Article Text

Abstract
Objective: To evaluate the impact on recovery, of single subacromial injection of methylprednisolone in patients with persistent, post-traumatic impingement of the shoulder.
Design: Randomised, controlled study.
Setting: Large accident and emergency department in Leicester, UK.
Participants: 98 patients with persistent, post-traumatic impingement of the shoulder.
Intervention: Single subacromial injection of methylprednisolone with bupivicaine (group S, n=54) or bupivicaine only (group C, n=44).
Main outcome measures: Pain using a 10 cm visual analogue scale (VAS) and active shoulder abduction.
Results: Comparison of pain scores by the 10 cm VAS between group and group C showed no statistical difference at 3, 6, or 12 weeks. Mean patient pain scores at 12 weeks were 1.38 in both groups (p=0.99). There were 16 patients in group S (mean age 52 years) with a 10 cm VAS greater than 1 (95% CI CI 0.17 to 0.43), compared with 13 patients (mean age 57 years) in group C (95% CI 0.17 to 0.45). Comparison of active shoulder abduction between group S and group C showed no statistical difference at 3, 6, or 12 weeks. Mean active abduction at 12 weeks was 168.9° in group S and 170.3° in group C (p=0.8). There were 10 patients in group S (mean age 60.5) with active abduction less than 170 at 12 weeks (95% CI 0.09 to 0.31), compared with five patients (mean age 62 years) in group C (95% CI 0.04 to 0.24).
Conclusions: Single subacromial injection of methylprednisolone has no beneficial impact on reducing the pain, or the duration of immobility in patients with persistent post-traumatic impingement of the shoulder
- corticosteroids
- impingement
- injection
- shoulder
Statistics from Altmetric.com
Post-traumatic shoulder pain is a common complaint,1 and presents to doctors from many different backgrounds—general practitioners, emergency physicians, rheumatologists, and orthopaedic surgeons, to name but a few. Injuries to the rotator cuff make up a small, though significant proportion of these presentations,2–4 and classically present with signs of painful arc caused by impingement of the cuff under the coracoacromial arch.5 The resulting disabling symptoms of pain and restricted shoulder movement may persist beyond 18 months.6
At present the treatment options include simple rest, analgesia, and physiotherapy,7 and/or subacromial injection of long acting corticosteroids.8 The use of corticosteroids however may have deleterious local9,10 and systemic effects.11–13 Furthermore, systematic reviews of existing studies suggest that the clinical benefit of corticosteroid treatment over rest, analgesia, and physiotherapy remains unproved.14–16 While all the recent studies reviewed suffer from small sample sizes and short follow up,17–20 a more striking failing is that the definition of rotator cuff injury lacks conformity and the shoulder conditions studied are heterogeneous.
The aim of this study was to evaluate the impact on recovery, of single subacromial injection of methylprednisolone in patients with persistent, post-traumatic impingement of the shoulder. Pain relief and the return of active shoulder abduction were the primary outcomes targeted.
METHODS
Participants
All consecutive patients aged over 16 years of age, attending a major accident and emergency department with post-traumatic shoulder pain, and normal radiographs, were reviewed after seven days in a dedicated shoulder research clinic. Participants in the clinic included an orthopaedic surgeon, an accident and emergency consultant, and two specialist registrars in accident and emergency.
Initial assessment and inclusion criteria
Assessment was undertaken using a dedicated form permitting documentation of the mechanism of injury, pre-existing shoulder abnormality, and analgesia use since injury in all patients. Patients were asked to mark the predominant pain level experienced since the injury on a validated 10 cm visual analogue scale (VAS).21 Shoulder examination was undertaken in all patients and monitored by another clinician, with active and passive movements recorded to the nearest 5°.
Patients exhibiting a painful arc and Cyriax signs,22 underwent aseptic subacromial injection (by means of a 21 gauge needle) of 8 ml 0.5% bupivicaine using the posterior approach.23 Complete resolution of pain with full active abduction after injection, permitted a diagnosis of incomplete rotator cuff injury (Neer’s impingement test5). Patients with complete rotator cuff disruption identified by this method were excluded from the trial but offered further appropriate treatment by the orthopaedic surgeon. Patients who did not meet the inclusion/exclusion criteria (table 1) and had a diagnosis other than a rotator cuff tear were treated accordingly and appropriate follow up arrangements made. Patients who were identified as having persistent post-traumatic impingement were invited to enter the trial, and informed consent obtained. Patients who refrained from entering the trial were treated and followed up along existing guidelines.
Sample size and study power
A power calculation undertaken three months into the study indicated that for a mean difference of 1 point in a VAS between groups, a total study size of 98 patients would give 0.80 statistical power.
Procedures for assignment and blinding
Patients who consented to participation in the trial were randomised by computer generated, random numbers obtained by telephone from a remote independent source. Patients were allocated into either a subacromial corticosteroid group (group S), or a control group (group C).
Interventions
Patients randomised to group S received (by an aseptic no touch technique) a single, subacromial injection of 40 mg methylprednisolone (Depomedrone, Upjohn) diluted with 2 ml 0.5% bupivicaine. Group C received no corticosteroid injection.
Both groups of patients were instructed in identical pendulum and wall finger climbing exercises, and asked to perform 20 repetitions of these four times a day.24 Patients were advised to continue with whatever drugs they were already taking and no adjustments were made.
Assessment of effectiveness
All patients were reviewed at 3, 6, and 12 weeks, with repeat pain scores measured by the 10 cm VAS, and measurements made of active and passive shoulder movements. Post-intervention assessment was blinded.
Statistical analysis
The subsequent results were analysed using the SPSS computer package. Parametric data were analysed by means of the two tailed Student t test and non-parametric data by means of the Mann-Whitney U test.25 Statistical significance is displayed by 95% confidence intervals (CI), and p values. All data were analysed on an intention to treat basis.
RESULTS
Recruitment and participation
Over a four year period 306 patients were reviewed in the shoulder clinic. Ninety eight patients met the inclusion criteria (61 men and 37 women, mean age 49, range 17–87 years), and were diagnosed as having persistent, post-traumatic impingement of the shoulder. Eight patients whose symptoms failed to resolve with subacromial injection of bupivicaine were diagnosed as having a complete rotator cuff tear and subsequent magnetic resonance imaging confirmed this (all exclusions listed in table 2).
Fifty four patients were randomised to group S and 44 to group C. Nine patients who were asymptomatic or improving at six weeks (group S=5, group C=4) failed to attend their subsequent appointments despite multiple recalls. Age, sex, analgesia use, baseline pain scores, and shoulder movements were comparable between group S and group C (table 3).
Primary outcomes
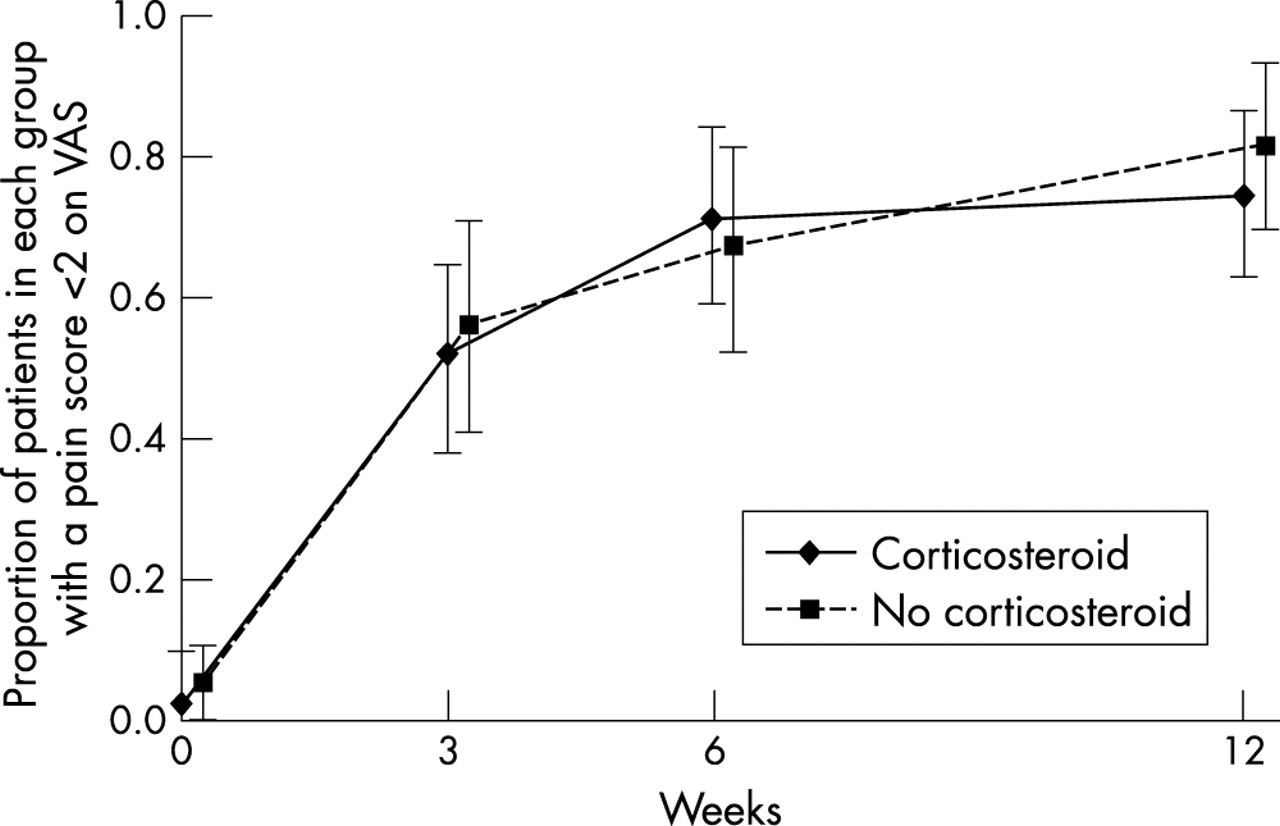
Comparison of pain scores by the 10 cm VAS between group S and group C showed no statistical difference at 3, 6, or 12 weeks (fig 1). Mean patient pain scores at 12 weeks were 1.38 in both groups (p=0.99). There were 16 patients in group S (mean age 52 years) with a 10 cm VAS greater than 1 (95% CI 0.17 to 0.43), compared with 13 patients (mean age 57 years) in group C (95% CI 0.17 to 0.45).
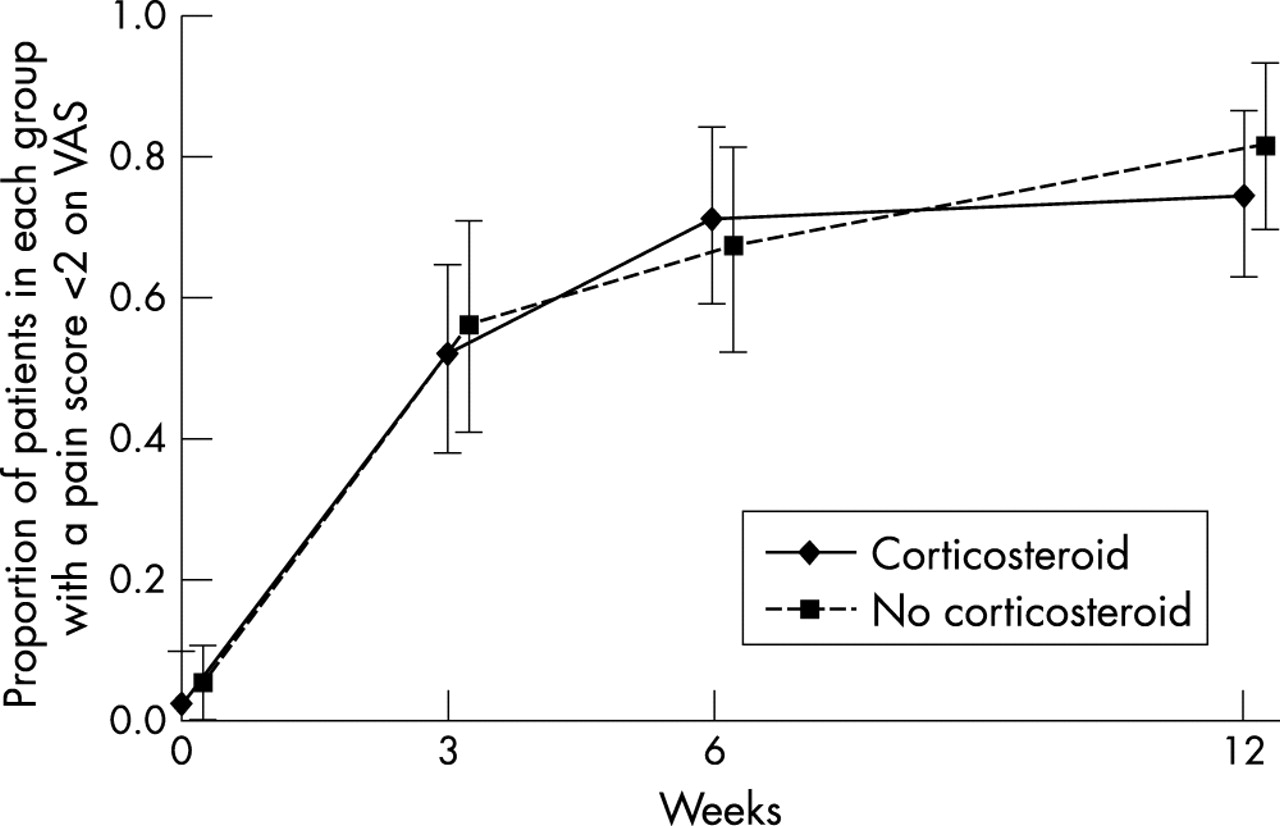
Comparison of improvement in shoulder pain between group S and group C over 12 weeks.
Comparison of active shoulder abduction between group S and group C showed no statistical difference at 3, 6, or 12 weeks (fig 2). Mean active abduction at 12 weeks was 168.9° in group S and 170.3° in group C (p=0.8). There were 10 patients in group S (mean age 60.5) with active abduction less than 170 at 12 weeks (95% CI 0.09 to 0.31), compared with five patients (mean age 62 years) in group C (95% CI 0.04 to 0.24).

{kind=link}
{kind=link}
Comparison of improvement in active shoulder abduction between group S and group C over 12 weeks.
Subgroup analysis by age and sex revealed no statistically significant difference in pain scores, or active abduction between group S and group C.
There were no adverse effects to treatment in either group during the 12 week study period, apart from the post-injection pain flare experienced by patients receiving the corticosteroid injection.
DISCUSSION
This study shows that a single subacromial injection of a long acting depot corticosteroid has no beneficial impact on reducing the pain, or the duration of immobility in patients with persistent post-traumatic impingement of the shoulder. These findings concur with a similar study by White et al,17 who compared triamcinolone with indomethacin in patients with rotator cuff tendinitis. Their study however was not powered and only followed up 22 patients through to six weeks, with the resulting possibility of a type 2 error.
Our results are at odds with a smaller study by Vecchio et al,18 who compared methylprednisolone with lignocaine (lidocaine) alone in rotator cuff tendinitis. They found that patients receiving a corticosteroid injection had improved resisted movement and painful arc scores compared with placebo, although up to 66% patients had no recollection of trauma, and had no radiographs undertaken. The possibility that their study sample consisted of patients with disparate shoulder conditions is high.
Patients with post-traumatic shoulder pain often cause diagnostic difficulty.1 This may account for the variation in the rotator cuff injury classification of previous studies, and explain the variation in conclusion as to “best” treatment in previous systematic reviews.14–16 A study by Bamji et al revealed that diagnostic concordance between consultant rheumatologists when assessing patients with shoulder pain was less than 50%, adversely impacting on choice of treatment.26
A study by Winters et al27 successfully solved this problem by dividing all patients with shoulder pain in a general practice setting into a “synovial group” or a “shoulder girdle group” before allocating treatment. We also simplified diagnosis in our inhospital study by replacing diagnostic terms such as non-calcific rotator cuff tendinitis, partial rotator cuff tear, etc, with the system of reproducible post-traumatic impingement signs described in the methods. Subsequently a homogenous sample was achieved with sufficient power to achieve our aims.
A study by Eustace et al28 has shown that inaccurate placement of corticosteroid injections around the shoulder adversely impacts on outcome. This study differs from the best recent trials17–20 by using the posterior approach, which has been described as the most efficacious route of administration.29
A potential criticism of this study is the lack of treatment double blinding at the initial consultation. Although one other study has described use of a double blind placebo19 we decided that such a method was unlikely to attain true “blindness” as patients invariably experience post-injection pain flare. Furthermore, the accurate, aseptic instillation of a safe placebo is technically difficult to achieve and may in itself introduce study bias. We do accept however that the absence of initial blinding is a potential criticism of our study.
Although previous authors have suggested that corticosteroids may have deleterious local and systemic effects9–13 such adverse effects did not occur during this study and may be secondary to a good technique of corticosteroid administration or because the sample size was comparatively small. The incidence of complication is cited as 1 in 1600 injections, and increases with the frequency of injections.9 Nevertheless, this study shows that subacromial injection of corticosteroid proffers no advantage in persistent, post-traumatic impingement of the shoulder. Consequently even though the risks are small, continued use of corticosteroids cannot be advocated in patients with persistent post-traumatic impingement syndrome.