Article Text

Abstract
Idiopathic inflammatory myopathies (IIM) include the main subgroups polymyositis (PM), dermatomyositis (DM), inclusion body myositis (IBM) and juvenile DM (JDM). The mentioned subgroups are characterised by inflammation of skeletal muscles leading to muscle weakness and other organs can also be affected as well. Even though clinically significant heart involvement is uncommon, heart disease is one of the major causes of death in IIM. Recent studies show an increased prevalence of traditional cardiovascular risk factors in JDM and DM/PM, which need attention. The risk of developing atherosclerotic coronary artery disease is increased twofold to fourfold in DM/PM. New and improved diagnostic methods have in recent studies in PM/DM and JDM demonstrated a high prevalence of subclinical cardiac involvement, especially diastolic dysfunction. Interactions between proinflammatory cytokines and traditional risk factors might contribute to the pathogenesis of cardiac dysfunction. Heart involvement could also be related to myocarditis and/or myocardial fibrosis, leading to arrhythmias and congestive heart failure, demonstrated both in adult and juvenile IIM. Also, reduced heart rate variability (a known risk factor for cardiac morbidity and mortality) has been shown in long-standing JDM. Until more information is available, patients with IIM should follow the same recommendations for cardiovascular risk stratification and prevention as for the corresponding general population, but be aware that statins might worsen muscle symptoms mimicking myositis relapse. On the basis of recent studies, we recommend a low threshold for cardiac workup and follow-up in patients with IIM.
- Atherosclerosis
- Cardiovascular Disease
- Dermatomyositis
- Treatment
- Polymyositis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Idiopathic inflammatory myopathies (IIMs) are associated with increased risk of cardiac involvement mainly due to atherosclerosis and myocarditis.
A low threshold for cardiac workup and follow-up in IIM is recommended.
Monitor carefully when using statins in IIM: statins may worsen muscle symptoms mimicking myositis relapse.
Introduction
Idiopathic inflammatory myopathies (IIMs) are a heterogeneous group of diseases characterised by proximal muscle weakness and inflammatory changes in skeletal muscle. Adults or children can be affected, and in adult onset IIM, cardiovascular complications represent a major cause of death. However, there is limited information on heart involvement in IIM, both due to the rarity of the diseases and because manifest cardiac complications in these patients are uncommon. In other rheumatic diseases, like rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE), cardiac involvement is well documented.1–3 More recently, registry-based studies reported associations between atherosclerosis and rare rheumatic and autoimmune diseases, including IIM.4 ,5 Whether atherosclerosis is the driving force of the cardiac involvement in IIM or mechanisms such as myocardial inflammation, systemic inflammation or small vessel vasculitis play equally important roles remains unknown.
Historically, cardiac involvement in IIM has been demonstrated by ECG,6–8 continuous electrocardiographic monitoring9–11 and autopsies.12 ,13 Today, new cardiac imaging modalities such as Tissue Doppler imaging (TDI) by echocardiography,14–18 Cardiac MR (CMR),19 99mtechnetium pyrophosphate (99mTc-PYP) scintigraphy18 ,20 ,21 and coronary artery calcification on CT scan22 can detect subtle cardiac abnormalities. Owing to their high sensitivity, these methods often suggest a higher frequency of heart disease in IIM than what is clinically evident. However, despite this discrepancy, subclinical cardiac pathology might represent early stages in cardiac remodelling that will later manifest as clinical heart disease, and can therefore not be ignored. Further research is needed to clarify if subclinical disease will eventually develop into clinically manifest cardiac disease.23
Beyond general guidelines for cardiac diseases, specific recommendations for treatment or cardiac follow-up of patients with IIM are non-existing. This review summarises current evidence of cardiac complications in patients with the IIM subgroups polymyositis (PM), dermatomyositis (DM), inclusion body myositis (IBM) and juvenile IIM, where juvenile dermatomyositis (JDM) is by far the most common subgroup. We will also discuss possible disease mechanisms and what make these patients particularly vulnerable, beyond the traditional cardiovascular (CV) risk factors.
Cardiac mortality
The three major causes of cardiac mortality in patients with IIM24 are similar to those of the population in general: congestive heart failure, myocardial infarction and arrhythmias. The reported mortality due to cardiac involvement in adult onset IIM varies substantially in the literature.25–30 Eleven by 20 (55%) of the deaths were due to cardiac aetiology in a Hungarian longitudinal study,26 36% of 149 deaths were due to circulatory causes (not further specified) in a register-based Finnish study, whereas 12/87 (14%) deaths were due to cardiac causes in a recent population-based Norwegian study.31 Also, in retrospective follow-up studies on patients with PM and DM, cardiac disease was one of the four most frequent causes of death.32 ,33 The discrepancies between the studies regarding aetiology of deaths may be due to variable study designs and populations, variable definitions of cardiac involvement, limited numbers of patients in some of the series and studies performed at different time periods and decades.
Not surprisingly, cardiac disease has been associated with poor prognosis: in one study, 9 of 28 patients (32%) with PM or DM and cardiac involvement died within 8 years, whereas only 4 of the remaining 48 patients (8%) died during the same period.34 In juvenile IIM, a Canadian study reported cardiac involvement in 3/17 reported deaths, but these patients also had involvement of other organ systems.35
Traditional cardiovascular risk factors
Increasing evidence suggests that traditional CV risk factors (including diabetes, hypertension, dyslipidaemia, obesity and smoking) are more prevalent in adult onset IIM than in the general population (table 1); this has especially been found for abdominal obesity.22 ,36 ,37 Increased prevalence of hypertension and dyslipidaemia has also been shown in untreated patients with IIM,38 ,39 which indicates an effect of the disease per se in addition to a possible effect of long-term glucocorticoid treatment. Also in JDM, hypertension and dyslipidaemia have been demonstrated (table 1).40–42 These findings are in line with RA43 and SLE.44
Demographic and traditional cardiovascular risk factors of patients with IIM
The potential influence of and associations between traditional CV risk factors, disease-specific parameters and cardiac disease in IIM have so far only been addressed in one study.22 In this study, traditional CV risk factors and severe coronary artery calcification (CAC) were commonly found in patients with PM/DM. However, severe CAC was not associated with PM/DM per se, but rather with age and smoking in these patients. Thus, clinicians should pay attention to the presence of traditional CV risk factors.
Clinical heart involvement
Cardiac dysfunction and heart failure
Heart failure is a clinical syndrome with characteristic symptoms and physical findings, while ‘cardiac dysfunction’ is a condition of cardiac pathology demonstrated by various cardiac imaging techniques, but without clinical symptoms. Systolic heart failure/dysfunction is due to impaired left ventricular contraction and results in reduced left ventricular ejection fraction (EF). In diastolic heart failure/dysfunction, left ventricular EF is normal, but pathological stiffness of the left ventricle causes a restricted filling pattern. The symptoms of systolic and diastolic heart failure are indistinguishable. Cardiac function is quickly and well assessed by echocardiography. The common definition of systolic dysfunction is left ventricular EF<40%. Diastolic dysfunction, on the other hand, is defined as E/é>14 (E, early diastolic transmitral flow; é early diastolic tissue velocity) and normal EF (>50).45
Presence of severe systolic heart failure in adult onset IIM is well documented in case reports.46–56 However, controlled studies have not demonstrated increased prevalence of systolic or diastolic heart failure in IIM (table 2). On the other hand, controlled studies have shown diastolic dysfunction in adult onset IIM with impaired E/e’, but no evidence of systolic dysfunction (table 2).14 ,15 ,18 ,57
Echocardiographic findings of studies including tissue Doppler imaging
In JDM, diastolic dysfunction was found in 22% of patients after a median of 17 years from disease onset (table 2)16 in addition to impaired systolic function (low long axis strain assessed by echocardiography) compared to age-matched and sex-matched controls (table 2).17
Whether systolic and diastolic heart failure represent the two extremes on a continuum of cardiac damage58 or whether they are two separate entities, is still a matter of debate.59 Interestingly, many of the referred IIM studies showed an independent association between diastolic dysfunction and disease duration,14–16 ,18 ,57 suggesting at least diastolic cardiac involvement to be a long-term complication of IIM, and only follow-up studies can show if these patients develop heart failure. Thus, the findings of diastolic dysfunction in IIM need attention, since cardiac dysfunction may be seen as an asymptomatic state on the road to clinically overt heart failure. However, whereas a number of treatment options exist for systolic heart failure, no therapy has yet proven effective in diastolic heart failure. It is not known if diastolic dysfunction/heart failure can be prevented by early disease control.
Coronary artery disease
The suggested main mechanism of cardiovascular involvement in IIM is atherosclerosis in the coronary arteries (figure 1). In 2014,60 Ungprasert et al conducted a systematic review and meta-analysis of published observational studies addressing risk of coronary artery disease in adult onset IIM. Four studies, all using registry-based databases, were included4 ,61–63 and demonstrated an increased risk of CAD with a pooled risk-ratio of 2.24 (CI 1.02 to 4.92). However, the only case–control study included in Ungprasert's review did not reveal an increased risk of CAD. Recently, a large population-based retrospective study with incident IIM cases from Canada reported an increased risk of myocardial infarction in dermatomyositis and polymyositis (nearly three and fourfold, respectively), after controlling for age, sex and use of corticosteroids and non-steroidal anti-inflammatory drugs.64 The risk for both groups was highest in the first year after diagnosis.
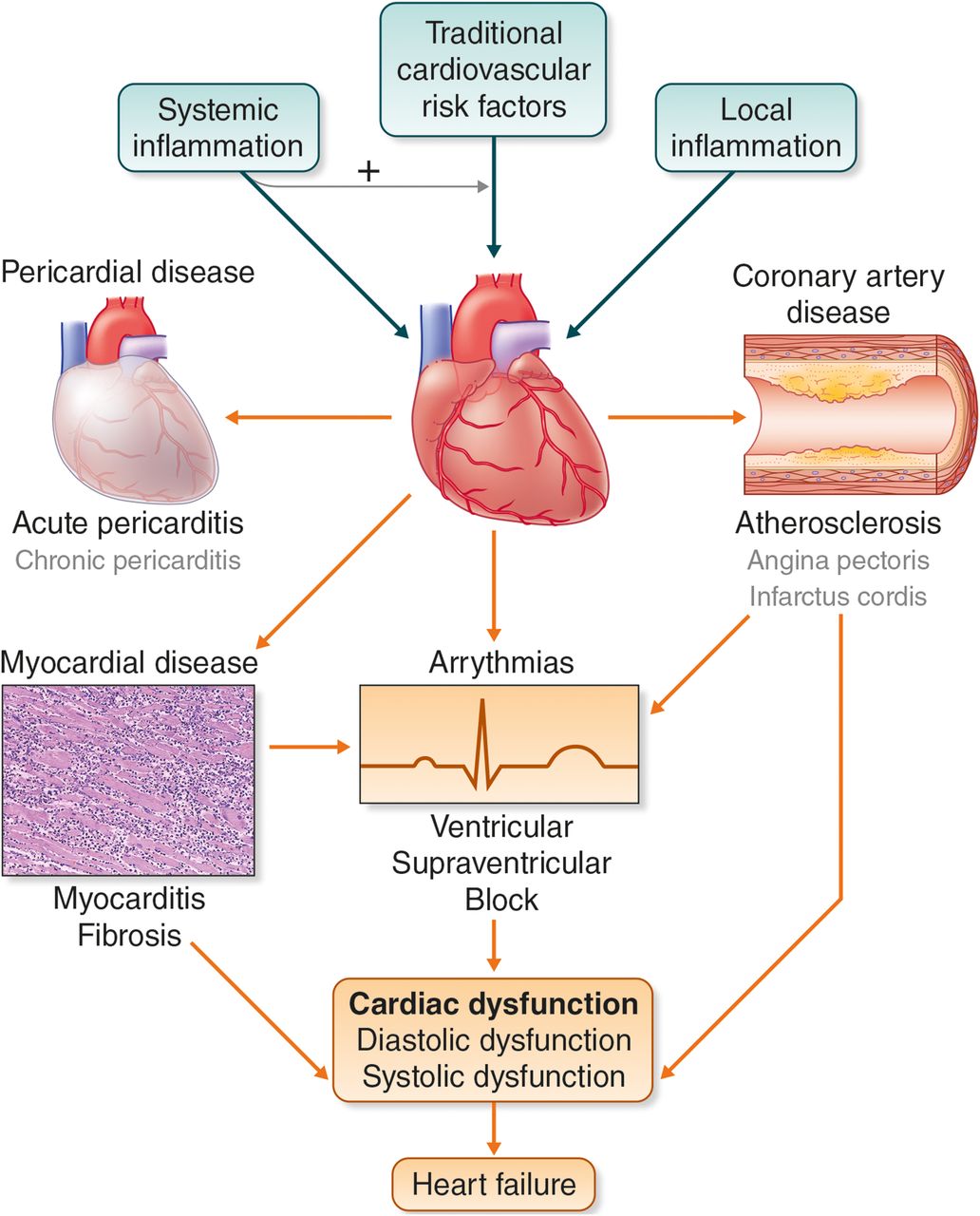
{kind=link}
Traditional cardiovascular risk factors can cause cardiac disease in patients with IIM. Systemic and local inflammation may either have a direct effect on the myocardium or make the heart more susceptible to traditional risk factors. In the heart, disease can occur in the pericardium, coronary arteries or the myocardium, and arrhythmias can appear. Myocardial disease can result in diastolic or systolic dysfunction, and when clinical symptoms arise, the patient has developed heart failure. Myocardial disease may result in arrhythmias, or they can occur as a result of inflammation directly influencing cardiomyocyte function. Both arrhythmias and coronary artery disease, such as myocardial infarction, can directly result in heart failure.
For IBM, few data exist. In a recent Norwegian population-based study with a mean disease duration of 5.5 years, the mortality due to heart failure and myocardial infarction was higher in those with IBM (8/31, 26%) than in those with PM and DM (4/56, 7%). However, the patients with IBM were older (66.9 (0.9) versus 53.2 (1.5) years).31 To the best of our knowledge, no studies address the relationship between JDM and coronary artery disease.
An accelerated process of atherosclerosis is evident in patients with IIM, and seems to be an important aspect in the development of cardiac involvement,22 ,41 ,65 as it is in RA66 and SLE.3 In addition, the higher burden of atherosclerosis appears to be associated with the increased presence of traditional cardiovascular risk factors.22 Taken together, clinicians should be aware of symptoms that can be caused by coronary artery disease in patients with IIM.
Myocarditis
Myocarditis is highlighted as a probable and intriguing mechanism for cardiac dysfunction in IIM, since inflammation similar to that seen in skeletal muscle also can occur in heart muscle (figure 1). Through a comprehensive literature search in 2011, Gupta et al24 found cardiac biopsy data on 68 patients with IIM (including patients with juvenile onset disease) almost exclusively autopsy based. In 1979 and 1982, two series showed myocarditis in 6 of 20 (30%) and 4 of 16 (25%) patients with DM and PM, respectively.12 ,13 Mononuclear cell infiltrates were localised to the endomysium and perivascular areas of the heart muscle, with or without small vessel disease and replacement fibrosis; this resembled the inflammation in skeletal muscle. Infiltrates were also found in the conduction system.13 The remaining of the 68 patients reviewed by Gupta et al were described in three studies and eight case reports.24 Nevertheless, among these unsystematically selected patients, as many as 38% had myocarditis and 41% myocardial fibrosis, suggesting a possible involvement of the heart muscle in patients with IIM.
CMR gives the opportunity of non-invasive investigation of cardiac inflammation. Recent uncontrolled data showed a high proportion (62–75%) of patients with IIM with pathological myocardial enhancement, resembling inflammation and fibrosis.19 ,67 ,68 Also, in a recent case report, MRI mapping techniques detected myocardial oedema.69 99mTechnetium pyrophosphate (99mTc-PYP) scintigraphy is also capable of detecting cardiac muscle involvement, and increased myocardium PYP-uptake, indicative of inflammation, was observed in 57% of patients with PM/DM.20 Two patients with high PYP-uptake and corresponding left ventricular dysfunction died. Autopsy showed inflammation, degeneration and fibrosis of the myocardium in accordance with PYP scintigraphy results. A controlled study has recently established a correlation between the magnitudes of myocardium PYP-uptake and diastolic dysfunction of the heart, which strongly suggests inflammation to be a significant contributor to cardiac involvement in IIM.18 However, these findings were subclinical and further prospective studies are desirable. We suggest considering MRI and/or (99mTc-PYP) scintigraphy as part of the clinical evaluation of patients with IIM if myocarditis is suspected.
Arrhythmia and heart rate variability
Conduction abnormalities on ECG is the most prevalent evidence of cardiac involvement reported in IIM (figure 1). In the late 1970s/1980s, several uncontrolled studies reported ECG changes like non-specific ST-T wave changes, conduction abnormalities or premature ventricular beats in 32–52% of patients with IIM (13–77 patients) without clinical signs of cardiac disease.6–8 ,34 In an autopsy study, as many as 13/18 (72%) had ECG changes assessed retrospectively.12 In a Danish study from 2015, patients with adult PM/DM had longer QTc intervals compared with controls,18 even though the prevalence of pathological QTc was comparable. Pathologically prolonged QTc is a known predictor for cardiac arrhythmias and sudden death. Further studies are needed to clarify the clinical relevance of longer QTc in IIM. A recent Norwegian study demonstrated that patients with JDM examined after a median disease duration of 17 years had more prevalent ECG abnormalities 23/59 (39%) compared to age-matched and sex-matched controls.16
In a subset of the same Norwegian JDM cohort (after a median disease duration of 13.5 years), heart rate variability (HRV) was lower in patients than controls assessed by Holter ECG.70 Low HRV indicates autonomic dysfunction, and is associated with increased risk of cardiac events and death in the general population.71 Autonomic dysfunction by HRV has, to the best of our knowledge, not been investigated in the adult onset IIM population.
Taken together, these findings indicate that even if the detected ECG abnormalities in IIM are often subclinical, the associated cardiac involvement can lead to arrhythmias or sudden death.
Pericarditis
Pericarditis in IIM is mostly asymptomatic and haemodynamically insignificant. It has been found in 4–25% of adult onset patients with IIM8–11 and 12–15% of patients with JDM during the disease course.16 ,72 However, it may be more common in subgroups of patients with antisynthetase syndrome (ASS). In a European multicentre study, 9 of 18 anti-PL-7-positive patients (50%) had pericardial effusion during the disease course.73
Pulmonary hypertension
In IIM, pulmonary hypertension (PH) is probably infrequent in the absence of ILD or antisynthetase autoantibodies, but has not been systematically described and data are mostly limited to case reports or case series.74 The most effective screening method is echocardiography, but PH must be confirmed by right heart catheterisation. PH has been confirmed in 8–9% of patients with ASS in two retrospective series,75 ,76 mostly secondary to ILD. The presence of PH dramatically worsened the prognosis, with a 3-year survival rate of 58%.75 These findings support that routine screening for PH should be performed by echocardiography in patients with ASS at diagnosis and then annually as recommended in patients with systemic sclerosis.77 Screening is important since PH can lead to right ventricular failure, a life-threatening complication.
Methods of cardiac assessments
There are several methods available for assessment of cardiac structure and function.78 The most important methods, their advantages and limitations, as well as an overview of the methods used in IIMs, are shown in table 3. We would like to highlight the opportunities offered by new echocardiographic methods and by CMR, making detection of subclinical cardiac dysfunction possible. Also, cardiac troponin I appears to be specific to the myocardium, while troponin T is also expressed in skeletal muscle. Thus, troponin T can be elevated in IIM in the absence of myocardial involvement.79
Methods of cardiac assessment in IIM
Pathophysiology
Different mechanisms are suspected in the development of cardiac involvement in IIM. Recently, Wang et al found dyslipidaemia in newly diagnosed, untreated patients with PM39 and with DM,38 with lower high-density lipoprotein cholesterol (HDL-c) and higher triglycerides and total-/HDL cholesterol (TC/HDL) ratio than matched controls. High TC/HDL ratio is a predictor of ischaemic heart disease, superior to other lipid parameters such as TC and HDL/low-density lipoprotein (LDL).80 Another controlled study of younger patients with JDM (median age 21.5 years), seen at long-term (17 years) follow-up, had similar findings of dyslipidaemia.16 High TC/HDL ratio and total cholesterol in the upper normal range correlated with subclinical cardiac dysfunction in those with active disease.42 This could indicate a lowered threshold of harmful cholesterol associated effects in active disease. The ‘lipid paradox’ with increased susceptibility to atherosclerosis with low cholesterol levels is even better documented in RA.81 ,82
Autopsy studies of patients with IIM have shown evidence of inflammatory cells in the myocardium,12 ,18 indicating the presence of myocarditis. Myocarditis can lead to myocardial fibrosis, which again causes stiffening of the ventricles (diastolic dysfunction) or arrhythmias (figure 1). In the general population, increased serum levels of proinflammatory cytokines are seen with increasing New York Heart Association-class83 and thus the degree of heart failure. In a cohort of patients with JDM, MCP-1 and CCL11 (eotaxin) were elevated and associated with cardiac dysfunction.42 MCP-1 is known to induce hypertrophy and myocardial fibrosis in rodents83 and CCL11 fibrosis and myocardial stiffness in rats.84
Myositis specific and associated autoantibodies (MSA and MAA) are strong diagnostic tools in IIM, which can define phenotypes, including lung involvement.85 An association between antisignalling recognition particle (anti-SRP) and cardiac disease has been proposed, but evidence is weak in adult IIM.24 However, in juvenile IIM, the presence of anti-SRP was associated with more frequent abnormal ECG and by echocardiography.86 In a recent Danish study, the presence of a MSA or MAA was associated with diastolic dysfunction, although a relationship between specific autoantibodies and diastolic dysfunction was not observed.18
Prevention, diagnostic work-up/follow-up and management
Prevention
Treatment of dyslipidaemia in patients with IIM is complex. Statins can prevent cardiovascular disease in the general population. In rare cases, statins can be the main cause of disease, that is, statin-associated autoimmune necrotising myopathy.87 A recent study performed by the International Myositis Assessment and Clinical Studies Group (IMACS) on the use of lipid-lowering therapy in patients with IIM showed that 76% of the IIM specialists prescribed lipid-lowering drugs, mostly statins (93%).88 Approximately 10% of the patients developed worsening of their muscle symptoms, of which some were reversible on discontinuation of statin treatment. With the literature available, patients with IIM should follow the same recommendations for cardiovascular risk stratification and prevention as for the corresponding general population.89 ,90 Thus, in IIM, statins should be used with careful monitoring as they may worsen muscle symptoms that can be misinterpreted as a relapse of myositis. Also, clinicians should keep in mind the lipid paradox described above.
Diagnostic workup and follow-up
If clinical or subclinical cardiac involvement is suspected based on cardiac symptoms and/or basic cardiac measurements (physical examination, troponin, ECG, etc), a cardiologist should be involved. A low threshold for echocardiographic examination should be observed. To evaluate systolic involvement, we recommend assessing long axis strain (EF is not sensitive enough), and to evaluate diastolic involvement we recommend E/é. If available, we suggest considering MRI and/or (99mTc-PYP) scintigraphy as part of the clinical evaluation of patients with IIM if myocarditis is suspected.
As a follow-up, it seems reasonable to do yearly ECG, since ECG changes are the most prevalent evidence of cardiac involvement reported in IIM. Specifically, attention should be paid to prolongation of the QTc interval, which in turn might call for Holter monitoring to exclude clinically significant ventricular arrhythmia.
Management
Currently, there are no specific guidelines available for treatment of heart involvement in myositis. Although inflammatory changes within the myocardium are thought to be the cause of reported cardiac dysfunction, the impact of immunosuppressive therapy is unknown. However, it is reasonable to assume that an early and sustained reduction in inflammation might reduce the risk of developing diffuse interstitial myocardial fibrosis, which is important since inflammation is treatable, while fibrosis is thought to be irreversible.
In several case reports, successful pharmacological treatment of arrhythmia, conduction disorders and heart failure in children and adults with myositis are reported.11 ,48 ,91 However, it is hard to decide the effect of the immunosuppressive treatment alone, since these patients also received antiarrhythmic drugs and heart failure management depending on their symptoms. Three studies including 20–44 patients with adult onset DM/PM show an effect of glucocorticoids plus other immunosuppressive drugs on clinical or subclinical heart involvement in the majority of patients.11 ,68 ,92
Importantly, heart disease can also occur any time during the disease course under immunosuppressive treatment,93 and even in patients in remission.94
Based on case reports, glucocorticoids, either alone or in combination with other immunosuppressive drugs, are cornerstones in the treatment of myocarditis. In addition to immunosuppressive therapy, management of cardiac involvement may require individually tailored cardiac specific therapy.
Concluding remarks
Similar to other rheumatic diseases, IIM is associated with an increased risk of cardiac disease: however, the prevalence still remains uncertain. The main mechanisms responsible seem to be atherosclerosis and myocarditis. New methods of cardiac imaging with ever increasing sensitivity enable us to detect subtle changes of cardiac function. As physicians, we must use this new insight to give patients with IIM optimal cardiac care and preventive treatment; however, consensus guidelines for this do not yet exist. Also, this new insight challenges us to determine which findings have clinical significance and, perhaps, which have not. Therefore, longitudinal follow-up of patients with IIM with recording of clinical manifestations of heart involvement is needed. Since these are rare diseases, international collaboration is essential. To support such collaboration, the Euromyositis Register has been developed to facilitate longitudinal follow-up of outcome in patients with IIM, including organ-specific morbidity (http://www.euromyositis.net.eu).
References
Footnotes
Funding TS and IS are supported by KG Jebsen Cardiac Research Center and Center for Heart Failure Research, University of Oslo, Oslo, Norway.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement No additional data are available.