

Abstract
Objective. Methotrexate (MTX) has been associated with reduced risk for cardiovascular disease (CVD) events among patients with rheumatoid arthritis (RA) not exposed to biologic disease-modifying antirheumatic drugs (bDMARDs). The effect of concomitant MTX on CVD risk among RA patients initiating bDMARDs remains unknown.
Methods. A retrospective cohort study was conducted to assess the effect of MTX on CVD risk using 2006–2015 Medicare claims data for patients with RA initiating bDMARD. The main exposure was current use of MTX, updated in a time-varying fashion. The primary outcome was a composite of incident myocardial infarction (MI), stroke, and fatal CVD. Secondary outcomes were each event that comprised the primary outcome. Incidence rates (IR) and 95% CI were calculated using Poisson regression. Associations between MTX and risk of CVD were assessed using Cox regression.
Results. A total of 88,255 bDMARD initiations and 1861 CVD events were included in this study. Mean age was 64.6 (12.3) years, 84.0% were female, and 68.2% were non-Hispanic White. The crude IRs (95% CI) for CVD were 17.9 (16.9–18.8) and 12.1 (11.1–13.2) per 1000 patient-years among MTX unexposed and exposed, respectively. The multivariable adjusted HR (95% CI) for CVD events associated with MTX was 0.76 (0.68–0.85). Multivariable adjusted HRs were 0.78 (0.66–0.91), 0.74 (0.62–0.88), 0.77 (0.68–0.86), and 0.82 (0.73–0.93) for MI, stroke, MI or stroke, and a composite CVD outcome, respectively. Results were robust in sensitivity and subgroup analyses.
Conclusion. Among patients with RA receiving biologics, concomitant MTX use was associated with a 24% lower risk for CVD events.
Rheumatoid arthritis (RA) is a chronic inflammatory polyarthritis affecting approximately 0.5–2% of the population.1,2,3 Without effective treatment, RA often leads to joint destruction, deformity, loss of function, disability, poor quality of life, and shortened life expectancy.4–10 Inflammatory features of RA are characterized by elevated production of cytokines and inflammatory markers (interleukin 1 [IL-1], IL-6, C-reactive protein [CRP], and tumor necrosis factor). Cytokines play an important role in the increased risk for cardiovascular disease (CVD) in RA patients, and they also are shown to promote atherosclerosis.11,12,13 Accelerated atherosclerosis remains important to rheumatologists given that CVD-related deaths account for a 50% excess mortality in patients with RA.14
Methotrexate (MTX) is the first-line disease-modifying antirheumatic drug (DMARD) recommended for the treatment for RA.15,16 RA patients with intolerance or with inadequate response to MTX typically add or switch to biologic DMARDs (bDMARDs). While many bDMARDs (e.g., tocilizumab [TCZ], sarilumab) have appreciable efficacy for RA treatment even in the absence of concomitant MTX use, other bDMARDs (e.g., infliximab, adalimumab) are clearly more effective when administered with concomitant MTX.17
A number of studies and metaanalyses have demonstrated that MTX is associated with reduced risk for CVD.18–28 Most studies concluded mechanistically that this effect is mediated primarily by controlling systemic inflammation or reducing serum cytokines.29 A large-scale US National Institutes of Health–funded trial, Cardiovascular Inflammation Reduction Trial (CIRT), showed no benefit of MTX on CVD prevention in patients with diabetes or metabolic syndrome with known coronary disease.30,31 However, there was no requirement that participants have any meaningful degree of systemic inflammation (e.g., as measured by elevated CRP), and there may have been other reasons (e.g., dosing) underlying the negative finding in this population. For patients with autoimmune or inflammatory conditions who are receiving other immunomodulatory therapies that may reduce systemic inflammation (e.g., bDMARDs), the incremental benefit of concomitant MTX on CVD risk is not clear. Therefore, the objective of this study was to assess the association between MTX and CVD risk when administered concomitantly with bDMARDs to patients with RA.
METHODS
Population and data source. This study utilized Medicare claims data for all patients with RA from January 1, 2006, to September 30, 2015. Medicare is a government-sponsored health plan provided to > 90% of US residents aged ≥ 65 years. Medicare also covers individuals aged < 65 years if disabled (e.g., due to RA) or with endstage renal disease.
RA cohort definition and biologic exposure. A retrospective cohort study was conducted among adult patients with RA who initiated a bDMARD between January 1, 2007, to September 30, 2015. Injection bDMARDs were identified from Medicare pharmacy data using national drug codes (NDC) and infusion therapies identified using Healthcare Common Procedure Coding System (HCPCS) codes. Infusion drugs in the first year, after regulatory approval and before a permanent HCPCS code was available, were identified using a published algorithm with sensitivity 94%, specificity 100%, and PPV 97%.32 To be considered a new user for each bDMARD, patients with RA had to have a minimum of 365 days of prior data with no previous claim for the specific therapy. This time period was referred to as the baseline period for assessing comorbidities. Patients with RA initiating a bDMARD who did not meet this criterion would have been prevalent users and, while excluded from analysis of that specific bDMARD, might still have qualified for initiation of other bDMARDs. RA was identified using ≥ 2 claims with International Classification of Disease, 9th Revision, Clinical Modification (ICD-9-CM) codes for RA assigned by a physician, separated by 7 days and occurring within 1 year. To make sure the treatment was for RA, patient diagnosis codes for other autoimmune/inflammatory disease at baseline were excluded. Patients with diagnosis codes for malignancy other than nonmelanoma skin cancer, HIV, or organ transplantation before bDMARD initiation (using all available data) were also excluded. Initiations for RA patients with a diagnosis code for myocardial infarction (MI; ICD-9-CM 410.xx), history of MI (412.xx), or stroke (430.xx, 431. xx, 433.xx, 434.xx, and 436.xx) before initiation date (using all available data) were excluded to allow for the study of incident CVD events. For a broader composite CVD event, we included all of the above, plus angina, coronary artery bypass grafting (CABG), and percutaneous coronary intervention (PCI) as outcomes. For this outcome, patients with an ICD-9-CM diagnosis code for other acute and subacute forms of ischemic heart disease (411.xx), angina (413.xx), heart failure (428.9x), other forms of chronic ischemic heart disease (414.xx), or ICD-9-CM procedure code or common practice terminology code (CPT) for CABG and PCI before the initiation date were excluded.
Primary exposure definitions for MTX use. Time-varying MTX use was defined as current exposure (i.e., days of supply, without extension), and updated for each person-day. In a sensitivity analysis, a 90-day extension was added to days of supply of MTX. A second sensitivity analysis defined “concomitant MTX” in a nontime-varying (i.e., fixed) fashion as any prescription for MTX within 120 days after initiation of bDMARDs. This sensitivity analysis required patients be event-free for those 120 days, and therefore, follow-up started at Day 121 to avoid immortal person-time bias. Demographic characteristics, comorbidities, and health behaviors. Age was updated at each bDMARD initiation. We identified history of CVD other than MI or stroke using all available data and other covariates using data in the 365 days prior to each bDMARD initiation date, which was also defined as baseline. Both comorbidities and healthcare utilization were dichotomous and identified using ICD-9-CM diagnosis codes. Using NDC and HCPCS codes, we also identified patients’ concurrent medications. Glucocorticoid dose was calculated as a 183-day average before initiation and classified as none, low dose (< 7.5 mg/day), or higher dose (≥ 7.5 mg/day). Statin use was identified using NDC codes and classified as none, low, medium, and high potency33 based on the last prescription in baseline. Folic acid use was identified using NDC codes and defined dichotomously and as time-varying. Nonalcoholic fatty liver disease and metabolic syndrome were defined using ICD-9 diagnosis codes using all available data before index date as fixed covariate for concomitant MTX analysis, and using all available data before and after index date as time-varying covariate for time-varying MTX analysis.
CVD outcome assessment. The primary outcome was a composite of incident MI, stroke, and fatal CVD. Incident MI was defined as at least 1 ICD-9-CM diagnosis code for MI (410.x1) from a hospital discharge with at least a 1-night stay in a hospital, unless the patient died (PPV ≥ 90%).34 Incident stroke was defined as at least 1 ICD-9-CM diagnosis code for stroke (430.xx, 431.xx, 433.x1, 434.x1, and 436.xx) from a hospital discharge (PPV ≥ 90%).35 Fatal CVD was identified by a validated claims-based algorithm with PPV ≥ 80%.36 The secondary outcomes were individual components of the primary outcome. A broader CVD outcome definition included angina identified using ICD-9 diagnosis codes, CABG and PCI using both ICD-9 procedure codes and CPT codes.
Follow-up. Follow-up began at the initiation of each specific bDMARD medication and ended at the earliest of (1) end of exposure to each specific agent (i.e., days of supply for injection bDMARDs or the standard dosing interval for infusion bDMARDs) plus a 90-day extension, (2) a switch to another bDMARD or tofacitinib, (3) CVD outcome, (4) death date (inclusive for fatal CVD), (5) loss of Medicare coverage, or (6) end of study.
Statistical methods. Descriptive statistics were calculated for covariates of interest, comparing patients with and without MTX use on their biologic initiation date, and characterizing the distribution of those risk factors during follow-up according to MTX exposed vs unexposed person-time. Mean and SD were calculated for continuous variables, and proportions were calculated for categorical variables. Standard mean differences (SMD) were calculated for both continuous and categorical variables; SMD > 0.1 was considered as indication for imbalance. Incidence rates (IRs) of CVD were calculated by dividing number of events by person-years (PY) exposed; 95% CIs were estimated with Poisson regression. Unadjusted and multivariable adjusted HR (aHR) and 95% CI were estimated using Cox regression. Age; sex; race; heart failure; atrial fibrillation; abdominal aortic aneurism; peripheral arterial disease; diabetes; hyperlipidemia; hypertension; obesity; chronic kidney disease (CKD); chronic obstructive pulmonary disease (COPD); fibromyalgia; any hospitalized infection; any hospitalization; number of physician visits; MTX, hydroxychloroquine, leflunomide, sulfasalazine, NSAID, and statin use and potency; other lipid-lowering drug use at baseline; number of other bDMARDs used prior to initiation; oral glucocorticoid dose in the 6 months before initiation; smoking, low income (i.e., enrolled in state buy-in program); and reason for Medicare eligibility other than age (e.g., disability) were included in the multivariable adjusted model. Robust sandwich covariance matrix estimate was used to account for the clustered nature of the data, since each patient could initiate multiple bDMARDs over time and thus contribute > 1 treatment episode (with the time axis reset and covariates updated). The proportional hazard assumption was assessed in the fixed concomitant MTX analysis and was not violated.
A subgroup analysis that included patients previously exposed to MTX was performed to ensure that the comparator group not exposed to MTX was at some point in the past deemed well enough to have received it. This subgroup would expect to therefore exclude individuals with strong (but potentially unmeasured) confounding related to factors for which clinicians would not give patients MTX (e.g., alcoholism, noncompliance with MTX-related monitoring, chronic liver disease) that might not be measured well in health plan data. A second subgroup analysis evaluated risk according to specific bDMARD used. One variable with 16 levels (e.g., abatacept with MTX, abatacept without MTX) was created and included in a multivariable adjusted Cox model; the effect of MTX on the risk for CVD for each bDMARD was calculated with a contrast statement.
Using external adjustment methods, potential confounding for RA disease activity was examined using the multibiomarker disease activity (MBDA) test results,37 assessed in the subgroup of patients who had their data linked to MBDA test results (within 6 months before bDMARD initiation) according to the method described by Schneeweiss et al.38 The effect size of MBDA (RRCD) on CVD risk was 1.5-fold elevated for patients in moderate or high RA disease activity compared to people who had low RA disease activity, measured by the MBDA37.
All analyses were conducted using SAS 9.4 (SAS Institute Inc.). Use of the Medicare data was governed by a Data Use Agreement (DUA) with the Centre for Medicare and Medicaid Services. The Institutional Review Board of the University of Alabama at Birmingham approved the study (IRB-121029003). As this was a retrospective observational cohort study, participants were not required to provide informed consent.
RESULTS
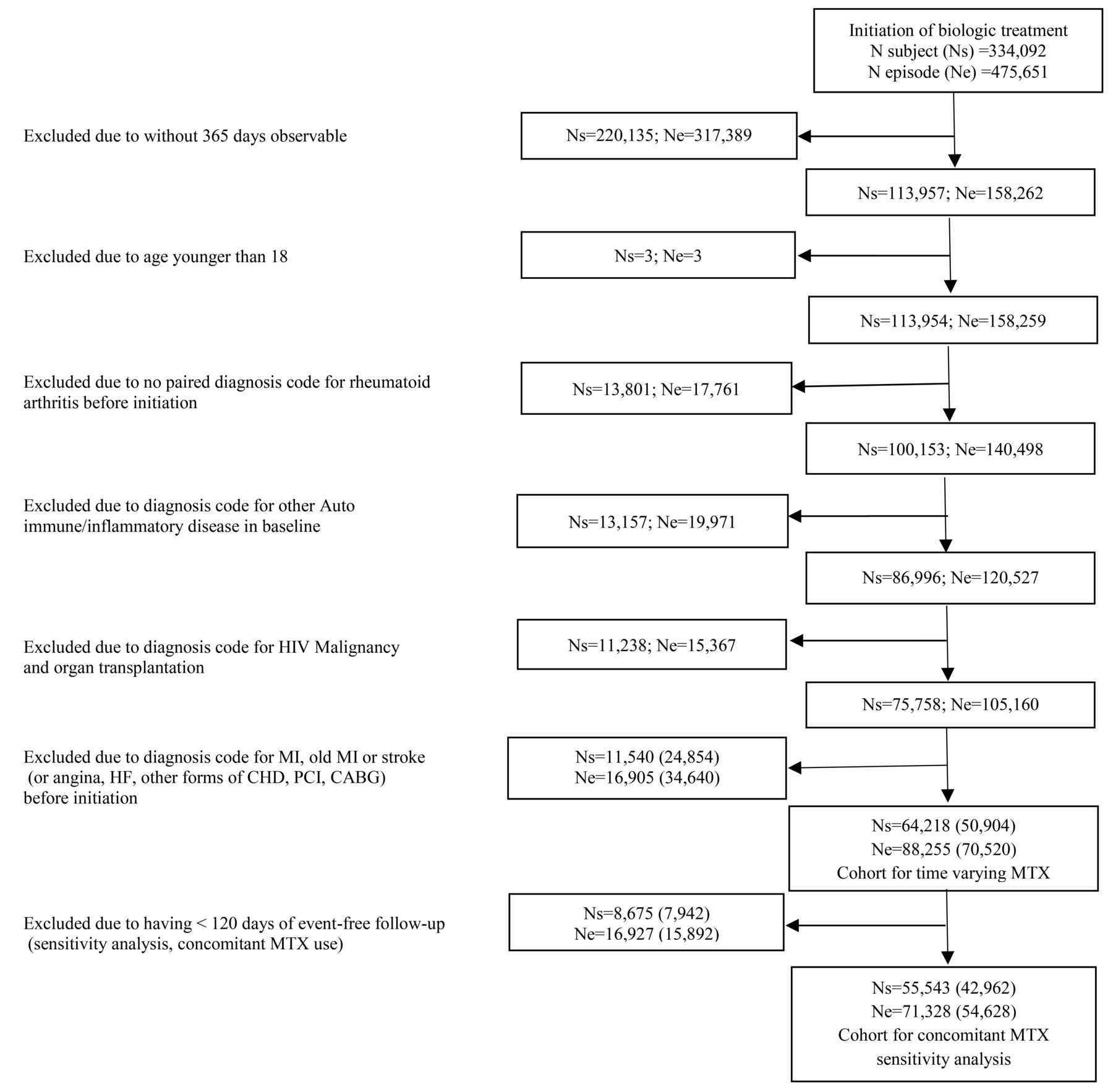
A total of 475,651 bDMARD initiations from 334,092 patients were identified. After applying the inclusion and exclusion criteria, 88,255 initiations (64,218 patients) were included in the main analysis, and 71,328 initiations (55,543 patients) in the fixed concomitant MTX sensitivity analysis (Figure 1). In the overall cohort, in weighting the exposure groups by their respective size, the average age at initiation was 64.6 (12.3) years, 84.0% were female, and 68.2% were non-Hispanic White.

Flowchart for RA cohort selection. Note that an “episode” refers to initiation of a specific biologic medication for RA. Patients could have initiated more than 1 biologic over the study time period and therefore contributed more than 1 episode to the analysis. CABG: coronary artery bypass grafting; CHD: coronary heart disease; HF: heart failure; MI: myocardial infarction; MTX: methotrexate; Ne: N episode; Ns: N subject; PCI: percutaneous coronary intervention; RA: rheumatoid arthritis.
Patients with MTX use (38.8%) concomitant to bDMARD initiation date were similar to patients without MTX use in age, sex, and race (Table 1). MTX users were more likely to initiate infliximab, be bDMARD-naïve, and be less likely to use leflunomide at baseline. They had a lower prevalence of CKD and COPD. They were somewhat less likely to have liver disease or a hospitalized infection, had fewer physician visits, and were less likely to be considered disabled by Medicare. Median (IQR) follow-up time was 288 (148–602) days.
Distribution of baseline characteristics by MTX use at the time of biologic initiation.
Association of MTX use with CVD risk. A total of 1324 composite CVD events were identified over 74,127 MTX unexposed PY, resulting in an IR of 17.9 (95% CI 16.9–18.8; Table 2) per 1000 PY. A total of 537 composite CVD events were identified during 44,312 MTX exposed PY, resulting in an IR of 12.1 (95% CI 11.1–13.2) events per 1000 PY. Given this difference of approximately 5/1000 PY, the number of RA patients needed to treat (NNT) with MTX for 1 year to prevent 1 additional composite CVD event would be about 200. The unadjusted HR (Table 2) was 0.68 (95% CI 0.61–0.75) and the multivariable adjusted HR (Figure 2, top panel) for exposure was 0.76 (95% CI 0.68–0.85). Multivariable adjusted HRs consistently showed a protective effect for MTX for the 4 CVD outcomes studied: MI (HR 0.78, 95% CI 0.66–0.91); stroke (HR 0.74, 95% CI 0.62–0.88); composite of MI or stroke (HR 0.77, 95% CI 0.68–0.86); and a broader CVD event definition including the above events plus angina, CABG, and PCI (HR 0.82, 95% CI 0.73–0.93). There was a suggestion of a protective effect for hydroxychloroquine (0.92, 95% CI 0.82–1.03 for MI outcome) that was not significant.
Incidence rate and unadjusted HR of composite CVD events, MI, and stroke associated with time-varying MTXa use, referent to MTX unexposed.

Forest plot showing the adjusteda HR for CVD risk associated with MTX in the primary analysis and sensitivity analyses referent to MTX nonuse, varying the definition used for MTX exposure. Primary outcome including MI, stroke, and fatal CVD, identified with algorithm with cutpoints for positive predictive value ≥ 0.80. CVD plus includes MI, stroke, fatal CVD, angina, coronary artery bypass grafting, and percutaneous coronary intervention. Concomitant MTX was defined as any prescription within 120 days after initiation of bDMARD.
a Adjusted for age, sex, race, Charlson comorbidity index, bDMARDs initiated, baseline MTX, hydroxychloroquine, leflunomide, sulfasalazine, heart failure, atrial fibrillation, abdominal aortic aneurism, peripheral arterial disease, diabetes, hyperlipidemia, hypertension, obesity, chronic kidney disease, chronic obstructive pulmonary disease, fibromyalgia, any hospitalized infection, any hospitalization, number of physician visits, nonsteroidal antiinflammatory drugs, statin potency, other lipid-lowering drug use at baseline, number of biologics used prior to initiation, oral steroid dose in 6 months before initiation, smoking, state buy-in (i.e., low income), and reasons for Medicare eligibility other than age (e.g., disability). For time-varying MTX, analysis was also adjusted for time-varying folic acid, nonalcoholic fatty liver disease, and metabolic syndrome. For concomitant MTX, analysis was also adjusted for folic acid, nonalcoholic fatty liver disease, other forms of liver disease, and metabolic syndrome assessed using baseline data. AMI: acute myocardial infarction; bDMARD: biologic disease-modifying antirheumatic drug; CVD: cardiovascular disease; IR: incidence rate per 1000 patient-years; MI: myocardial infarction; MTX: methotrexate.
The sensitivity analysis for time-varying MTX exposure with a 90-day extension resulted in similar IRs and aHRs compared with the main analysis (Figure 2, middle panel) and found a multivariable adjusted HR for the composite CVD outcome of 0.85 (95% CI 0.75–0.96). The sensitivity analysis for concomitant MTX as a fixed exposure resulted in similar IRs (Figure 2, bottom panel); the multivariable adjusted HRs were all < 1.0, although some CI included 1.0.
Subgroup analyses. The subgroup analysis limited to RA patients who used MTX prior to bDMARD initiation resulted in similar HR to the main analysis (Table 3). The overall multivariable adjusted HR for composite CVD was 0.76 (95% CI 0.67–0.85) for MTX use. The IRs for composite CVD for bDMARDs without MTX exposure updated in a time-varying fashion ranged from a low of 14.6 (95% CI 11.8–18.0) for TCZ initiators to a high of 22.4 (95% CI 20.1–25.0) for infliximab initiators (Supplementary Table 1, top panel, available with the online version of this article). The IRs for composite CVD events for bDMARDs with concomitant MTX exposure updated in a time-varying fashion ranged from a low of 8.6 (95% CI 5.5–13.5) for TCZ initiators to a high of 13.6 (95% CI 10.2–18.3) for rituximab initiators (Supplementary Table 1, top panel, middle). Contrasts for comparing CVD risk with and without MTX exposure ranged from a low of 0.59 (95% CI 0.36–0.98) for certolizumab pegol initiators to a high of 0.93 (95% CI 0.70–1.23) for etanercept initiators. All remaining contrasts evaluating risk for the composite CVD outcome were within these boundaries, and all were < 1. Contrasts for each component of the CVD outcome (MI, stroke, or either) generally were similar to that for composite CVD (Supplementary Table 1, lower 3 quarters).
Subgroup analysis evaluating the incidence rate and hazard ratio of composite CVD events and each component associated with MTX use, restricted to patients exposed to MTX at any time before initiation of biologic DMARDs.
External adjustment for disease activity. The proportion of moderate or high MBDA scores was 87.0% among all MBDA tests (n = 123,921) analyzed. Measured at the start of biologic therapy, the proportion of RA patients with moderate or high MBDA scores were nearly identical, comparing bDMARD initiators with and without MTX (94% vs 93%). Assuming an HR of 1.5 for the association between moderate/high MBDA score and CVD based on published data, external adjustment for the MBDA by exposure group therefore led to no change in the overall estimated HR for composite CVD associated with time-varying MTX use (aHR = 0.76).
DISCUSSION
In this retrospective cohort study of Medicare-insured RA patients who initiated bDMARDs, we observed a 24% reduction in the risk for CVD events associated with concomitant MTX use. The observed results were robust in 2 sensitivity analyses and a subgroup analysis of patients who had been taking MTX previously but had discontinued it. These findings lend additional support to MTX yielding an incremental benefit to reducing CVD risk, even among RA patients treated with biologics. We note that the absolute rate difference of the composite CVD event of approximately 5/1000 PY and the associated NNT of about 200 is relatively small. By itself, a benefit of this magnitude is unlikely to be a strong motivator for patients or clinicians. Nevertheless, for those taking MTX mainly for its clinical effects to treat RA, its potential benefits to further reduce CVD risk may be compelling.
Several previous studies have demonstrated that MTX is associated with a reduced risk for CVD events among patients with RA using conventional synthetic DMARD.18,19,20,21,28 In a prospective single-center study including 1240 patients with RA between January 1, 1981, and December 31, 1999, Choi, et al18 found the HR associated with MTX use for CVD death was 0.3 (95% CI 0.2–0.7). In a study including veterans with RA, Prodanowich et al19 found the risk ratio for CVD for MTX use was 0.83 (95% CI 0.71–0.96). Suissa, et al21 conducted a cohort study using the PharMetrics claims database and found the risk ratio for MI for MTX use to be 0.81 (95% CI 0.60–1.08). These studies were conducted among patients with RA never exposed to bDMARDs and are compatible with the aHR we observed (0.76, 95% CI 0.68–0.85). Of importance from a study design perspective, because MTX is now considered an “anchor drug” in the treatment of RA, it is challenging to construct a reasonable comparator therapy for MTX in any contemporary analysis, given how it is used in RA. Thus, our study design where all patients were initiating bDMARDs, with some receiving background MTX and others not, is particularly relevant in terms of being able to study its effects in the modern era.
The clinical implications of our study are notable. While combination therapy with MTX may only marginally increase the clinical efficacy of some bDMARDs (e.g., TCZ), combination therapy may further reduce the risk for CVD. The recently completed CIRT showed no benefit of MTX for CVD risk reduction among patients with stable coronary artery disease and either type 2 diabetes or metabolic syndrome who were not selected on the basis of having systemic inflammation.31 In contrast, the Canakinumab Antiinflammatory Thrombosis Outcome Study (CANTOS) showed that when given to patients with prior MI with elevated inflammatory markers (high-sensitivity CRP ≥ 2 mg/L), canakinumab led to a 17% reduction in the risk of heart attack, stroke, urgent need for revascularization, or CVD. The effect size of MTX for CVD risk reduction that we observed in RA patients treated with bDMARDs is comparable to the effect size associated with canakinumab. Our study suggests that when tolerability is not a problem, concomitant MTX to bDMARDs not only improves symptoms and reduces the risk for radiographic progression but may offer the possibility of further reduction of CVD risk.
Our study has several strengths. We included fatal CVD as a part of a CVD composite outcome. Fatal CVD was identified through a validated claims-based algorithm36; not including fatal CVD events in such an analysis will underestimate the IR for CVD events and may result in biased estimates of its exposure-outcome associations. We used a validated algorithm32 to identify infusion represented with nonspecific HCPCS codes 3490 and 3590 before a permanent HCPCS code was available; failure to identify these infusion drugs will reduce the sample size and, more importantly, will misclassify some prevalent users as new users by misclassifying their initiation date. Our large sample size made it possible to assess effect of MTX on CVD risk according to specific bDMARD exposure and to estimate IRs and HRs with high precision. We used the MBDA to assess the distribution of disease activity, recognizing the potential for residual confounding due to unmeasured factors such as RA disease activity, and given that large claims databases typically lack laboratory test results. There was no difference in the proportion of patients with moderate or high MBDA biomarker scores between patients initiating bDMARDs with or without MTX. Recognizing that a 1-time measurement of the MBDA is not a gold standard to control for the influence of RA disease activity on the cardiovascular system and noting that other clinical measures of disease activity were not available in this data source, this approach nevertheless may help address the concern that RA disease activity, previously shown to be associated with CVD risk,39 might confound our observed associations. This concern may be further attenuated given that all patients were initiating biologic therapy, making baseline disease activity more likely to be in the moderate-to-high end of the range and thus more comparable between the MTX and the non-MTX exposure groups.
Our study has limitations common to other studies using administrative data. Despite adjusting for a multitude of covariates, some may be unascertained (e.g., obesity), misclassified (e.g., smoking, over-the-counter folate), or unavailable (e.g., family history). Claims data contain information only on whether a prescription was filled, and patients filling a prescription do not necessarily take the medication as directed, and thus we could have misclassified exposure. For this reason, we did not study MTX dose, given that patients could change dose (particularly down-titration) without requiring a new prescription. We also recognize that patients discontinue MTX for a variety of reasons, only some of which could be controlled for in this type of data source. CVD outcome events were not adjudicated individually, although we relied on claims-based algorithms that have a positive predictive value in excess of 80–90% in their accuracy, and there is little reason to expect that performance of these would be differential by specific biologic exposure or MTX use. Finally, a minority of RA patients had MBDA test results available for external adjustment; patients may have been tested with the MBDA up to 6 months prior to bDMARD initiation, and tested patients may be systematically different from those not tested.
In conclusion, our observational study suggests an overall 18–25% reduction of CVD risk associated with MTX use, incremental to the inflammatory disease control conferred by concomitant biologic use. These findings provide additional information to support the importance of optimal disease activity control and reduction of inflammation attainable by combination RA therapy with MTX.
Footnotes
Support for this research was provided in part by the Patient Centered Outcomes Research Institute (PCORI): PPRND-1507-32163. PCORI had no role in the writing of or decision to publish the manuscript.
JRC receives research grants and consulting fees from AbbVie, Amgen, BMS, Corrona, Eli Lilly, Janssen, Myriad, Pfizer, Regeneron, Roche/Genentech, and UCB. EBL receives research grants from Amgen, and consulting fees from Novartis and Amgen. HY receives research grants from Pfizer and BMS. All other authors declare no conflicts of interest.
- Accepted for publication September 28, 2020.
- Copyright © 2021 by the Journal of Rheumatology
REFERENCES
DATA AVAILABILITY
The data that support the findings of this study are available from Centers for Medicare and Medicaid Services (CMS). However, the data are nonpublic and access to data files is restricted to users of the DUA under authorization of CMS.








{kind=link}
{kind=link}