

Abstract
Objective. Preliminary evidence suggests that ankylosing spondylitis (AS) is associated with an increased cardiovascular (CV) risk. We investigated subclinical atherosclerosis and arterial stiffness in patients with AS compared with controls, and identified CV and AS related risk factors for atherosclerotic disease.
Methods. A total of 59 patients with AS who were scheduled for etanercept treatment according to the ASsessments in Ankylosing Spondylitis guidelines and 30 healthy controls were recruited. Subclinical atherosclerosis was assessed as the average intima-media thickness (IMT) of the common carotid artery. Arterial stiffness was determined by distensibility, compliance, and Young’s elastic modulus of the carotid artery.
Results. AS patients had a greater IMT (0.62 ± 0.09 mm vs 0.57 ± 0.09 mm in controls; p = 0.02), a difference that remained after adjustment for traditional CV risk factors. AS was associated with higher carotid pulse pressure (47 ± 7 mm Hg vs 44 ± 8 mm Hg in controls; p = 0.04), but this was not due to local vessel wall properties. Among AS patients, age and body mass index (BMI) were determinants of IMT. Age, BMI, total cholesterol, triglycerides, and disease duration were identified as determinants of stiffness indices. No relationship was found between large-vessel properties and higher Bath AS disease indices or C-reactive protein values.
Conclusion. AS was associated with subclinical atherosclerosis and arterial stiffness, supporting epidemiological evidence of an increased CV risk in these patients. Whether these differences are due to AS or to a higher prevalence of CV risk factors in patients with AS remains to be determined.
Ankylosing spondylitis (AS), a chronic inflammatory disease of the sacroiliac joints and spine affecting up to 1% of the population, is associated with increased mortality rates1. Epidemiological studies have shown that this increased mortality is largely attributable to cardiovascular (CV) disease2–4. In a large sample of AS patients aged 50 to 75 years, we recently found that the prevalence of myocardial infarction is increased by about 2–3-fold compared with control subjects matched for age and sex5. Accelerated atherosclerosis in AS may be due to traditional CV risk factors, e.g., an atherogenic lipid profile and hypertension6,7. In addition, the generalized inflammatory state that characterizes active AS may render these patients more prone to develop CV disease8. Indeed, there is increasing evidence that the underlying inflammatory process in chronic inflammatory conditions resembles the chronic inflammatory processes that contribute to various stages of atherothrombosis, from early atheroma formation to plaque instability and thrombus formation9,10.
High-resolution ultrasonography can be used to measure the intima-media thickness (IMT) as well as vascular elasticity of the carotid artery. An increased carotid IMT reflects the atherosclerotic burden and predicts the development of (clinically apparent) CV disease in the general population11,12. Arterial stiffness is another important and independent risk factor for CV disease, partly due to its association with increased systolic blood pressure, ventricular mass, and decreased diastolic coronary perfusion13–16.
It is unknown whether AS patients without CV disease show early signs of large artery damage compared to controls, and if so, what the determinants of such large-vessel abnormalities are. This knowledge could prove useful for development of risk stratification and intervention strategies. Hence, this study was designed to determine whether signs of subclinical atherosclerosis and arterial stiffness are more prominent in a sample of AS patients compared to healthy controls, and to study determinants of these large-vessel characteristics.
MATERIALS AND METHODS
Study population
Eighty-two consecutive patients with AS attending the outpatient clinic of the Jan van Breemen Institute and VU University Medical Center, Amsterdam, and who were scheduled to receive etanercept treatment according to the ASAS (ASsessments in Ankylosing Spondylitis) guidelines for anti-tumor necrosis factor-α (anti-TNF-α) treatment were studied17. All patients fulfilled the modified New York diagnostic criteria for AS18. Thirty volunteers (patients’ friends or hospital staff) matched for age and sex served as controls. Patients and controls were excluded if a CV disease history was positive (myocardial infarction, percutaneous transluminal coronary angioplasty, surgery for ischemic heart disease, stroke, transient ischemic attack, carotid endarterectomy, peripheral arterial reconstructive surgery, or limb amputation). Patients and controls with diabetes mellitus (self-reported or when using glucose-lowering agents), hypertension (systolic blood pressure > 140 mm Hg, diastolic blood pressure > 90 mm Hg, or usage of antihypertensives), statin usage, anticoagulants, and/or low-dose aspirin usage were excluded. At conclusion of the protocol 59 of the 82 AS patients fulfilled the criteria. All participants gave written informed consent and the institutional ethics committees of the 2 hospitals approved the study protocol.
Other measurements
AS patients and controls attended the outpatient clinic at the Jan van Breemen Institute or VU University Medical Center, where they were examined by a research physician, and completed a questionnaire recording demographic data and medical and medication history. CV risk factors [current smoking (yes/no), blood pressure, body mass index (BMI), self-reported diabetes, and blood samples (for C-reactive protein [CRP], lipids)] were assessed in AS patients and controls. Height and weight were measured barefoot wearing light clothes only. The mean value of 2 measurements was used. BMI was calculated as the ratio of weight and height squared. Serum total cholesterol, high-density lipoprotein (HDL) cholesterol, and triglyceride levels were analyzed by enzymatic techniques as described19. The atherogenic index was calculated dividing total cholesterol levels by HDL cholesterol levels. AS-related variables that were assessed included the Bath AS Disease Activity Index (BASDAI)20, the Bath AS Functional Index (BASFI)21, and the AS mobility score [the Bath Ankylosing Spondylitis Metrology Index (BASMI)]22.
Arterial properties
Measurements were conducted in a quiet, temperature-controlled room after 15 minutes of rest, with the subjects in supine position. Subjects were asked to refrain from beverages other than water (in particular no caffeine or alcohol), smoking, and meals from midnight at the testing day. Brachial systolic and diastolic blood pressures and heart rate were assessed in the left upper arm at 5-minute intervals with an oscillo-metric device (Collin Press-Mate, BP-8800, Komaki City, Japan). Brachial pulse pressure (PP) was calculated as systolic minus diastolic blood pressure, and brachial mean arterial pressure (MAP) as (2 diastolic pressure + systolic pressure)/3.
Ultrasound analysis of the right common carotid artery and the right brachial artery was performed by 2 observers who were unaware of the participants’ clinical or laboratory characteristics. Measurements were performed with a 7.5-MHz linear probe connected to a computer equipped with vessel wall movement detection software and an acquisition system (Wall track system, Pie Medical, Maastricht, The Netherlands), which enables measurement of the IMT, diameter, and distension. The distance between the lumen-intima interface and the leading edge of the media-adventitia interface of the far wall corresponds with IMT. After localization of the common carotid artery, cross-sectional measurements were performed 10 mm proximal from the carotid bulb. Sites with mural atherosclerotic plaque were excluded while measuring. We defined plaques as focal widening of the vessel wall of 50% relative to adjacent segments with protrusion into the lumen. The protrusion was evaluated by a visual judgment23. The mean IMT, diameter, and distension of 3 consecutive measurements were used for the analyses. Carotid PP was determined according to the method from Van Bortel and coworkers24. Carotid diameter (D), distension (ΔD), carotid PP (ΔP), and IMT were used to calculate different arterial stiffness indices, as follows25:
The interobserver variability [CV = (standard deviation of the mean difference/√ 2)/pooled mean] for the studied measurements were IMT, 7%; carotid diameter, 2%; and carotid distension, 7%. The corresponding values for the intraobserver variability were, for observer 1 and 2, respectively: IMT, 6% and 7%; carotid diameter, 2% and 2%; and carotid distension, 6% and 9%.
Statistical analyses
Data are expressed as mean (SD) or median (interquartile range) as appropriate. Differences in demographic variables, CV risk factors, and arterial wall properties between AS patients and controls were investigated using Student T tests, Mann-Whitney U tests, and Pearson chi-square tests, when appropriate. Univariate and multivariate linear regression models were conducted to investigate differences in arterial wall properties between AS patients and controls. Multivariate models were conducted according to a forward selection procedure, introducing variables that showed a significant association with the outcome measure (p < 0.10). Variables entered into the multivariate models were age, sex, pulse pressure, heart rate, CRP, smoking, and the atherogenic index. Pulse pressure was replaced by MAP if the outcome measure was one of the arterial stiffness indices. As carotid stiffness indices (i.e., carotid distensibility, compliance, and elastic modulus) were not normally distributed, data were analyzed with the logarithms (natural) of these values and the regression coefficients and confidence intervals were presented using these values. Among AS patients, we investigated the relationship between arterial wall properties and CV and AS risk factors with Pearson correlations or Spearman rho tests when appropriate. A 2-tailed probability value of p < 0.05 was considered statistically significant.
RESULTS
Patients with AS
Table 1 summarizes the baseline characteristics of all AS patients; their median age was 39 years and 63% were male. Most AS patients were HLA-B27-positive (88%), median AS disease duration was 9 years; BASDAI disease activity score was 6.2, which represents high disease activity. All AS patients were currently being treated with nonsteroidal antiinflammatory drugs (NSAID).
Baseline characteristics of AS patients and controls.
AS patients compared to controls. CVD risk profile
AS patients smoked more often, and had slightly higher systolic blood pressure and lower diastolic blood pressure, resulting in a significantly higher pulse pressure (Table 1). CRP was significantly higher in AS patients. No significant differences were observed for total cholesterol, HDL cholesterol, atherogenic index, triglycerides, and BMI.
Carotid arterial wall properties
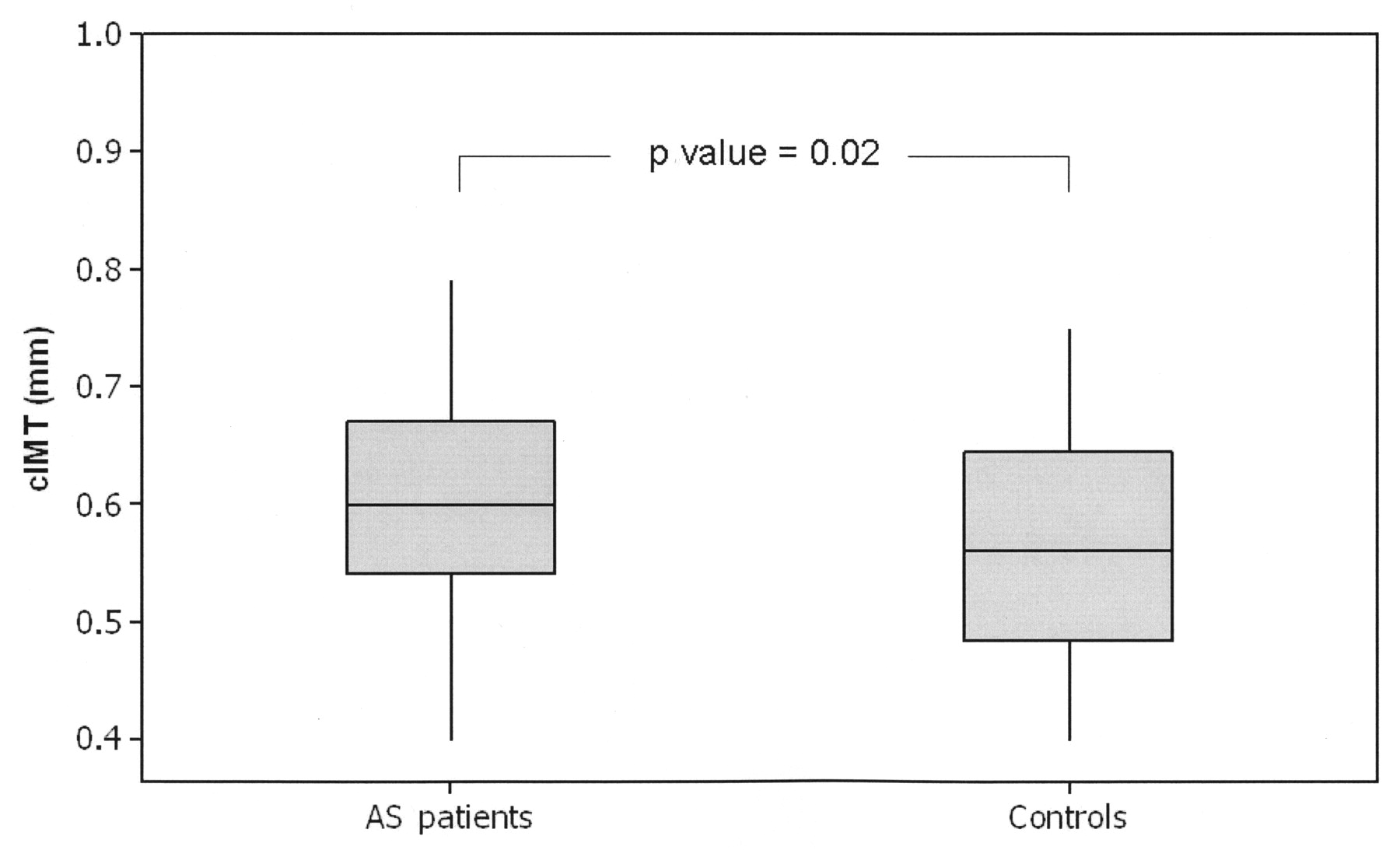
Table 1 shows all carotid arterial wall properties in AS patients compared with controls. AS patients had increased IMT (0.62 mm in patients vs 0.57 mm in controls; p = 0.02; Figure 1). This difference remained when linear regression analyses were done adjusting for potential confounders (Table 2). In conjunction with a higher brachial pulse pressure, the carotid pulse pressure was significantly higher in AS patients (47 ± 7 mm Hg vs 44 ± 8 mm Hg, respectively; p = 0.04). This difference decreased after adjustment for traditional CV risk factors, but remained statistically significant (Table 2). No significant differences were observed for local wall properties reflecting arterial stiffness, including carotid distensibility, compliance, and elastic modulus.

Carotid intima-media thickness: AS patients, 0.62 mm; controls, 0.57 mm (p = 0.02).
Arterial wall properties in AS patients relative to controls.
Relationships of IMT, arterial stiffness, and CV and AS-related risk factors
In AS patients, IMT was correlated with age (r = 0.392, p = 0.002) and BMI (r = 0.288, p = 0.03). IMT did not correlate with AS-related risk factors reflecting current disease activity, i.e., BASDAI and CRP, or with AS-related risk factors reflecting an increased disease burden, i.e., BASFI, BASMI, and disease duration. Subgroup analysis comparing AS patients with CRP levels > 10 mg/l to those with normal CRP levels also revealed no differences in IMT or arterial stiffness indices (data not shown). In addition, no correlations were observed for carotid pulse pressure with either traditional or AS-related risk factors. Arterial stiffness by means of carotid distensibility was correlated with age (r = −0.666, p < 0.001), total cholesterol (r = −0.522, p < 0.001), triglycerides (r = −0.416, p = 0.001), and BMI (r = −0.284, p = 0.03). In agreement with IMT, arterial stiffness did not correlate with AS-related risk factors (CRP, BASDAI, BASFI, and BASMI), except for disease duration (r = −0.362, p = 0.005). Similar correlations were found for the compliance and the elastic modulus (data not shown).
DISCUSSION
There is considerable interest in the association between chronic inflammatory diseases and CV disease, but the current evidence base for a link between AS and CV disease is limited. Our study reveals a higher CV risk among AS patients as indicated by a greater IMT and brachial and carotid pulse pressure in comparison with controls, but this was not reflected by impaired arterial stiffness indices. These observations support epidemiological findings indicating that AS may be associated with an increased CV risk, although further prospective studies are needed to appraise the clinical relevance of a 0.05 mm carotid IMT difference5,26. In addition, we observed a high CV risk factor profile in patients with AS, and some of these risk factors (lipids and BMI) were associated with a greater carotid IMT and increased arterial stiffness.
Four studies assessing IMT in AS patients and controls have been published27–30. All studies found a nonsignificant trend toward a greater IMT in AS patients, but none of these studies selected AS patients with an active disease as part of the study protocol. Given that inflammation has increasingly been acknowledged as the reason rheumatic patients bear elevated CV risk31, we selected patients with an active disease, represented by a BASDAI > 4 at inclusion and insufficient response to NSAID32–34. However, in our cohort we found no association between large-vessel properties and higher Bath AS indices or CRP values. Several reasons could potentially explain this. First, the cross-sectional study design does not permit a good estimate of the cumulative inflammatory burden. Second, all patients included in the study had high disease activity, which may have diminished the potential to observe such an association by selecting a potentially more homogeneous population than would be seen clinically. However, this argument is unlikely to be applicable to the CRP marker, for which values varied widely among patients with AS. Hence, the inflammatory hypothesis may perhaps apply to AS to a lesser extent than to these other rheumatic diseases. Of note, CRP levels, although several times higher than in controls, are considerably lower in AS patients than in patients with other rheumatic diseases, such as rheumatoid arthritis and psoriatic arthritis. Third, somewhat paradoxically, despite stringent inclusion criteria used in this study, clinical heterogeneity of patients may also have been too great. For instance, patients with active disease and high BASMI values may have had limited spinal mobility due to pain/inflammation rather than advanced radiological damage35. In all, the lack of an association between inflammatory mediators and arterial wall properties does not, per se, exclude the possibility that the chronic inflammatory burden is atherogenic, and further studies are needed to address this association.
These results suggest that an adverse CV risk profile may cause, at least partly, the greater IMT and higher pulse pressure in patients with AS. Indeed, BMI and total cholesterol and triglycerides have been positively correlated with IMT and/or arterial stiffness7,29. In conjunction with this, 23 of the consecutive 82 screened AS patients (28%) were excluded from the analyses because of prior CV disease or other important CV risk factors. These observations are in accord with the findings of others26,29 and may imply that CV risk factors have more influence on the CV system than AS itself, and they underline the importance of proper CV management36.
Interestingly, despite a higher carotid pulse pressure in AS, carotid vessel wall properties did not differ between AS patients and controls. Apparently, other segments of the arterial tree are responsible for the increased pulse pressure, although a role for increased stroke volume/contractility cannot be fully excluded. An impaired aortic compliance may be responsible for the higher pulse pressure as this is the arterial segment that predominantly affects pulse pressure throughout the arterial tree37. However, to date, no studies have been published on aortic compliance in AS, and our findings illustrate the necessity to perform such studies. Whatever the cause, our observations are important as higher pulse pressure itself translates into higher CV risk38.
Interpretation of our findings needs to be cautious, as all observations are cross-sectional and do not provide definitive evidence for causality or directionality. In addition, a single-point measurement technique was used to determine arterial properties, i.e., IMT, diameter, and distension, and this may have influenced our results due to variability of these characteristics along the arterial segment. However, we minimized measurement variability by clearly defining where IMT had to be determined. Further, methodological blinding to case-control status of participants was impossible, because some patients had AS-specific deformities. It should also be noted that a large proportion (~50%) of the AS patients smoked, which may have caused bias towards the null hypothesis. However, multivariable adjustment should account for such bias. Moreover, when patients and controls that smoked were excluded from the comparison analysis, the age and gender-matched IMT difference remained. In agreement, all correlations between arterial wall properties and risk factors remained when patients that smoked were excluded. All AS patients were treated with stable doses of NSAID and this may be a potential confounder explaining the observed differences in IMT and arterial stiffness39. To clarify the CV effects of inflammation and NSAID, one might compare patients with noninflammatory back pain using NSAID with AS patients in future studies. The fact that controls had a significantly lower heart rate, which may reflect more physical activity and lower smoking prevalence, may indicate that this group had a lifestyle more conducive to cardiovascular health. Finally, since AS patients included in the study were highly selected, we cannot necessarily conclude that AS patients with a lower disease activity do have changes in arterial wall properties similar to those we observed.
Our observations indicate that AS is associated with early signs of preclinical atherosclerosis, but future larger (prospective) studies are needed to confirm our findings and to investigate which factors contribute to these arterial perturbations.
Acknowledgments
We thank Ingrid Knufman for her contribution to the arterial wall measurements and Prof. Nico Westerhof for critical reading of the manuscript.
Footnotes
-
The Jan van Breemen Institute receives financial support from the Dutch Arthritis Association. The Dutch Arthritis Foundation financially supported this study.
- Accepted for publication August 7, 2009.








{kind=link}