exacerbation of the underlying AIIRD.
In 2011, evidence-based recommendations for vaccination in patients with AIIRD were published. They were formulated by an EULAR task force to aid health professionals dealing with questions regarding vaccination in patients with AIIRD in daily clinical practice, with the aim of reducing infection-related morbidity and mortality in these patients.2 The authors stated that the recommendations needed to be updated on a regular basis as new evidence becomes available.2 Towards this end, the League commissioned another multidisciplinary task force with the purpose of formulating up-to-date recommendations for vaccination in patients with AIIRD.
The current report presents the results of an SLR on efficacy, immunogenicity and safety of vaccination in adult patients with AIIRD, including those using immunomodulating agents. Together with the results of an SLR on incidence and prevalence of VPIs in patients with AIIRD,1 the current SLR provided the task force with a basis for updating the recommendations.3
Methods
The work was performed in accordance with the 2014 EULAR standard operating procedures for EULAR-endorsed recommendations.4
The expert committee first formulated four main research questions (Box 1), based on the 2011 version of the recommendations. The current review reports on the SLR results of three of these four questions, which include the topics of efficacy, immunogenicity and safety of vaccination in adult patients with AIIRD (including those receiving immunosuppressive agents) and the effect of vaccinating their household members on the occurrence of VPIs in both patients and their household members (including newborns). The efficacy of vaccination was defined as the capacity to prevent infections, while the immunogenicity of vaccination refers to the capacity to induce vaccine-specific humoral and/or cellular immune responses. Safety of vaccination in the AIIRD population was determined by the assessment of both the occurrence of adverse effects and the influence on the underlying disease.1
Research questions
What is the incidence or prevalence of vaccine-preventable infections (VPI) in adult patients with AIIRD?*
What is the efficacy, immunogenicity and safety of available vaccines in adult patients with AIIRD?
Are vaccines efficacious and immunogenic in adult patients with AIIRD, treated with immunosuppressive agents and disease-modifying antirheumatic drugs?
What is the effect of vaccinating household contacts of patients with AIIRD on the occurrence of VPI in both patients and household members (including newborns)?
* The systematic literature review covering research question 1 has been submitted for publication separately.1
AIIRD, autoimmune inflammatory rheumatic disease(s).
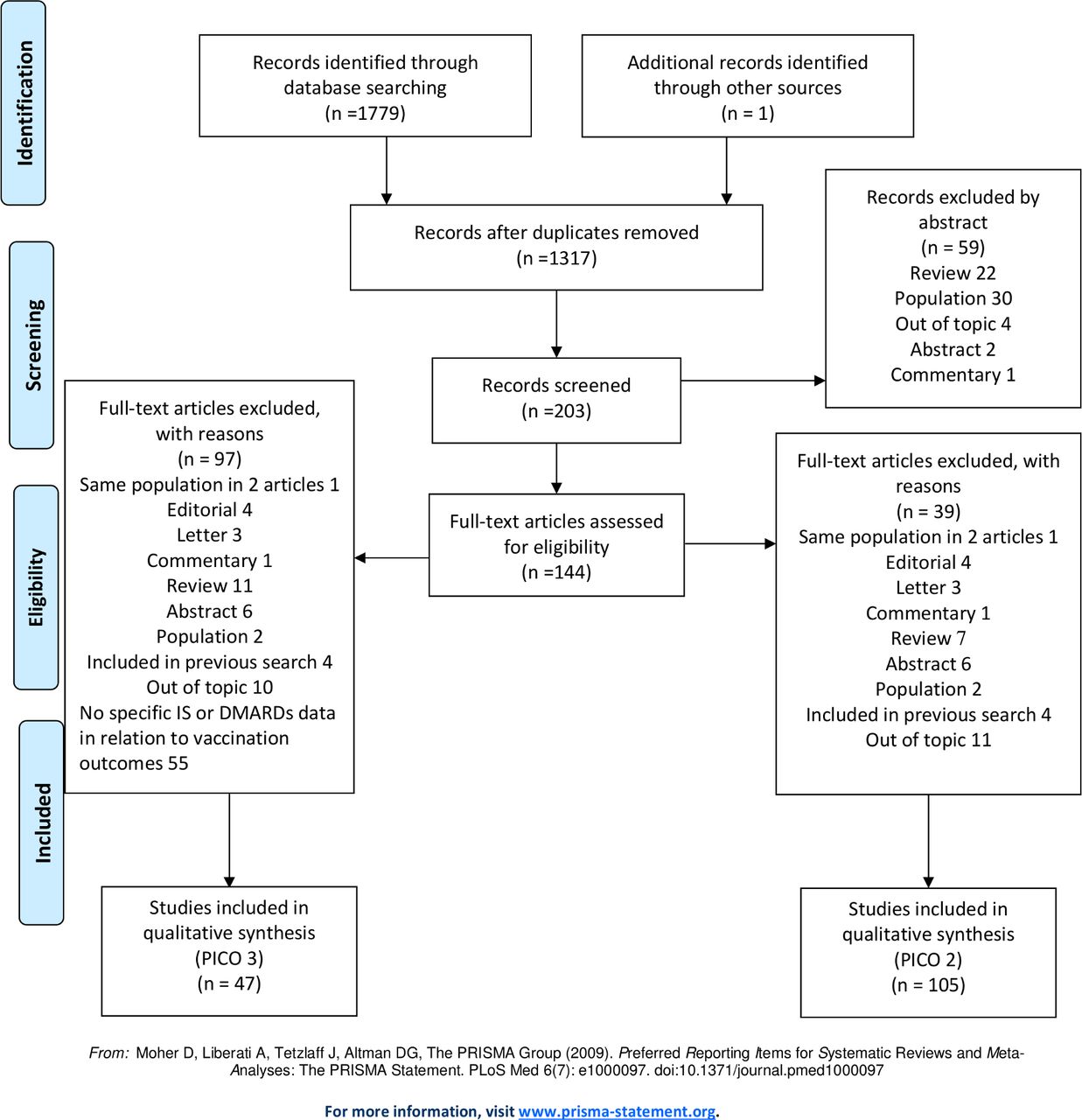
Next, the research questions were adapted according to the PICO-method (population-intervention-comparison-outcome). Population, intervention, comparison and outcome definitions were combined and adapted to be used as search terms (table 1). Medline (via Pubmed), Embase and the Cochrane Library were searched from October 2009 to August 2018. Meta-analyses, randomised trials, cohort studies and case series with at least five participants were eligible. Only English articles on adult patients (≥18 years) were included. Papers with non-original data, case reports, case series with less than five patients, abstracts presented in scientific meetings, and papers included in the previous version of these recommendations were excluded. Papers that were not retrieved in the search, but were relevant in the opinion of the committee, could be added. See figure 1 for the flow chart displaying the search strategy for PICO 2 and 3. For some of the AIIRD, immunomodulating agents and vaccines (diphteria, pertussis, measles, mumps, rubella, Neisseria meningitides, Haemophilus influenzae B and typhoid fever vaccine) that were included in the literature search, no relevant articles were retrieved. No relevant articles were retrieved in the search on the effect of vaccinating household members of patients with AIIRD (research question 4).

{kind=link}
Flow chart displaying the search strategy for PICO 2 and 3. DMARDs, disease-modifying antirheumatic drugs; IS, immunosuppressives; PICO, population-intervention-comparison-outcome.
Formulation of PICO-questions
Data analysis was performed by CR, VF, MH, SvA and OE. The following information was retrieved from all included articles: name of first author, year of publication, country where the study was performed, years of data inclusion, type of study, vaccine used, addition of adjuvant, type of AIIRD, number of participants, age and sex of participants, disease duration, time of follow-up, medication used and outcome of vaccination (efficacy, immunogenicity and/or safety). The articles were critically assessed (online supplementary file S6—included articles and critical appraisal) by applying tools from the Cochrane Library (online supplementary file S7—critical appraisal criteria) and given a level of evidence based on the Oxford Centre for Evidence-based Medicine approach (table 2). Discrepancies between reviewers were resolved by consensus. The final recommendations were graded according to the level of evidence of the underlying articles (table 3).5
Supplemental material
Supplemental material
Oxford Centre for Evidence-Based Medicine—levels of evidence
Grades of recommendation
Results
Influenza vaccination
Efficacy—immunogenicity—safety
Up to the previous recommendations, one study addressed the issue of efficacy of influenza vaccination in patients with AIIRD.6 Immunogenicity of the vaccine had been evaluated in 26 studies, mainly including patients with rheumatoid arthritis (RA), systemic lupus erythematosus (SLE) and granulomatosis with polyangiitis (GPA).7–32 Most of these studies demonstrated similar rates of immunogenicity among patients and healthy controls (HC), except for the studies in patients treated with rituximab, whose responses were severely impaired.12 14 33
From the previous recommendations up to August 2018, seven meta-analyses and 50 other studies have been published on efficacy, immunogenicity and safety of influenza vaccination, including the 2009 pandemic H1N1 influenza strain vaccine, in patients with AIIRD (table 4 for seasonal trivalent and table 5 for monovalent pandemic influenza vaccination).
Efficacy, immunogenicity and safety of trivalent influenza vaccination in patients with AIIRD (October 2009–August 2018)
Efficacy, immunogenicity and safety of monovalent (H1N1) pandemic influenza vaccination in patients with AIIRD (October 2009–August 2018)
Five studies addressed the efficacy of influenza vaccination. Retrospective database analysis studies reported a reduced all-cause mortality rate and risk of hospitalisation for influenza-related complications in patients with RA34 and SLE35 who received trivalent seasonal subunit influenza vaccine. A prospective Japanese study following a total of 17 735 patients with RA during four influenza seasons, found that trivalent subunit influenza vaccination was associated with a lower self-reported rate of influenza infections (RR 0.83, 95% CI 0.71 to 0.95).36 These findings are supported by two prospective cohort studies.6 37
Most studies on influenza vaccination in patients with AIIRD, however, address immunogenicity, mainly by assessing the development of a protective level of antibodies (titre value ≥40, as measured by the haemagglutination inhibition assay). For RA, most of these studies report similar responses in patients and HCs.7 9–15 20 38–41 A meta-analysis including a total of 886 patients with RA and 685 controls concluded that 60%, 68% and 61% of patients with RA reached seroprotective antibody levels following influenza vaccination for the H1N1, H3N2 and B strain, respectively. Only for the H1N1 influenza strain, the strain for which most data were available, responses were significantly lower in patients than in HCs.42
For SLE most studies report similar, adequate immune responses using trivalent seasonal subunit influenza vaccine,17 22–25 43 44 although modestly lower responses compared with HCs were also reported.21 26–29 Two meta-analyses reported an adequate but lower response against influenza A strains (H1N1 and H3N2) but not against influenza B in patients with SLE as compared with HCs,45 46 while another meta-analysis reported a reduced immunogenicity in SLE for H1N1 and B strains, but not for H3N2.47 Reported pooled seroprotection rates in patients with SLE are 66%–68%, 64%–76% and 60%–66% against H1N1, H3N2 and B strains, respectively.46 47
Likewise, in other AIIRD, including patients with spondyloarthropathies, antineutrophil cytoplasmic antibodies (ANCA)-associated vasculitis and primary systemic sclerosis (pSS), adequate serological responses to influenza vaccination were found.30–32 48–53
Regarding the pandemic monovalent subunit influenza vaccine, most larger studies report reduced immunogenicity in patients with AIIRD (mostly RA and SLE), although protective antibody levels were reached in the majority of patients.41 52 54–68 A second booster dose of vaccine, given 3–4 weeks after the first, improved immunogenicity, resulting in seroprotection levels comparable to those of HCs.55 62 69 This phenomenon has also been shown in patients with SLE who received seasonal influenza vaccine for the first time.70 High disease activity levels did not preclude reaching seroprotection in a study that included 340 patients with RA, of which 14.5% had a DAS 28 (Disease Activity Score in 28 joints) value above 5.1.58
Influenza vaccination did not influence activity of the underlying AIIRD in patients with RA,7 8 12 14 15 38 39 42 54 55 57 71–73 SLE,6 19 21 26 28 37 43 45–47 ANCA-associated vasculitis30 31 48 or systemic sclerosis.32 49 Adverse events of influenza vaccination in patients with AIIRD were comparable to those in HCs in most studies,7 19 21 23 30 59 65 including a meta-analysis in patients with SLE,46 In contrast, a meta-analysis including 13 studies in patients with RA concluded that local, mild adverse events occurred significantly more frequently in patients with RA.42
Influence of immunomodulating agents
The influence of immunomodulating agents on influenza vaccine efficacy and immunogenicity is summarised in table 6. No influence of methotrexate (MTX) on influenza immunogenicity was found in most studies39 40 43 62 72 74 including one meta-analysis in patients with RA.75 In some, a modest reduction in immunogenicity was observed.58–60 73 76 In another meta-analysis, results on the influence of MTX differed depending on whether response rates per influenza strain, or for at least two of the three strains, were analysed. In case of the latter approach, the negative impact of MTX was significant.77 Interestingly, temporary discontinuation of MTX was shown to significantly improve immunogenicity of seasonal influenza vaccination in patients with RA in two studies by Park et al.78 79 Discontinuation of MTX for 2 weeks after influenza vaccination led to a 11%–16% (depending on influenza strain) higher seroprotection rate compared with patients with RA who continued the use of MTX. Flare rates tended to be higher in patients with RA who temporarily halted MTX use, but the increase in disease activity was transient.78 79
Influence of disease-modifying antirheumatic drugs on influenza and pneumococcal vaccine efficacy and immunogenicity
Hydroxychloroquine does not influence the development of an adequate immune response to influenza vaccination.47 64 66 The same holds true for the use of TNFα-blocking agents in the majority of studies,11 13 20 41 80 including two meta-analyses in RA.75 77 Another meta-analysis reported a lower seroprotection, but not seroconversion rate in patients with RA on anti-TNF α, only for the H1N1 influenza strain.42 Four studies did report a modestly reduced response to influenza vaccination in patients using anti-TNFα.10 16 40 60
B cell depleting therapy has been associated with hampered antibody responses following influenza vaccination in multiple studies. A negative influence of B cell depleting therapy was observed in two meta-analyses that pooled data from cohort studies. Patient numbers in analyses were low however, and CIs were wide.42 77 The interval between administration of rituximab and vaccination differed between studies. A study that included both patients with RA vaccinated 4–8 weeks (n=11) and 6–10 months after (n=12) the administration of rituximab demonstrated no response to influenza vaccination in the first, early group and a modestly restored response in the late group.14 The use of rituximab did not seem to affect cell-mediated immune responses to influenza vaccination in a study with a limited number of patients.38
Two studies demonstrated that patients with RA treated with tocilizumab, an IL-6 receptor blocking agent, were able to mount a satisfactory antibody response following influenza vaccination.73 81
Controversial data have been published on the effect of abatacept on influenza vaccine immunogenicity. Most of the studies were small in patient numbers, but they reported a substantial negative effect.59 62 82 One relatively large but uncontrolled study, including 184 patients with RA, reported an adequate humoral response to influenza vaccination.83
Only one study investigated the influence of tofacitinib on influenza vaccine immunogenicity in AIIRD. Tocafitinib alone did not seem to affect the immune response to the vaccine, but a combination of tofacitinib and methotrexate was associated with a lower response.84
The effect of glucocorticoids on the immune response to influenza vaccine has mainly been studied in combination with other immunosuppressive agents. The antibody response is generally adequate in patients who were on glucocorticoids at the time of influenza vaccination,21–23 42 47 although some studies did find a mildly reduced response.17 43 44 64 69
Summary and clinical implications
Seasonal trivalent influenza vaccination is associated with a reduced incidence of bacterial complications, hospital admissions and mortality in patients with RA and SLE. It has also been proven to be immunogenic in the majority of studies in patients with AIIRD, even when treated with immunosuppressive agents, with the exclusion of B cell depletion. Although studies that are sufficiently powered with regard to safety are lacking, in the majority of studies disease activity remained stable and only mild adverse events were reported, comparable with HCs. Therefore, the updated EULAR recommendation on influenza states that influenza vaccination should be strongly considered for the majority of patients with AIIRD.3
Pneumococcal vaccination
Efficacy—immunogenicity—safety
To date, 91 pneumococcal serotypes have been identified, 30 of them being responsible for up to 90% of all infections.85 Although the pneumococcal polysaccharide vaccine that includes 23 serotypes (PPSV23) was found to prevent invasive pneumococcal infections in the general population, it did not generate immunity in children younger than 2 years of age and had a limited efficacy in reducing non-bacteraemic pneumonia.86 Therefore, in 2000 a pneumococcal conjugate vaccine comprising seven antigens (PCV7) was developed and expanded to 13 serotypes (PCV13) which was licensed in 2010 based on immunogenicity outcome studies.87 88 In 2015, a randomised controlled study performed in the older healthy population demonstrated the capacity of PCV13 to prevent vaccine-type pneumococcal, bacteraemic and non-bacteraemic community-acquired pneumonia as well as vaccine-type invasive disease.89
Up to the previous recommendations, 15 studies addressed the issue of immunogenicity and safety of PCV13 and PPSV23 in patients with AIIRD: 7 studies in RA,8 90–95 8 in SLE,95–102 2 in patients with spondyloarthropathy (SpA)91 103 and 1 in pSS.104 Adequate as well as reduced immunogenic responses compared with controls were reported in these studies. Treatment with rituximab, TNFα blockers and MTX seemed to impair the humoral response to the pneumococcal vaccine.16 90 92 93
From the previous recommendations and up to August 2018, 34 studies53 76 81 83 84 105–133 and two meta-analyses45 77 have been published on the efficacy, immunogenicity and safety of PPSV23 and the conjugated vaccines PCV7 and PCV13, including evaluation of a combined strategy (tables 7 and 8).106 128 133
Efficacy, immunogenicity and safety of 23-valent pneumococcal polysaccharide vaccine (PPSV23) in patients with AIIRD (October 2009–August 2018)
Immunogenicity and safety of 7-valent and 13-valent pneumococcal conjugate vaccine (PCV7 and PCV13), including prime boosting with 23-valent pneumococcal polysaccharide vaccine (PPSV23), in patients with AIIRD (October 2009–August 2018)
Regarding efficacy of pneumococcal vaccination in AIIRD, a randomised double-blind trial on the clinical efficacy of PPSV23 in preventing pneumonia in patients with RA did not demonstrate an increased efficacy of the vaccine over placebo, emphasising the need for a more efficacious vaccine.120 In contrast, a retrospective study on the long-term effect of PPSV23 in 180 patients with RA treated with MTX showed a relative risk of 9.7 to develop pneumonia among non-vaccinated patients.121 Vaccination with PCV7 tended to reduce the risk of pneumococcal infections in patients with RA and SpA.122 In this cohort, a direct correlation was shown between the postvaccination levels of antipneumococcal antibodies and the risk of pneumococcal infections: more robust antibody responses after vaccination with PCV7 were associated with lower risk of serious pneumococcal infections.123 The humoral immunogenicity and safety of PPSV23 were demonstrated in RA,76 81 109 112 113 119 124 SLE,116 125 134 and, to a limited extent, in SpA and other rheumatic diseases.115 The long-term immunogenicity of PPSV23 was evaluated in two studies in patients with RA, treated with MTX121 and biologics.130 Both have shown a long-term duration of protective antibodies, up to 7 years.
Humoral immunogenicity of PCV7 is similar to that of PPSV23,111 but was shown to decrease after 1.5 years.127 A randomised controlled study in patients with SLE aiming at evaluating the immunogenicity of the combination of PCV7 and PPSV23 in comparison with PPSV23, showed an adequate and similar response in the two groups.128 The immunogenicity of PCV7 is preserved in patients with ANCA-associated vasculitis on remission.105
The immunogenicity of PCV13 has been evaluated in small groups of patients with RA,118 129 SLE114 and pSS.131 It induced an adequate humoral response.
Three studies evaluated the prime-boost strategy. In SLE, the combination of PCV7 and PPSV23 was not more immunogenic than PPSV23 alone.128 Another randomised controlled study evaluated the serological response to PCV13 followed by PPSV23 after 16–24 weeks in patients with RA, with one of the arms including two doses of PCV13. This study demonstrated an adequate response in patients with RA (87% and 94% on biological disease-modifying antirheumatic drugs (DMARDs) and conventional synthetic DMARDs, respectively), without additional effect of two PCV13 injections.106 An additional study has questioned the long-term effect of the prime boosting strategy using PCV13 and PPSV23, showing reduced levels of functional antibodies 2 years after vaccination.133
No safety issues following pneumococcal vaccination in most of the AIIRDs were reported, independent of vaccine type (see tables 7 and 8). In contrast, data from the b-CONFIDENT Study in patients with cryopyrin associated periodic syndrome (CAPS) and from a case series of seven patients with CAPS showed that PPSV23 might induce severe local reactions and systemic reactions in these patients (fever, headache, meningismus, nausea), necessitating hospitalisation.126 All symptoms resolved within a period of 3–17 days.
Influence of immunomodulating agents
Humoral immunogenicity of PPSV23 has been shown to be reduced by MTX,119 abatacept,109 golimumab,124 tofacitinib84 and rituximab,90 but not to be affected by certolizumab76 and belimumab.125 Immunogenicity following PCV7 vaccination is reduced by the use of MTX,110 abatacept and rituximab,108 but not by TNFα blockers.110 Additionally, the humoral response of PCV13 is reduced under MTX.118 A randomised controlled study in patients with RA that evaluated the serological response to PCV13 followed by PPSV23 after 16–24 weeks, showed a significantly decreased response in patients treated with rituximab. The prime-boost strategy with PCV13 did not improve the response106 (see table 6 for summary).
Summary and clinical implications
Stepwise pneumococcal vaccination, according to the prime-boost strategy (PCV13 followed by PPSV23, with an interval of at least 8 weeks between the two vaccinations) is currently recommended by the Centers for Disease Control and Prevention (CDC) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) for young children, adults above 65 years of age and patients at risk for pneumococcal disease.135 This is mainly based on expert opinion, although studies conducted in the general population136 137 and in patients with HIV138 did show an augmented immunogenic response following combined vaccination.
Pneumococcal vaccination should be strongly considered for the majority of patients with AIIRD for the following considerations: (1) The increased risk of non-invasive and invasive pneumococcal disease in patients with AIIRD.1 (2) Good efficacy, immunogenicity and a favourable safety profile of pneumococcal vaccines (with the exception of patients with CAPS). (3) In line with the present recommendations of the CDC87 139 and the ESCMID.135 Given the insufficient evidence for the efficacy of the combination of PCV13 and PPSC23, the choice and sequence of pneumococcal vaccination should be in concordance with local guidelines.
Hepatitis A vaccination
Efficacy—immunogenicity—safety
Hepatitis A virus (HAV) vaccine, an inactivated vaccine, is very efficacious in preventing hepatitis A.140 141 There are however no studies on the efficacy of HAV vaccination in patients with AIIRD. All three studies on immunogenicity HAV vaccination in patients with AIIRD have been published after the 2011 version EULAR recommendations2 and SLR142 (table 9).
Efficacy, immunogenicity and safety of hepatitis A vaccination in patients with AIIRD
In healthy persons, the HAV vaccine is highly immunogenic, resulting in seroprotection in ≥95% only 1 month after the first vaccine dose.143 144 In patients with RA, it has been shown to be less immunogenic. The percentage of seroprotected patients with RA after 1 month varied between 10%145 and 60%–68%146 in two studies that used different methods. A three-dose schedule (0, 1 and 6 months or 0 (double dose) and 6 months) resulted in 99% seroconversion in patients with RA after 12 months.146 A double dose of vaccine at baseline did not result in an improved seroconversion rate after 1 month, compared with the usual dose (68% vs 60%).146
In terms of safety, there are no data on the influence of vaccination on activity of the underlying AIIRD. Adverse events were generally mild, and reported in up to 17% of patients.145 146 Askling et al reported one case of meningoencephalitis which occurred in a patient with an RA 2.5 weeks after the second dose of HAV vaccine.145
Influence of immunomodulating agents
Using a cut-off for seroprotection of anti-HAV ≥10 mIU/mL instead of 20 mIU/ml, significantly more patients with RA using only an anti-TNFα agent (73%, n=15) reached seroprotection than those using a combination of anti-TNF and MTX (15%, n=21) or MTX alone (6%, n=17).145 In a study of 173 immunosuppressive-treated patients (31 anti-TNF, 123 classic DMARD and 19 other), the use of anti-TNF was associated with lower seroprotection rates in a multivariate logistic regression analysis (see table 9).147
Summary and clinical implications
Since a single dose of HAV vaccine does not seem to afford sufficient protection in a substantial percentage of patients with AIIRD, it is recommended to administer a second dose of vaccine 6 months after the first and to determine postvaccination antibody titres. If this is not possible, as in the case of a last-minute traveller, it should be borne in mind that a patient with AIIRD may not be protected after a single dose of HAV vaccine. Passive immunisation for the specific journey may be considered.
Hepatitis B vaccination
Efficacy—immunogenicity—safety
The incidence of hepatitis B virus (HBV) infections has markedly decreased in countries where HBV vaccination is routinely implemented.148 Although no antibody level gives complete protection against transient infection, there is a clear association between antibody level and risk of HBV infection.149 In general, a level of antihepatitis B surface antigen ≥10 mIU/ml is considered protective.
Up to the previous version of recommendations, a total of four studies reported on the immunogenicity of HBV vaccination in patients with RA,150 SLE,151 AS152 and Behçet’s disease.153 One additional study in patients with RA had been published since then (online supplementary table S1).154
Supplemental material
This recent study, including 46 patients with RA and 9 HCs, reported a significantly lower percentage of patients versus HCs reaching seroprotective antibody levels (64% in patients vs 100% in HCs).154 Another controlled study from 2005, with 13 patients with Behçet’s disease and 15 HCs reported no difference in immunogenicity of the HBV vaccine.153 A response to the vaccine was demonstrated in all remaining studies on HBV vaccination in patients with AIIRD that did not include a control group150–152 (online supplementary table S1).
The HBV vaccine did not lead to changes in overall disease activity in patients with RA and Behçet’s disease.150 153 154
Influence of immunomodulating agents
A severely hampered antibody response to HBV vaccination was noted in patients with AS treated with TNF-blocking agents.152
Summary and clinical implications
HBV vaccine should be administered to patients with AIIRD at risk of infection, for example, medical personnel, patients having an infected family member, intravenous drug users, men who have sex with men, and patients travelling to or residents from endemic countries. It is advised to determine vaccination response. For non-responders several strategies are available to try to reach seroprotection. A booster vaccination or passive immunisation should be considered for an unvaccinated patient or a patient with insufficient response exposed to HBV. See recommendations of the CDC via https://www.cdc.gov/vaccines/pubs/pinkbook/downloads/hepb.pdf.
Tetanus toxoid vaccination
Efficacy—immunogenicity—safety
The efficacy of tetanus toxoid vaccination in the prevention of tetanus has never been studied in a vaccine trial. The incidence of tetanus has been shown to decrease dramatically in vaccinated populations,155 156 although this was not specified for the AIIRD population. The protective antibody level for tetanus is generally considered to be ≥0.1 IU/mL. Tetanus is extremely rare in fully immunised adults who received their last dose of vaccine within the preceding 10 years.
Reports on immunogenicity of tetanus toxoid vaccination in patients with RA showed satisfactory antibody responses.9 112 157 Most studies in patients with SLE reported adequate response rates.102 157–159 One small study from 1980 including nine patients with SLE and nine HCs showed a diminished response in the patients with SLE, with a blunted response in three of them.160
Most studies did not report on safety of tetanus toxoid vaccination. One randomised controlled trial (RCT) showed a higher incidence of mild/moderate adverse events after combined tetanus toxoid and pneumococcal vaccination in patients with RA on MTX who recently started the use of tocilizumab, compared with patients with RA on MTX only (online supplementary table S2).112
Influence of immunomodulating agents
Rituximab administered 24 weeks before vaccination did not affect response to the tetanus toxoid vaccine in patients with RA.90 An RCT in 54 patients with RA on MTX who started tociluzimab 3 weeks before tetanus toxoid vaccination, and 27 RA MTX disease controls, showed no difference in immunogenicity of the tetanus toxoid vaccine between groups. However, there were only three patients in the tocilizumab + MTX group who did not have a seroprotective antibody level at baseline. Two out of these three patients reached a protective level 5 weeks after vaccination.112
An observational study on immunogenicity of pneumococcal, tetanus toxoid and H. influenzae type B vaccine in 73 patients with SLE reported a trend towards a lower response in patients on glucocorticoids and azathioprine, which was not specified for tetanus toxoid vaccination.102
Summary and clinical implications
As satisfactory immune responses were observed in patients with AIIRD following tetanus toxoid vaccination, mostly similar to the response in HCs, and no serious adverse events have been reported, the updated EULAR recommendations conclude that patients with AIIRD should receive tetanus toxoid vaccination according to national recommendations for the general population. Since no data are available on efficacy or immunogenicity of tetanus toxoid vaccination in patients who received B cell depleting therapy within the preceding 6 months, passive immunisation with tetanus immunoglobulins should be considered in these patients in case of an event with high risk of acquiring tetanus, when the vaccine would otherwise be indicated, according to expert opinion.
Herpes zoster vaccination
Efficacy—immunogenicity—safety
Up to the previous recommendations, no data were available on herpes zoster vaccination in patients with AIIRD. Since 2010 seven relevant studies have been published (table 10).
Efficacy, immunogenicity and safety of live-attenuated herpes zoster vaccination in patients with AIIRD
Currently, two different vaccines are available for the prevention of herpes zoster in varicella-zoster virus (VZV)-seropositive healthy adults above the age of 50 years: one is a live-attenuated vaccine and the other is an adjuvanted subunit (non-live) vaccine. All studies on zoster vaccination in patients with AIIRD have been performed using the live-attenuated zoster vaccine. This vaccine has been shown to decrease the risk of herpes zoster in adults above the age of 50 years by 38%–70%,161 162 with lowest efficacy in those above 70 years.161 Of note, the AS01 adjuvanted subunit (non-live) vaccine has recently been shown to be safe and more efficacious than the live-attenuated vaccine in healthy adults above the age of 50 and 70 years.161 163 164 Vaccine efficacy ranged between 91% and 98% and did not significantly differ between age groups.163 164 Of note, safety of the adjuvant system AS01, which contributes to the generation of a particularly strong cellular immune response,165 166 has not yet been determined in patients with AIIRD.
Vaccination with the live-attenuated zoster vaccine was associated with a reduced incidence of herpes zoster in patients with immune-mediated diseases (RA, psoriatic arthritis, ankylosing spondylitis, psoriasis and inflammatory bowel diseases) over 60 years of age, as reported in a large retrospective database study by Zhang et al. In total, 7780 vaccinated and over 800 000 unvaccinated patients were included in their analysis.167 A rapid decline in vaccine efficacy was observed in the same study population. Six years after vaccination, the difference in herpes zoster incidence between groups of vaccinated and unvaccinated subjects was no longer significant.168
Immunogenicity of the live-attenuated zoster vaccine has been investigated in patients with RA169 170 and SLE.171 Both patient groups were able to mount cell-mediated immune responses to the vaccine,169–171 which is crucial for the protection against herpes zoster.172 However, live-attenuated zoster vaccination resulted in lower cell-mediated immunity in patients with RA (n=41) than in controls (n=28).169 Because no correlate of protection for herpes zoster infection is known, and methods for assessing herpes zoster immunity are not uniform, interpretation and comparison of studies is difficult.
Disease activity of the underlying AIIRD did not seem to be affected by live zoster vaccination, but numbers of analysed patients are low.169–171 In a study in patients with RA, who were randomised to receive tofacitinib (n=55) or placebo (n=57) 2–3 weeks following vaccination, three serious adverse events were observed in the tofacitinib group versus none in the placebo group. Of note, one case of disseminated primary varicella occurred in a patient who was VZV-seronegative at baseline.170 In the retrospective database study by Zhang et al, the zoster vaccine did not seem to induce infection within 42 days after vaccination. On the contrary: a reduced incidence of herpes zoster was seen in the vaccinated patients. No cases of hospitalised meningitis or encephalitis were identified in this period.167
Influence of immunomodulating agents
The favourable effect of vaccination on herpes zoster incidence in patients with autoimmune diseases is present regardless of medication use, including biologics (used by 633 vaccinated patients), as reported in the same large database study by Zhang et al.167 A daily dose of 5–20 mg of corticosteroids in a heterogeneous patient group (206 patients received zoster vaccination, of whom 25% were patients with polymyalgia rheumatica) did not seem to affect humoral immune response to live-attenuated zoster vaccination. Unfortunately, effect on cell-mediated immune response was not reported.173 Zoster vaccination resulted in a similar cell-mediated response in patients with RA who started the use of tofacitinib or placebo 2–3 weeks after vaccination (see table 10).170
Summary and clinical implications
Although large prospective trials that are sufficiently powered for assessing safety are lacking, the safety and efficacy profile of the live-attenuated zoster vaccine seem to be favourable for VZV-seropositive patients with AIIRD. However, the vaccine contains live-attenuated virus and, therefore, should still be considered with caution in the immunocompromised patient. Before administering the zoster vaccine, it is advisable to affirm the VZV-seropositive status of the patient. In case of a VZV-seronegative patient, a less potent VZV vaccine approved for preventing primary varicella in children may be considered. Based on expert opinion, the zoster vaccine is preferably administered 4 weeks prior to initiation and not during treatment with biologics and targeted synthetic DMARDs .
As noted earlier, the novel non-live AS01 adjuvanted subunit vaccine has been shown to be more efficacious than the live-attenuated vaccine in healthy adults above the age of 50–70 years. Whether this also holds true for the AIIRD population and whether the adjuvant system AS01 is safe in this patient group, is most interesting and warrants further investigation.
Yellow fever vaccination
Efficacy—immunogenicity—safety
The yellow fever vaccine is a live-attenuated vaccine. Several cases of visceral dissemination of yellow fever of the vaccine type have been reported, with clinical features similar to wild type yellow fever, including high mortality.174–176 The vaccine is therefore generally contraindicated in immunocompromised patients177–180 (online supplementary table S3).
Only limited observational studies have been published on yellow fever vaccination in patients with AIIRD, mostly concerning revaccination (see online supplementary table S3 for details). The reported immunogenicity results are mainly adequate, and similar as in HC.177–180
A study of 34 glucocorticoid-treated patients (among whom 9 were patients with RA and 14 with chronic inflammatory conditions, revaccination in 44%) and 68 HC, reported more moderate and severe local reactions in patients (12% vs 2%).179 No serious systemic adverse events of yellow fever vaccination were reported in the previously mentioned studies in patients with AIIRD. As the vaccine has been contraindicated in immunocompromised patients for years, numbers of studies and included patients are however very low and, as stated, most patients were revaccinated. Of note, lethal outcomes of fellow fever vaccination have been reported in immunocompromised patients, including a female patient with RA and SLE, who was possibly treated with glucocorticoids and MTX.181
Influence of immunomodulating agents
Due to the heterogeneous populations of the small studies on yellow fever vaccination in patients with AIIRD, it is difficult to discern the separate influences of different immunosuppressive agents. In a study of corticosteroid-treated patients, of whom 44% were vaccinated for yellow fever earlier in life, seroprotection against yellow fever was reached in all 20 analysed patients. A trend towards a lower yellow fever antibody response was observed in anti-TNFα-treated patients with RA (n=17) compared with HC (n=15).180
Summary and clinical implications
Reported immunogenicity results of yellow fever revaccination among patients with AIIRD are mainly adequate and similar as in HC. However, the available data on the safety of yellow fever vaccination in this group are very limited, and potential sequelae are serious (including death). Patients with AIIRD under immunosuppression should, therefore, avoid yellow fever vaccination in general. Temporarily withholding immunosuppressive therapy may be considered for patients with AIIRD travelling to endemic countries.
Human papillomavirus vaccination
Efficacy—immunogenicity—safety
Data on the efficacy of human papillomavirus (HPV) vaccination originate from vaccine trials in HCs that investigate the capacity of HPV vaccination to prevent premalignant lesions. A vaccine efficacy of 66% to prevent cervical intraepithelial neoplasia grade III was reported in a bivalent (HPV types 16 and 18) HPV vaccine trial after 4.5–10 years of follow-up.182
The correlation between the level of anti-HPV antibodies and protection against the development of cervical carcinoma is not known, since there are no reports on cervical carcinoma in vaccinated subjects. The level of seroprotection is based on comparison with naturally infected subjects.183
To date, no studies on the efficacy of HPV vaccination to prevent malignancies or premalignant lesions in the AIIRD population have been published, but there are studies on HPV vaccine immunogenicity in patients with AIIRD, all published after 2010 (online supplementary table S4). All but one study, performed in patients with juvenile idiopathic arthritis (JIA),184 include patients with SLE and used a quadrivalent (HPV types 6, 11, 16 and 18) vaccine.185–189 Seroconversion rates in patients were high and usually similar to those of healthy subjects, although two studies reported a lower geometrical mean titre for HPV 16 in patients with SLE after 5 years of follow-up,185 and also for patients with JIA,184 compared with HCs.
Rates of vaccine adverse events similar to HCs were reported for both patients with SLE188 and patients with JIA.184 Disease activity after vaccination was stable.184 186 188 189
Influence of immunomodulating agents
Mok et al reported that anti-HPV titres were lower in vaccinated patients with SLE using immunsosuppressive agents, especially in those receiving a combination of mycophenolate mofetil (MMF) and glucocorticoids.188 After 5 years of follow-up it was noted that patients with SLE that no longer were anti-HPV seropositive received significantly longer and higher doses of glucocorticoids and MMF than those with persistent seropositivity.185
Summary and clinical implications
Immunogenicity of HPV vaccination in the AIIRD population is high and, in the majority of studies, similar to that in HCs. The vaccine appears to be safe in patients with AIIRD. Therefore, the vaccine is recommended for patients with AIIRD, in accordance with recommendations for the general population. Patients with SLE, in particular, are advised to receive HPV vaccination, since they were shown to be at high risk of contracting a genital HPV infection, including the serotypes that are considered to be high risk for developing cervical dysplasia.190–194
Tickborne encephalitis vaccination
Efficacy—immunogenicity—safety
The available tickborne encephalitis (TBE) vaccines are inactivated vaccines. The vaccine is highly immunogenic in the general adult population.195 Excellent effectiveness of TBE vaccination in prevention of TBE was demonstrated in an Austrian study.196 Nonetheless, cases of vaccine failure have been reported, which occurred mainly in older or immunocompromised persons197 .
To date, only one study on vaccination against TBE in patients with AIIRD has been published (online supplementary table S5). This Swedish study by Hertzell et al enrolled 65 patients with RA and 1 patient with AS on anti-TNF (n=16), a combination of MTX and anti-TNF (n=36) or MTX alone (n=14). Four doses of vaccine instead of three were offered to patients and HCs ≥60 years of age. One month after the last dose of vaccine, 39% of the patients and 79% of the HCs had developed protective levels of neutralising TBE antibodies. The difference was statistically significant. An extra dose of vaccine in patients with an undetectable antibody level at month 13 resulted in seroprotection in 4 out of 10 patients, all of whom were older than 60 years. No serious adverse events occurred.198
Influence of immunomodulating agents
In the study by Hertzell et al, regarding only patients ≥60 years of age, it seemed that a lower percentage of those treated with a combination of MTX and anti-TNF reached seroprotective anti-TBE levels than those treated with MTX or anti-TNF alone (25% vs 38%–40%).198
Summary and clinical implications
Although the updated recommendations do not specifically provide recommendations regarding TBE vaccination, an overarching principle states that non-live vaccines can be administered to patients with AIIRD, including during their use of glucocorticoids and DMARDs. The only available study on TBE vaccination in the AIIRD patient population showed a diminished immunogenicity response in these patients. As such, determining TBE-antibody levels after the last vaccine dose and, if necessary, giving an extra dose of vaccine may be considered.
Discussion
This SLR summarises the available data on efficacy, immunogenicity and safety of vaccination in patients with AIIRD, including patients with AIIRD using immunomodulating agents. Since the first version of EULAR recommendations and accompanying SLR on vaccination of adult patients with AIIRD were published in 2011,2 142 there has been a large expansion in the amount of available evidence on this topic, necessitating an update. By defining four research questions, we were able to address incidence/prevalence of VPIs, efficacy, immunogenicity and safety of vaccination, as well as the influence of immunomodulating agents on vaccine efficacy/immunogenicity in patients with AIIRD. To enable the presentation of a clear overview of the large amount of available data, the evidence on the incidence and prevalence of VPI diseases in patients with AIIRD was presented in a separate SLR, which was submitted for publication simultaneously with this report. The literature search for the fourth research question, dealing with the effect of vaccinating household members of patients with AIIRD on the occurrence of VPI in these patients and household members (including newborns), did not result in finding any relevant studies. Therefore, the recommendation encouraging household members of patients with AIIRD to receive vaccines according to national guidelines with the exception of oral polio vaccine, as formulated in the updated recommendations, is based on expert opinion. This recommendation follows guidelines of international societies such as the Infectious Diseases Society of America.199 Also the recommendation of avoiding live-attenuated vaccines during the first 6 months of life in newborns of mothers treated with biologics during the second half of pregnancy is based on expert opinion. This recommendation is in line with the EULAR points to consider for use of antirheumatic drugs before pregnancy, and during pregnancy and lactation.200
One strength of our current approach, compared with the 2011 SLR, is the clear separation between efficacy and immunogenicity of vaccination, allowing a just interpretation of the data by readers. When assessing the different vaccines, evidence on efficacy, defined as the capacity of a vaccine to prevent infection, was considered to be of higher quality than evidence on immunogenicity, which refers to the capacity of vaccines to induce humoral and/or cellular immune responses. Unfortunately, because of the necessarily large sample size, using a clinical end point was essentially infeasible for some groups of AIIRD and/or vaccines. Consequently, only a small number of studies used a clinical end point.
It is important to note that although a large number of articles was included, for certain AIIRDs, vaccines and immunomodulating treatments the number of publications was still very limited. The majority of studies was performed in patients with RA and SLE. Results in these patient groups cannot uncontestedly be extrapolated one on one to patients with other AIIRDs.
Regarding safety of vaccination in the AIIRD population, both the occurrence of adverse events and influence on underlying disease of vaccination were assessed. Although since 2011 the amount of available evidence has considerably grown, studying safety of vaccination in patients with AIIRD remains a challenge. While vaccination did not lead to significant harms in the large majority of the included studies, these studies were too small or not properly designed to be able to detect the occurrence of rare adverse events.
In conclusion, evidence on efficacy, immunogenicity and safety of vaccination in patients with AIIRD (including those using immunomodulation agents), from October 2009 to August 2018, was systematically reviewed to provide a basis for updated evidence-based recommendations for vaccination in patients with AIIRD,3 in order to aid physicians, nurses and other health professionals dealing with questions regarding vaccination in patients with AIIRD in daily clinical practice.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.↵
- 170.↵
- 171.↵
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.↵
- 183.↵
- 184.↵
- 185.↵
- 186.↵
- 187.↵
- 188.↵
- 189.↵
- 190.↵
- 191.↵
- 192.↵
- 193.↵
- 194.↵
- 195.↵
- 196.↵
- 197.↵
- 198.↵
- 199.↵
- 200.↵
- 201.
- 202.
- 203.
- 204.
- 205.
- 206.
- 207.
- 208.
Footnotes
CR and VF contributed equally.
Contributors CR, in collaboration with SvA, reviewed articles on efficacy, immunogenicity and safety of vaccination for influenza, hepatitis A, hepatitis B, tetanus toxoid, herpes zoster, yellow fever and tickborne encephalitis in patients with AIIRD, and drafted the first version of the manuscript. VF, in collaboration with OE, performed the literature search and reviewed articles on vaccination in patients with AIIRD on the various immunomodulating therapies. MH reviewed articles on efficacy, immunogenicity and safety of vaccination of human papillomavirus vaccination in patients with AIIRD. OE initiated the project, reviewed articles on efficacy, immunogenicity and safety of vaccination for pneumococcal disease in patients with AIIRD, and wrote the paragraphs on pneumococcal vaccination. All authors collaborated in discussions during two meetings, and read and approved the final manuscript.
Funding This project was supported by EULAR.
Competing interests KW reports personal fees from Pfizer, during the conduct of the study; grants and personal fees from Biotest, CSL Behring, personal fees from LFB, Grifols, Baxter, Roche, Octapharma, grants from BMS, outside the submitted work. AM reports grants and personal fees from ABBVIE, Pfizer, BMS, UCB, MERCK, during the conduct of the study. MD reports grants and personal fees from PFIZER, ABBVIE, UCB, NOVARTIS, LILLY, MERCK, ROCHE, grants from BMS, outside the submitted work. OE reports grants and personal fees from Pfizer, Abbvie, Roche, Janssen, personal fees from Novartis and Lilly. All other authors have no conflicts of interests to declare.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.