

Abstract
Objective. Rheumatoid arthritis (RA) is a systemic chronic inflammatory joint disease, whereas osteoarthritis (OA) is a local joint disease with low-level inflammatory activity. The pathogenic role of the adipocytokine adiponectin is largely unknown in these diseases. We hypothesized (1) that plasma adiponectin concentrations differ in healthy controls and patients with early disease-modifying antirheumatic drug (DMARD)-naive RA, chronic RA, and OA; (2) that changes in adiponectin are observed during methotrexate (MTX) treatment of chronic RA; and (3) that adiponectin correlates to disease activity measures in RA.
Methods. Plasma adiponectin was analyzed with a validated in-house immunoassay. We measured adiponectin in healthy controls (n = 45) and patients with early DMARD-naive RA (n = 40), chronic RA (n = 74), and OA (n = 35). In a subgroup of patients with chronic RA (n = 31), the longitudinal effect of MTX treatment on adiponectin (Week 0 vs Week 28) was investigated.
Results. Adiponectin differed significantly between healthy controls (mean 4.8 ± SD 2.7 mg/l) and the 3 groups, with 8.9 ± 4.8 mg/l in early RA, 11.6 ± 5.6 mg/l in chronic RA, and 14.1 ± 6.4 mg/l in OA. Longitudinally, MTX treatment increased adiponectin significantly from 9.7 ± 4.5 mg/l at Week 0 to 11.0 ± 4.5 mg/l at Week 28 in chronic RA. No correlations to disease activity measures were found.
Conclusion. Both early DMARD-naive and chronic RA were associated with higher plasma adiponectin compared to healthy controls, but lower plasma adiponectin than OA. Adiponectin increased 13% during MTX treatment. In patients with RA and OA body mass index, age, sex, and disease activity measures failed to explain the findings.
Adiponectin, an adipocytokine, is mainly synthesized by mature adipocytes and circulates in high concentrations in the bloodstream (0.01% of total serum protein). The adiponectin molecule contains 4 domains: an amino-terminal signal sequence, a variable region, a collagen-like domain, and a C-terminal globular domain1. Adiponectin shares strong sequence homology with complement factor Clq2. Further, it has a similar 3-dimensional structure and conserved amino acid sequences as members of the tumor necrosis factor (TNF) superfamily, suggesting an evolutionary link1. In plasma, adiponectin forms trimers (low molecular weight complexes) that further polymerize into hexamers (mid-molecular weight complexes) and 12- to 18-hexamers [high molecular weight (HMW) complexes]3. The biological activity of adiponectin is elicited by all complexes and also by a proteolytic cleavage product (the globular domain) of adiponectin. The pro- and antiinflammatory roles of the different molecular complexes of adiponectin remain to be clarified4. Both antiinflammatory and proinflammatory effects of adiponectin have been described. Adiponectin reduces the production of TNF-α in cultured macrophages5, and TNF-α and interleukin 6 (IL-6) decrease mRNA expression of adiponectin in adipocytes6. By contrast, adiponectin appears to have proinflammatory effects on various cells from the immune system. In the presence of lipopolysaccharides, HMW adiponectin augmented IL-8 production and the phagocytosis of apoptotic cells by human macrophages7, and adiponectin induced TNF-α and IL-6 secretion from human peripheral macrophages8.
Rheumatoid arthritis (RA) is a systemic chronic inflammatory disease with predilection for synovial joints. The complex autoimmune pathogenesis of RA is not fully clarified; however, proinflammatory cytokines such as TNF-α and IL-6 play a key role9,10, whereas the possible pathogenic role of adiponectin is controversial. Only a few studies concerning RA and adiponectin have been published. An increase in adiponectin during anti-TNF treatment of RA (infliximab and etanercept)11–14, but not adalimumab15, has been observed. Increased plasma adiponectin concentrations are found comparing RA patients and healthy controls16,17, but not OA patients16.
Osteoarthritis (OA) typically affects one or only a few joints with local, low-level inflammatory activity and no signs of systemic inflammation. Both pro- and antiinflammatory properties of adiponectin in different cell types (fibroblasts, chondrocytes) from patients with OA have been reported18–20. OA serum adiponectin was reported to be at the same level as in RA patients, but was higher in healthy controls16.
Other factors influence adiponectin levels. Women have consistently higher adiponectin concentrations than men16,21, whereas the influence of age on plasma adiponectin levels has varied22–25. Obese subjects have lower levels of adiponectin than lean subjects21.
The pro- and antiinflammatory effects of adiponectin led us to hypothesize that plasma adiponectin levels differed among patients with early and chronic RA, OA patients, and healthy controls. In patients with chronic RA undergoing treatment with methotrexate (MTX), no data on adiponectin are available. Therefore, we compared plasma adiponectin levels in patients with very early steroid- and disease modifying antirheumatic drug (DMARD)-naive active RA and chronic RA. OA patients and healthy controls served as controls. Changes in plasma adiponectin during MTX treatment in chronic RA were studied. The effect of glucocorticoid (GC) on plasma adiponectin was investigated in chronic RA. We correlated plasma adiponectin with demographic data and RA disease activity indicators.
MATERIALS AND METHODS
Patients
The study cohort included patients from the Department of Rheumatology, Aarhus University Hospital, Aarhus, Denmark, who had participated in 3 multicenter studies: the CIMESTRA study for early RA26, the MTX study for chronic RA27, and the Hyaluronan study for OA28.
The patients with very early steroid- and DMARD-naive active RA consisted of 40 of 160 patients included in the CIMESTRA study as described26. To be included in the CIMESTRA study, all patients fulfilled the 1987 American College of Rheumatology (ACR) revised criteria for RA29, had active disease duration < 6 months, at least 2 swollen joints at baseline, were age 18–75 years, and were steroid- and DMARD-naive. Laboratory assessment and clinical data included measurement of Disease Activity Score in 28 joints (DAS28), C-reactive protein (CRP), number of swollen joints (NSJ; n = 38), number of tender joints (NTJ; n = 40), and Health Assessment Questionnaire (HAQ). Patients with early RA had a mean age of 50.5 ± 13.0 years. The distribution by sex was 26 women and 14 men. Mean disease duration was 0.3 ± 0.1 years. Mean body mass index (BMI) was 24.9 ± 4.3 kg/m2. Mean DAS28 was 5.3 ± 1.2, and 65% were IgM rheumatoid factor (RF)-positive. Data are listed in Tables 1 and 2.
Clinical and demographic characteristics of healthy controls and patients with early RA, chronic RA, and OA.
Gender distribution of plasma adiponectin, age, disease duration, and BMI in healthy controls and patients with early RA, chronic RA, and OA.
Patients with chronic RA consisted of 74 of 82 patients included in the MTX study27. All patients fulfilled the 1987 ACR revised criteria for RA29. Additional inclusion criteria were either longterm treatment with MTX or start of MTX treatment after at least 4 weeks of washout, if they had previously received another DMARD such as MTX, salazopyrin, myochrisine (aurothiomalate), penicillamine, auranofin, azathioprine, or hydroxychloroquine. Thirty-five patients were MTX-naive (–MTX) and 39 were in steady-state MTX treatment (+MTX). Forty-four patients (59%) did not receive systemic GC, whereas 30 (41%) did. The –MTX were divided into those who received GC (+GC; n = 16) and those who did not (–GC; n = 19; Table 3). Plasma was analyzed before and after MTX treatment in 31 patients at Weeks 0 and 28. The dose adjustment of MTX was based on disease activity and adverse events, aiming at remission. The physician was allowed to add low-dose prednisone while awaiting the response to MTX. Laboratory assessment and clinical data at Weeks 0 and 28 included measurement of CRP, NSJ (n = 38), NTJ (n = 40), and HAQ. Patients with chronic RA (55 women, 19 men) had a mean age of 56.4 ± 11.6 years. Mean disease duration was 13.4 ± 10.6 years; mean BMI was 23.9 ± 5.3 kg/m2; and 82% were IgM RF-positive (Tables 1, 2, and 3).
Clinical and demographic characteristics of 35 MTX-naive patients with chronic RA divided on whether they received glucocorticoid (+GC) or not (–GC).
The OA patients consisted of 35 of 103 patients who participated in a randomized, placebo-controlled, double-blind multicenter study (Hyaluronan)28. All patients fulfilled the ACR criteria for primary OA of the knee30. Inclusion criteria were age > 18 years, moderate to severe OA, and normal CRP. All patients were included at baseline and therefore received no treatment. Exclusion criteria were secondary OA, inflammatory joint disease, radiographic attrition < 5 mm, significant clinical OA of the other knee, comorbidity, intraarticular injections with hyaluronan, intraarticular injections with GC within the previous 3 months, treatment with analgesics/antiinflammatory medication for a condition unrelated to the knee pain, skin conditions overlying the joint that would contraindicate injections, history of allergy to acetaminophen or avian proteins, pregnancy, and breast-feeding. OA patients (22 women, 13 men) had a mean age of 64 ± 9.3 years; mean disease duration was 4.1 ± 3.2 years; mean BMI was 28.9 ± 4.9 kg/m2 (Tables 1 and 2).
Our study also included 45 healthy controls (26 women, 19 men), mean age 49 ± 12.5 years; BMI data were not available (Tables 1 and 2).
Adiponectin determination
Plasma adiponectin levels were determined by a validated in-house time-resolved immunofluorometric assay as described31. All unknown samples were analyzed in duplicate, with an intraassay coefficient of variation (CV) averaging < 5% and interassay CV < 7%.
CRP determination
CRP levels were analyzed at the local departments of biochemistry using standard routine assays.
Statistics
Descriptive data are given as mean ± SD. Normal distribution of data was tested with the Kolmogorov-Smirnov test. The groups were compared with ANOVA if normally distributed, or with the Kruskal-Wallis test. In case of significant p values the Student’s unpaired t test or Mann-Whitney unpaired rank-sum test was used as appropriate. Spearman rank correlation analyses were used to test for relationships between variables. Student’s paired t test was used to compare data obtained before and after MTX treatment. The chi-square test was used to analyze for differences in sex distribution in the groups. A p value < 0.05 was considered statistically significant.
All patients provided written informed consent. Study protocols were approved by local ethics committees and national health authorities. Trials were performed in accord with the Declaration of Helsinki and the International Conference on Harmonisation 1996 revised Guidelines for Good Clinical Practice in the European Community.
RESULTS
Clinical and demographic data
Clinical and demographic data of controls and the 3 patient groups are presented in Tables 1 and 2. Mean age showed no difference between healthy controls and early RA, but differed significantly among healthy controls and patients with chronic RA and OA. No gender differences were observed between the 4 groups. Disease durations between the 3 patient groups differed significantly. OA patients had significantly higher BMI than RA patients. Mean DAS28 was 5.2 ± 1.2 for early RA, indicating a high degree of active disease. In early RA, NTJ and NSJ were significantly higher than in chronic RA. CRP and HAQ did not differ significantly between early and chronic RA, although levels were higher among early RA. All OA patients had normal CRP (< 75 nmol/l).
Comparing gender-related distributions in age, disease duration, and BMI, we found significant age differences in men and women in the early RA group, but no other statistical differences were observed (Table 2).
NTJ and HAQ differed significantly between MTX-naive chronic RA patients with and without GC treatment (Table 3).
Plasma adiponectin levels
Adiponectin levels in healthy controls were significantly lower than in the 3 patient groups (Table 1, Figure 1). Among the patients, early RA patients had the lowest plasma adiponectin levels, followed successively by the chronic RA patients and OA patients. Plasma adiponectin levels differed significantly among the 3 patient groups (Table 1, Figure 1).

Plasma adiponectin levels in healthy controls and patients with early RA, chronic RA, and OA. Horizontal line represents the median and broken line the mean. Boxes represent 25th and 75th percentiles; whiskers indicate 10th and 90th percentiles; circles represent outliers.
Thirty-one MTX-naive chronic RA patients were studied before and after 28 weeks of MTX treatment. Plasma adiponectin increased from 9.7 ± 4.5 mg/l at Week 0 to 11.0 ± 4.5 mg/l at Week 28. Thus, MTX treatment increased plasma adiponectin significantly by 13% (Figure 2).

Plasma adiponectin levels in 31 patients with chronic RA at Week 0 (before MTX treatment) and at Week 28 (after MTX treatment).
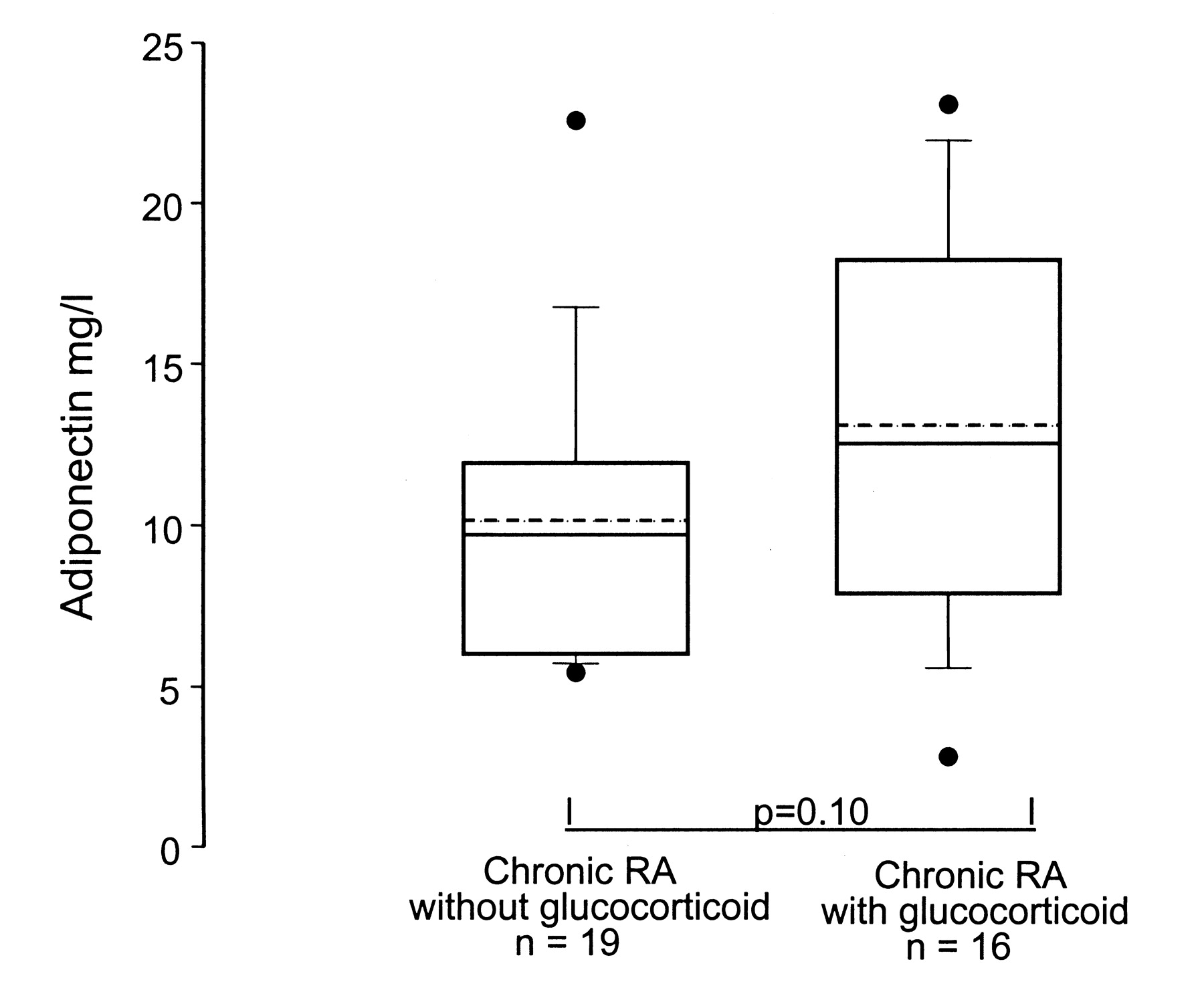
Plasma adiponectin was similar in chronic RA patients with and without GC treatment, but there was a trend toward higher plasma adiponectin in chronic RA patients treated with GC (Table 3, Figure 3).

Plasma adiponectin levels in patients with chronic RA treated without and with glucocorticoids. Horizontal line represents the median and broken line the mean. Boxes represent 25th and 75th percentiles; whiskers indicate 10th and 90th percentiles; circles represent outliers.
In both healthy controls and the patient groups, women had higher levels of adiponectin than men, reaching statistical significance in healthy controls and chronic RA and OA patients, but not in early RA patients (Table 2).
Between plasma adiponectin and demographic data only a few correlations were found: age was positively correlated to plasma adiponectin in patients with chronic RA (p < 0.001, r = 0.28) and in patients with OA (p < 0.001, r = 0.56).
No correlations between plasma adiponectin and disease activity indicators (DAS28, CRP, NTJ, NSJ, and HAQ) were found in early or chronic RA.
DISCUSSION
The main finding in our study was that very early steroid- and DMARD-naive patients with active RA had higher levels of adiponectin than healthy controls, and lower levels than both chronic RA and OA patients. In chronic RA, a clinically effective MTX treatment was associated with an increase in plasma adiponectin, and plasma adiponectin tended to be higher in GC-treated than in untreated patients. Finally, there was no relationship between plasma adiponectin and the clinical disease activity measures in patients with RA.
Patient groups were not strictly comparable concerning BMI, as OA patients had higher BMI than both the RA groups. Obese subjects are known to have lower adiponectin levels than lean subjects21, and accordingly, our OA patients were expected to have the lowest adiponectin concentrations, but we found the opposite. Thus, BMI status failed to provide an explanation for our results.
It is well known that women have higher adiponectin plasma levels than men16,21. The proportion of females was lowest in the healthy controls (57%), equal in the early RA and OA groups (65% and 63%), and highest in the chronic RA group (74%). This gender difference was not statistically significant and is not likely to explain all the observed differences in adiponectin levels, although the lower proportion of women among healthy controls could contribute to the lower adiponectin level, and similarly the high proportion among chronic RA patients to a higher level in this group.
In terms of age, OA patients were older than both RA groups and healthy controls (Tables 1 and 2). Conflicting observations concerning age-related changes in plasma adiponectin have been published: positive23,24, negative22, and no correlations25 have been described. In our study groups, we found a positive correlation between plasma adiponectin and age in chronic RA and OA. One previous study described an increase in adiponectin of approximately 1 mg/l for men and 0.5 mg/l for women, comparing subjects aged 50 to 65 years24. In our study the mean age differed about 15 years between healthy controls (49.5 yrs) and OA patients (64.0 yrs), and the difference in mean plasma adiponectin level between healthy controls and OA was considerably larger than 1 mg/l (about 9 mg/l). Thus, the age difference hardly explains more than a small part of the observed difference between RA and OA patients.
In the group of patients with early RA with high disease activity and a high level of proinflammatory cytokines, we found a relatively low level of adiponectin. We expect this level to increase during effective treatment, but these data are not available yet. However, in the group of patients with chronic RA who had been treated effectively with MTX we saw a clear increase in the adiponectin level. Our findings are in agreement with several recent reports on anti-TNF treatment11–14. Together these observations indicate a reverse relationship between disease activity/systemic inflammation and adiponectin level in RA.
Patients with inflammatory diseases such as systemic lupus erythematosus32, ulcerative colitis33, and type 1 diabetes34 have shown elevated levels of adiponectin. It has been suggested that the elevated adiponectin levels represent a beneficial counter-regulatory mechanism serving to protect the patient from harmful effects of different diseases35. In both early and chronic RA we found elevated adiponectin levels that did not correlate with disease activity indicators, and we similarly speculate that the elevated adiponectin has a counter-regulatory function in this disease. Thus, in RA high plasma adiponectin is counter-regulatory for inflammation, and future research will show if it protects against radiographic progression of joint destruction.
In agreement with others we found the highest plasma adiponectin in OA patients compared with healthy controls, but, in contrast to others, higher plasma adiponectin in OA than in RA patients16. These results indicate that systemic inflammation, and thus increased proinflammatory cytokines in the circulation, is probably not necessary for upregulation of plasma adiponectin, at least not in OA. Both in RA and in OA, research concerning the mechanisms and the molecules that regulate adiponectin synthesis and secretion from adipocytes is still needed.
Patients with chronic RA without GC treatment had lower plasma adiponectin levels than patients treated with GC. It has been reported that adiponectin concentrations in RA and OA were comparable16, but 80% of the RA patients were treated with GC. Taking our results into account, GC treatment may be responsible for the comparable levels between RA and OA patients we studied. Numerous findings support a relationship between GC use and adiponectin. Thus, GC inhibited the secretion of 2 inhibitors of adiponectin synthesis, namely TNF-α36,37 and IL-638,39, which is in agreement with our results. However, opposite effects of GC on adiponectin synthesis have also been reported: in vitro, dexamethasone suppressed adiponectin gene expression in 3T3-L1 adipocytes40, and inhibited release of adiponectin from subcutaneous adipocytes from obese subjects41. Halleux, et al42 have observed that dexamethasone downregulated the expression of adiponectin mRNA in human visceral adipose tissue.
RA disease activity measures did not correlate with adiponectin in DMARD-naive patients with early RA and with chronic RA. Indeed, negative11, positive17, and nonsignificant15 correlations between serum adiponectin levels and disease activity have been observed. Based on our observations, adiponectin does not behave as an acute-phase reactant in early DMARD-naive and chronic RA.
Plasma levels of adiponectin in steroid- and DMARD-naive patients with very early active RA were higher than in healthy controls and lower than in patients with chronic RA or OA. Further, we found that plasma adiponectin increased during 28 weeks of clinically effective treatment with MTX. BMI, age, sex, and disease activity measures failed to explain the findings. Further studies are needed to clarify the possible pathogenic role of adiponectin in RA and OA.
Acknowledgments
The authors thank Hanne Petersen and Lis Lund for skillful laboratory assistance.
Footnotes
-
Supported by the Danish Medical Research Council (Dr. Frystyk and Dr. Flyvbjerg), The Danish Rheumatism Association, and the Institute of Clinical Medicine, Aarhus University.
- Accepted for publication March 27, 2009.








{kind=link}
{kind=link}
{kind=link}