Article Text

Abstract
Objective The cross-immunogenicity of the recently approved infliximab-biosimilar Remsima (CT-P13) with the originator drug Remicade is still unknown.
Design Sera of patients with IBD with or without measurable anti-Remicade antibodies to infliximab (ATI) were tested for their cross-reactivity to two batches of Remsima. Experiments were repeated after deglycosylation of Remicade/Remsima, IgG purification, excipients’ dialysis and monomer purification by size exclusion chromatography. Anti-Remicade antibodies were tested for their functional inhibition of TNF-α binding by Remsima/Remicade by competition assay. Cross-reactivity of anti-adalimumab antibodies with Remicade/Remsima was also investigated.
Results 125 patients’ and controls’ sera were tested (median age 31 years, IQR 24.5–39.5). All 56 anti-Remicade ATI-negative controls (14 healthy individuals, 42 patients with IBD) were also negative for anti-Remsima ATI. All 69 positive anti-Remicade IBD sera were cross-reactive with Remsima. ATI titres against Remicade or Remsima were strongly correlated (r values between 0.92 and 0.99, p<0.001 for all experiments, Spearman's correlation test). The background ELISA signal for Remsima was slightly higher compared with Remicade in negative controls (1.25±0.6 µg/mL vs 0.76±0.5 µg/mL, respectively, p<0.001), and persisted after deglycosylation, dialysis or protein size filtration, but abolished by IgG purification and significantly diminished by monomer purification. Anti-Remicade ATIs of patients with IBD (n=10) exerted similar functional inhibition on Remsima or Remicade TNF-α binding capacity (p=NS for all inhibition curve points). Antibodies-to-adalimumab in adalimumab-treated patients with IBD (n=7) did not cross-react with either Remicade or Remsima.
Conclusions Anti-Remicade antibodies in patients with IBD recognise and functionally inhibit Remsima to a similar degree, suggesting similar immunogenicity and shared immunodominant epitopes on these two infliximab agents. In contrast, anti-adalimumab antibodies do not cross-react with Remsima or Remicade.
- IBD CLINICAL
- IMMUNOTHERAPY
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
The infliximab biosimilar Remsima (CT-P13) has recently been approved for use in Europe across all indications.
Antidrug antibodies can lead to infusion reactions and/or loss of response.
The cross-immunogenicity of Remicade and Remsima has not been explored yet.
What are the new findings?
Antibodies to Remicade in patients with IBD similarly recognise and cross-react with Remsima.
The background signal in unexposed patients is slightly higher to Remsima compared with Remicade, possibly owing to minute difference in aggregate content, but is unrelated to any difference in glycosylation.
Antibodies to Remicade similarly neutralise TNF binding of Remsima and Remicade.
Antibodies to adalimumab do not cross-react with either Remicade or Remsima.
How might it impact on clinical practice in the foreseeable future?
The cross-reactivity of Remsima and Remicade suggests similar immunodominant epitopes and immunogenic potential of the two agents.
Patients with IBD who develop high-titre antibodies and infusion reaction/loss of response to Remicade should probably not be considered for switching to Remsima.
In contrast, patients who develop anti-adalimumab antibodies may be considered for a switch to either Remicade or Remsima, if clinically indicated.
Assays for measuring immunogenicity of biosimilars may not be entirely identical to originators’ assays but need to be adapted based on cross-immunogenicity and background signal validation.
Pharmacovigilance studies of Remsima with longitudinal immunogenicity monitoring are pertinent.
Introduction
Infliximab is an antitumour necrosis factor α (anti-TNF-α) chimerical monoclonal IgG1 antibody with proven efficacy in IBD,1 ,2 as well as in other immune inflammatory disorders such as rheumatoid arthritis (RA), psoriasis and ankylosing spondylitis (AS). The originator drug, distributed under the trade name of Remicade, has been tested and approved separately for all these indications. Recently, an infliximab biosimilar was introduced under the trade name Remsima (Developmental name CT-P13, produced by Celltrion, South Korea, and also distributed by Hospira, USA under the trade name Inflectra).3 Following extensive biocompatibility assays and similar pharmacokinetic profile and clinical efficacy in two head-to-head trials in RA and AS,4 ,5 Remsima was recently approved for use by the European Medicinal Agency also in patients with IBD by extrapolation of indications.6 A decision by the US Food and Drug Administration (FDA) regulatory agency is still awaited. However, the decision by the European Medicinal Agency has already stirred a debate pertaining to the ability to extrapolate clinical efficacy across indications and the safety of a biosimilar, in particular with respect to its potential immunogenicity.7–9
Virtually all biologic monoclonal antibodies (mAbs) are immunogenic, that is, can elicit antidrug antibodies in some recipients. Antibodies to infliximab (ATI) have been associated with accelerated drug clearance, reduced drug efficacy and higher risk of infusion reactions.10–12 As such, ensuring immunogenicity equivalence between an innovator biologic and its biosimilar is a major cause for concern.7 ,8 Although the rates of antidrug antibodies to Remsima and Remicade were similar in the RA and AS studies,4 ,5 there are still no direct data pertaining to cross-immunogenicity of Remicade and Remsima, particularly in patients with IBD.
Therefore, the aim of the present study was to investigate the immunogenic comparability between Remicade and Remsima by examining if antibodies elicited by Remicade treatment in patients with IBD also cross-react and recognise Remsima to a similar degree.
Methods
Study population
Patients with IBD treated at the Gastroenterology Department of the Sheba Medical Center were included. IBD was diagnosed by the combination of established clinical, radiological, endoscopic and histological criteria. The sera of patients treated with infliximab (Remicade, Janssen Biotech, Horsham, Pennsylvania, USA) as well as sera of patients with IBD not treated by anti-TNF-α biologics and sera of healthy individuals were used for this study. For infliximab treated patients, sera were obtained before the next infusion and trough level of the drug and antidrug antibodies were determined by anti-λ ELISA (see below). Patients and healthy volunteers gave written informed consent.
Measurement of ATI cross-reactivity with Remicade and Remsima
To assess whether anti-Remicade ATI from Remicade-treated patients with IBD cross-react with Remsima, the titre of anti-Remsima ATI was measured in anti-Remicade ATI-positive sera obtained from Remicade-treated patients. Negative controls (ATI-negative) consisted of patients with IBD unexposed to infliximab, patients with IBD receiving infliximab without detectable ATI and healthy individuals. ATI were determined by the antihuman λ chain ELISA, which is capable of detecting ATIs also in the presence of the drug, as previously described.13 ,14 Briefly, infliximab (0.1 mg/mL) was added to preplated TNF-α (500 ng/mL) in 100 µL wells of ELISA plates (Nunc, Roskilde, Denmark). In all experiments, infliximab-Remicade (Janssen, USA) and infliximab-Remsima (Celltrion, Incheon, South Korea) were used in the ELISA plate wells side-by-side for the purpose of comparison. After drying, 100 µL of serum was added and incubated for 90 min at room temperature. Plates were then washed and goat antihuman λ chain horseradish peroxidase-labelled antibody (Serotec, Oxford, UK) was added at a dilution of 2.5×104 for 60 min and reacted with tetramethylbenzidine substrate. The results were read by an ELISA reader EL-800 (Biotek Instruments, Winooski, USA) and expressed as mcg/ml after normalisation versus results obtained using additions of graded concentrations between 9 ng/mL and 600 ng/mL of horseradish peroxidase labelled goat antihuman F(ab’)2 fragment antibody (MP Biomedicals). The assay’s cut-off level of detection for anti-Remicade ATI is 2.5 µg/mL. Antibodies to adalimumab (ATA) were similarly measured after plating the wells with adalimumab (AbbVie, USA) at a similar concentration as above.
Functional inhibition of Remicade/Remsima TNF-α binding capacity
An inhibition assay was performed to compare whether anti-Remicade ATI elicited in Remicade-treated patients inhibited to similar extent Remicade and Remsima TNF-α binding capacity. For this purpose, five anti-Remicade ATI-positive IBD sera and five anti-Remicade ATI-negative sera were tested. Sera were diluted 1:20 in bovine serum albumin (BSA), preincubated with the designated graded concentrations of exogenous Remicade or Remsima for 30 min at room temperature, and then added to preplated TNF-α ELISA plates. The concentration of the bound infliximab (Remicade or Remsima) was then measured as previously described.13 ,14
Deglycosylation experiment
To investigate if the glycosylation pattern of the IgG mAb agents impacts cross-immunogenicity, deglycosylation of Remsima and Remicade was performed. Briefly, 100 µg each of Remsima and Remicade (determined by BCA kit, ThermoScientific, Illinois, USA) were subjected to deglycosylation using Protein Deglycosylation Mix kit (New-England BioLabs Ipswich, Massachusetts, USA), employed according to manufacturer's instructions. One hundred micrograms of untreated and treated protein were subsequently used in the ATI-ELISA as above. Completeness of deglycosylation was assessed by native gel electrophoresis. To this end, a 50 µL sample buffer of native gel was added, and 30 µg of protein were loaded on native precast 7.5% gels (mini protein TGX gels, BIO-RAD, Germany). Control protein was BSA (66 kDa, Sigma, USA). The gels were allowed to run for 6 h at 0.5 mA 100 V with native running buffer Tris/Glycine (BIO-RAD, Germany), stained with SeeBand (Gene Bio-Application, Israel).
IgG purification by protein G column
Protein G column purification was performed after the designated mAbs were brought to the concentration of 1.5 mg/mL with binding buffer. Protein G bead purification of IgG was accomplished with a commercial kit according to manufacturer's instructions (NAb Spin Kit, cat. No. 89949, ThermoScintific, Illinois, USA). After elution, protein concentration was determined with BCA kit (ThermoScintific, Illinois, USA)
Dialysis and protein size filtration experiments
Remicade and Remsima at 13.5 mg in 0.5 mL of phosphate buffered saline (PBS) (sigma, USA) were loaded into a dialysis tube (midi GeBaflex-tube, Gene Bio-Application, Israel) with a molecular weight cut-off of 3.5 KD (kilodalton) and were immersed in PBS which was changed three times during 24 h at 4°C with stirring. The concentration of the protein was then determined with a BCA kit (ThermoScintific, Illinois, USA). Size filtrations for 30 KD and 100 KD subfragments were performed for Remicade and Remsima after addition of 13.5 mg protein in 0.5 mL of PBS (Sigma, USA) to a centrifugal filter device Microcon YM-30 or YM-100 (Amicon, Millipore, USA), which was spun at 14 000 g for 12 min at 25°C. After retention of the sample, protein concentration was determined with a BCA kit and used for ELISA as previously described above.
Size exclusion chromatography
Remicade and Remsima IgGs were purified by preparative size exclusion chromatography (SEC) using a Sephacryl 26/60 S200 (GE Healthcare) 320 mL column. Twenty micrograms of each antibody were injected in a volume of 1 mL into the loading loop of an Äkta-FPLC machine (GE Healthcare) that was developed using PBS as the running buffer at 1.0 mL/min. Ten micro litre fractions were collected. Protein content was determined and the monomer fraction was used for ELISA as described above.
Statistical analysis
Continuous variables were tested for normality by Shapiro-Wilk test and Q-Q plots, and analysed by paired two-tailed t test or Wilcoxon test, for normally and non-normally distributed paired measurements, respectively. Categorical variables were analysed by Fisher’s exact test. Correlation coefficients were determined by Spearman's correlation test. All statistics were carried out using MedCalc software (Mariakerke, Belgium). A two-tailed p<0.05 was considered statistically significant.
Results
Cross-reactivity of anti-Remicade ATI with Remsima
Overall, 108 patients and healthy individuals participated in the study and 125 sera were tested for Anti-Remicade ATI cross-reactivity to Remsima (17 patients had sera obtained at two different time points). The clinical characteristics of these 108 patients and controls are depicted in table 1. None of the subjects was ever exposed to Remsima.
Clinical characteristics of the study population
In a first experiment, 30 anti-Remicade ATI-positive sera of Remicade-treated patients with IBD as well as 12 negative control sera were tested to examine whether ATIs elicited to Remicade will cross-react with Remsima. All 30 sera of Remicade-sensitised patients with IBD containing anti-Remicade ATIs were cross-reactive with Remsima. Moreover, when tested against two different Remicade batches, there was excellent correlation between anti-Remsima and anti-Remicade ATI titres (r≥0.98, 95% CI 0.97 to 0.99, p<0.001 for both the comparisons, Spearman's correlation test, figure 1A, B). The correlation between anti-Remsima and anti-Remicade ATI was not different from the correlation between two ATIs towards two different batches of Remicade themselves (r=0.99, 95% CI 0.97 to 0.99, p<0.001 figure 1C).

(A–C). Dot plots of correlations between anti-Remsima antibodies-to-infliximab (ATI) levels and anti-Remicade ATI levels in ATI-negative and ATI-positive sera (n=42). Cross-reactivity with two Remicade batches is depicted and each marker denotes the level obtained for a single serum. (D) Anti-Remicade/anti-Remsima ATI in negative ATI controls and in patients with positive anti-Remicade ATI (n=83) as measured towards the two designated Remicade batches and the two Remsima batches. Each marker denotes the result obtained for a single serum sample. The p value denotes differences between Remicade and Remsima batches collectively.
In a second validation experiment, a larger group of patients with IBD and controls (n=83) was tested, this time employing two different batches of Remsima (along with two different batches of Remicade) and larger percentage of negative control sera. All sera (n=41) with positive anti-Remicade ATI were cross-reactive with the two Remsima batches and all anti-Remicade ATI negative sera (n=42) were also negative for anti-Remsima ATIs (figure 1D). The mean titres of anti-Remsima and anti-Remicade ATI in sera of patients who were anti-Remicade positive were similar (p=NS (non-significant value) for all comparisons, table 2). The mean ATI titres in sera of patients who were anti-Remicade negative were significantly lower than ATI in anti-Remicade positive patients, although the negative background signal obtained towards Remsima was slightly but significantly higher than towards Remicade (figure 1D and table 2). Nonetheless, there was still a robust correlation between the ATI titres measured towards the four different Remicade/Remsima batches (r values ≥0.92, p<0.001 for all tests, Spearman's correlation test, online supplementary figures S1a–f).
Mean±SD of ATI levels measured towards two different Remicade and two different Remsima batches in anti-Remicade ATI-negative sera (n=42) and ATI-positive sera (n=39)
Similar results were also obtained when testing ATI-negative sera from patients with transient anti-Remicade ATI (n=11). Specifically, testing for anti-Remicade and anti-Remsima ATI in the second ATI-negative serum following a single previous ATI-positive serum in patients with transient ATI, showed a slight but statistically significant difference in ATI-negative sera signal intensity between Remicade and Remsima (0.71±0.5 µg/mL vs 1.22±0.94 µg/mL, respectively, p=0.02, Wilcoxon rank-sum test, online supplementary figure S2). However, the negative anti-Remsima ATI titres were not different from the negative values obtained in ‘genuine’ unexposed ATI-negative controls (n=44, 1.22±0.94 vs 1.37±0.63, respectively, p=0.63).
Effects of deglycosylation, IgG purification and removal of excipients on background ELISA signal to Remicade/Remsima
To explore whether the slightly higher background signal in ATI-negative sera when tested against Remsima compared with Remicade is related to differences in glycosylation pattern, both mAbs were subjected to deglycosylation using a commercially available protein deglycosylation kit (see Methods section). As shown in figure 2A, a native gel electrophoresis verified the complete deglycosylation of Remicade and Remsima. ATI-negative sera (n=25), as well as a small sample of positive ATI controls (n=3), were then tested for ATI level towards the native Remicade or Remsima compared with the ATI level towards their corresponding deglycosylated forms. Similar to the previous experiments, the background signal obtained for ATI-negative sera was once more slightly but significantly different between Remicade and Remsima (1.55±5.1 µg/mL vs 1.97±5.5µg/mL, respectively, p<0.0001, Wilcoxon rank-sum test). For Remicade and Remsima, deglycosylation slightly increased the level of the background signal compared with the untreated protein. However, the difference in background signal between Remicade and Remsima remained unchanged after deglycosylation (2.43±5.2 µg/mL vs 2.96±5.5 µg/mL, respectively, p<0.001, Wilcoxon rank-sum test, figure 2B). In three positive ATI sera there was no difference between Remicade and Remsima before or after deglycosylation (results not shown).
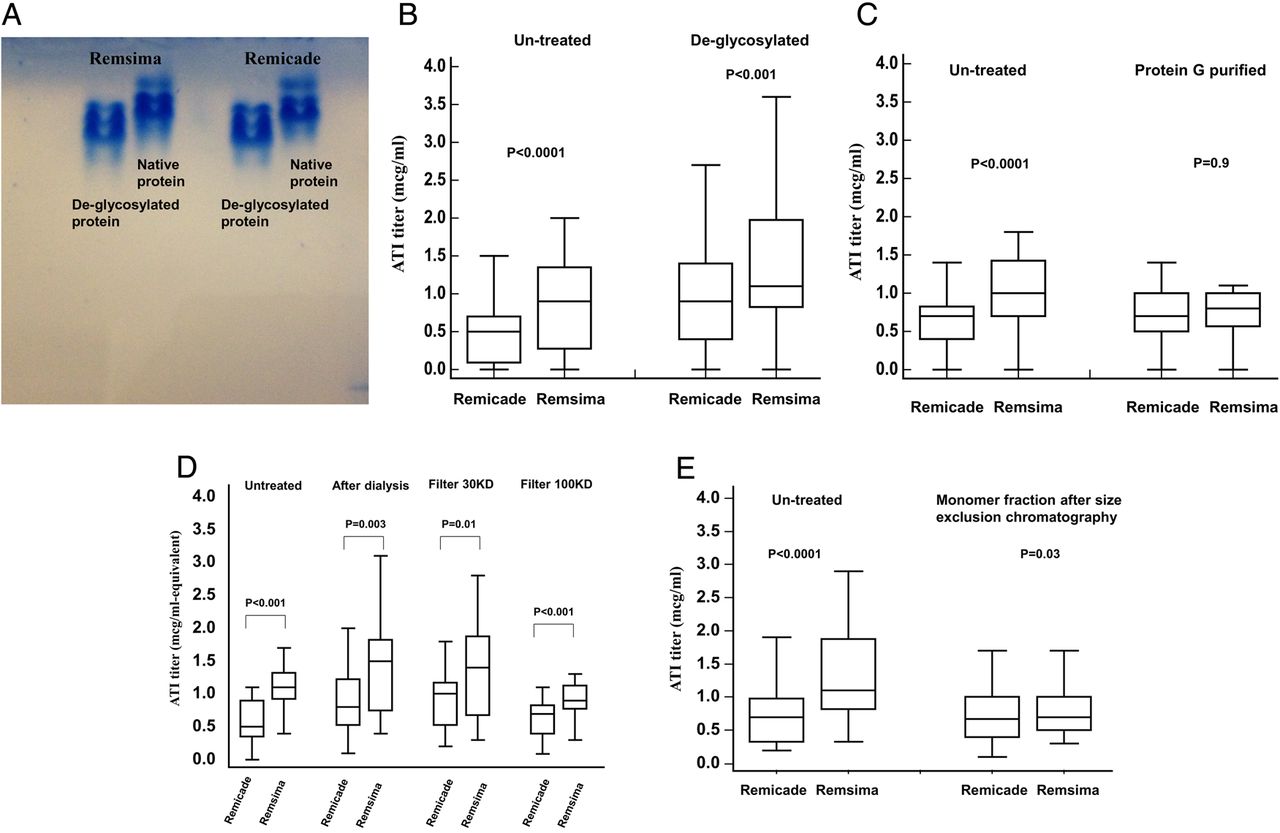
(A)Native gel electrophoresis of Remicade or Remsima before and after deglycosylation. (B) Deglycosylation does not abolish the difference between Remicade and Remsima in the background ELISA signal in negative antibodies-to-infliximab (ATI) controls. Box-and-whisker diagrams are shown for ATI level measured towards untreated proteins and deglycosylated proteins in ATI-negative patients (n=25). (C) Protein G purification of IgG abolishes the difference between Remicade and Remsima in the background ELISA signal in negative ATI controls. Box-and-whisker diagrams are shown for ATI level measured towards untreated proteins and protein G purified proteins in ATI-negative patients (n=20). (D) Dialysis and size filtration do not alter the difference between Remicade and Remsima in the background ELISA signal in negative ATI controls. Box-and-whisker diagrams are shown for ATI level measured towards the untreated and treated proteins in ATI negative patients (n=12). (E) Monomer purification by size exclusion chromatography diminishes and nearly abolishes the Remicade-Remsima difference in the background ELISA signal. Box-and-whisker diagrams are shown for ATI level measured towards untreated proteins and towards monomeric fractions thereof, in ATI-negative patients (n=27).
To examine if differences between the Remsima/Remicade IgG molecules themselves were responsible for this slight difference in background signal, we then assessed ATIs towards purified IgG molecules of Remsima and Remicade, after binding and elution over a protein G column. Interestingly, the difference between background signal for Remsima/Remicade disappeared when control ATI-negative sera were tested against the purified IgG mAb of Remicade and Remsima (0.79±0.43 mcg/ml vs 0.78±0.37 mcg/ml, respectively, p=0.8, paired t test, n=20, figure 2C).
In further experiments, the removal of excipients by subjecting Remicade/Remsima to dialysis with 3.5 KD filter before the measurement of ATI, or the removal of subprotein fragments by size filtration with either a 30 KD filter or a 100 KD filter did not abolish the slight difference in background signal between the two mAbs (figure 2D).
We next sought to examine whether IgG aggregates may be responsible for the slight difference in the background signal. To this end, SEC was performed to purify monomeric forms of Remsima and Remicade. Subsequently, these IgG monomers were used to detect ATIs by similar ELISA as above in ATI-negative controls (n=27) and ATI-positive patients (n=5). As shown in figure 2E, the difference between Remicade and Remsima background signal was again slight yet significant (0.68±0.42 µg/mL vs 1.29±0.64 µg/mL for Remicade and Remsima, respectively, p<0.0001), but was nearly completely abolished when monomers were tested (0.74±0.47 µg/mL vs 0.82±0.45 µg/mL for Remicade and Remsima monomers, respectively, p=0.03). The signal in ATI-positive sera was unaltered after SEC (data not shown).
Functional inhibition of Remicade/Remsima TNF-α binding by anti-Remicade antibodies
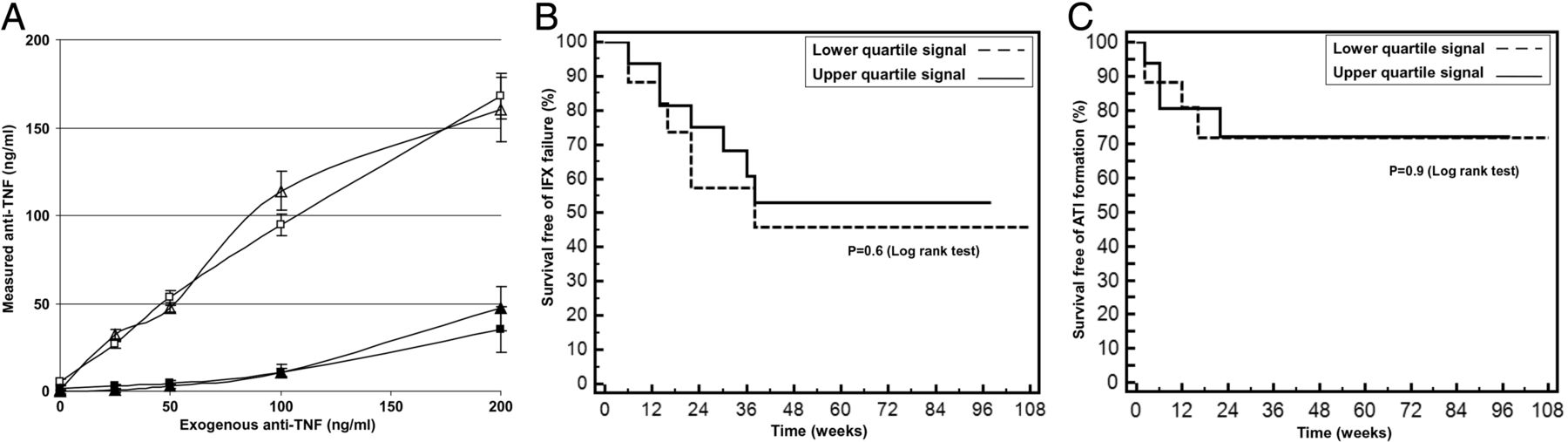
To investigate if anti-Remicade ATIs formed in Remicade-treated patients with IBD can functionally inhibit to similar extent the binding of Remsima or Remicade to their target TNF-α, 10 sera were tested in a binding-inhibition assay (5 anti-Remicade ATI-positive and 5 anti-Remicade ATI-negative). As shown, anti-Remicade positive sera (filled markers) inhibited Remicade and Remsima TNF-α binding to similar extent. Conversely, anti-Remicade ATI-negative sera (hollow markers) had no inhibitory effect on Remicade or Remsima TNF-α binding capacity (figure 3A).
{kind=link}
{kind=link}
{kind=link}
(A) Remicade and Remsima TNF-α binding capacity is similarly inhibited by anti-Remicade antibodies to infliximab (ATI)-positive sera and unaffected by ATI-negative sera. Shown are bound TNF-α Remicade/Remsima at the designated graded exogenous concentrations, as measured after preincubation with anti-Remicade ATI-positive sera (filled markers) or ATI-negative sera (hollow markers). (B) Kaplan-Meier curve depicting survival without clinical failure of Remicade in patients with IBD whose pretreatment ELISA background signal was in the upper quartile (n=17) on the negative ATI range versus those in the lower quartile (n=17). (C) Kaplan-Meier curve depicting survival without formation of anti-Remicade ATIs in patients with IBD with upper versus lower quartile of pretreatment ATI background ELISA signal (n=17 in each quartile).
To gain some further insight on the functional significance of the slight differences in background signal to Remicade and Remsima in patients never exposed to either drug, we examined the impact of differing pre-exposure background ELISA signal in patients with IBD starting infliximab treatment. To this end, a cohort of 68 patients with IBD who had pretreatment sera available before they commenced Remicade therapy was investigated. Patients in whom the pretreatment ATI signal was in the upper quartile of the negative ATI range were compared with those in the lower quartile of the negative ATI signal with respect to subsequent clinical failure (no and/or loss of response) of Remicade and to formation of ATI during treatment. As shown in figures 3B, C, there was no clinical or immunogenic difference in response to Remicade in patients with high versus low pretreatment background signal to Remicade. Similar results were obtained when the comparison was performed for patients with pretreatment background signal to Remicade above or below the median negative ATI value (data not shown).
Cross-reactivity between adalimumab and Remicade/Remsima
To investigate if anti-adalimumab antibodies cross-react with Remsima, eight positive ATA sera of adalimumab-treated patients with IBD (seven never exposed to Remicade, one with prior failure of Remicade with positive anti-Remicade ATI) were tested in parallel for their cross-reactivity against two Remicade and two Remsima batches. The results showed that in all seven ATA-positive sera there was no detectable anti-Remicade or anti-Remsima cross-reacting antibodies (read-outs below 2.5 µg/mL detection level in all sera, table 3). In contrast, the positive control ATA-positive serum which was also ATI-positive after prior exposure to Remicade, exhibited detectable anti-Remicade and anti-Remsima antibodies (serum 3754).
Results of cross-reactivity by ATI levels for seven anti-adalimumab positive sera of patients with IBD unexposed to Remicade as measured towards two batches each of Remsima and Remicade
Discussion
The advent of biosimilars into the IBD arena is likely an inevitable step, and may also possibly benefit patients by facilitating easier and earlier access to biologic treatments through reduced drug costs.3 ,9 ,15 Notwithstanding, although the infliximab biosimilar Remsima has been extensively tested and validated to be comparable to the bio-originator Remicade in rheumatological diseases, there is still an ongoing debate regarding its use in IBD. Much of the debate is stirred by questions pertaining to safety issues and to concerns about the bioequivalence of Remsima with respect to immunogenicity potential and possible immunogenic adverse events.7 ,8 ,15 ,16
In the present study, we examined the cross-immunosensitisation to Remicade and Remsima in patients with IBD. The findings indicate that in all patients with IBD who developed anti-Remicade antibodies after prior exposure to Remicade, these antibodies were also cross-reactive with Remsima. Moreover, the titre of the antibodies was strikingly similar whether gauged with Remicade or Remsima as the target antigen and was also comparable when using several batches of the drugs (figure 1A–D and table 2). Importantly, functional assays showed similar capacity of these ATIs to inhibit TNF binding by either Remicade or Remsima, further suggesting a similar affinity of anti-Remicade antibodies to Remsima. Taken together, these data strongly support a similar immunogenic profile for Remicade and Remsima, probably due to shared common immunodominant epitopes on these two infliximab agents. The consequent clinical implications are that switching between Remicade/Remsima in patients who developed high-titre ATI and an infusion reaction and/or loss of response to one of these agents, is probably unwarranted, as the likelihood of immune reactivity to the second agent is very high. In contrast, these data may indicate that switching ATI-negative patients between these two agents may not confer an increased risk for evoking immunogenicity, but clinical studies will be needed before this practice can be routinely endorsed.
A slight but statistically significant difference in the ELISA background signal was observed when control ATI-negative sera were tested against Remicade or Remsima. The cause for this slight difference is probably unrelated to different glycosylation patterns of the two molecules, since the difference remained unchanged even after stripping both proteins off their glycosylation by deglycosylation (figure 2A, B). Removal of drug excipients by dialysis and of subprotein fragments by size filtering did not affect the background signal as well. However, the difference in the background signal disappeared when ATI-negative sera were tested against pure IgG molecules of Remsima and Remicade after they were bound and eluted by protein G columns (figure 2C), suggesting the slight background reactivity is unrelated to the IgG molecule itself. Testing of three batches of Remsima versus three batches of Remicade by SEC-high performance liquid chromatography (HPLC) and SEC-multi-angle laser light scattering (MALS) showed near-identical monomer content, with 99.8–99.9% for Remicade batches and 99.4–99.6% for Remsima.17 This minute difference in aggregates content may still underlie the slightly higher background signal to Remsima found in the present work, because the difference in background signal was nearly completely eliminated after purification of monomers by SEC. Regardless of the exact cause for this analytical difference, it is probably of little direct functional significance as testing ATI-negative sera proved them to be similarly devoid of blocking TNF-α binding capacity to Remsima or Remicade. It was previously suggested that pretreatment ATI levels in the upper part of the negative ATI range are associated with subsequent infliximab clinical failure, although whether these failures were due to ATI formation or not was not reported.18 We could not reproduce these findings in our Remicade-treated IBD cohort of patients who had high and low pre-exposure background ELISA signals towards Remicade. Indeed, despite the need for cautious interpretation due to possible underpower to detect a difference in this population (n=68), these patients fared similarly with respect to clinical failure rate of Remicade and the rate of formation of anti-Remicade ATI during subsequent treatment (figure 3B, C). Furthermore, two recent clinical trials found identical rates of ATI formation in patients with RA and AS treated for 1 year with Remsima or Remicade.4 ,5 Taken together, these observations suggest that the slightly higher background ELISA signal for Remsima compared with Remicade is probably of little clinical significance. However, future immunopharmacovigilance studies in larger cohorts of patients administered Remsima and Remicade will be pertinent to further corroborate this contention. These observations may also prove important when designing future assays for measuring anti-Remicade and anti-Remsima ATIs for clinical use, as the limit of detection may need to be differentially determined and adjusted separately for each drug.
Switching between infliximab and adalimumab (or other anti-TNF-α agents) is often advocated when a patient loses response to one drug, especially when loss of response is immunogenic and caused by measurable antidrug antibodies.19 ,20 Patients who develop ATI are more prone to develop ATA later on when exposed to adalimumab.21 ,22 This is probably mediated by some common genetic or other susceptibility factors, because it was reproducibly shown that ATI elicited against Remicade do not cross-react with adalimumab,12 ,13 and thereby do not in themselves comprise the subsequently developed ATA. The present study extends these observations by showing that anti-adalimumab antibodies also do not cross-react with the infliximab biosimilar Remsima (table 3), providing preliminary novel reassurance for the safety of switching from adalimumab to Remsima in cases with loss of response to adalimumab due to anti-adalimumab antibodies.
A limitation of the present study should be acknowledged, as showing cross-reactivity of anti-Remicade ATI to Remsima may not be purely analogous to showing cross-reactivity of anti-Remsima ATI to Remicade. Because of the implications for switching between the two agents, future studies should test for cross-immunogenicity of anti-Remsima ATI to Remicade in Remsima-treated patients. In addition, more data will need to be obtained to show that pretreatment higher-quartile negative ATI are also inconsequential in the case of Remsima-treated patients.
In conclusion, anti-Remicade ATI in Remicade-treated patients with IBD similarly recognise and cross-react with the bio-similar Remsima, supporting the immunogenic similarity between these two infliximab agents. Further immunopharmacovigilance studies of Remsima-treated patients are warranted to corroborate these findings.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figures
Footnotes
Contributors SB-H conceived the study, designed the experiments, interpreted the results and drafted the manuscript. YC participated in study design and interpretation and in drafting of the manuscript. MY, RE, IB, EF, OP, BU, SYL and SHK participated in acquisition and interpretation of the data and in critical revision of the manuscript for important intellectual property.
Funding This work was supported in part by a research grant from Celltrion (to SB-H), ‘Talpiot’ medical leadership grant from the Sheba Medical Center (to SB-H) and the Leona M and Harry B Helmsley Charitable Trust (to SB-H, RE and YC).
Competing interests SB-H received consultancy fees and/or research support from AbbVie, Janssen, Takeda, Schering-Plough and Celltrion. RE received consultancy fees and/or research support from AbbVie, Janssen, Takeda, Schering-Plough. YC received consultancy fees and/or research support from AbbVie, Janssen, Takeda & Schering-Plough. SYL and SHK are employees of Celltrion.
Ethics approval Sehba Medical Center IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The raw results of experiments described were available to all authors and can be made available upon request to any investigator.