Article Text

Abstract
Background: A novel T helper (Th) cell lineage, Th17, that exclusively produces the proinflammatory cytokine interleukin 17 (IL17) has been reported to play important roles in various inflammatory diseases. IL23 is also focused upon for its potential to promote Th17. Here, the roles of the IL23/IL17 axis in inflammatory bowel diseases such as ulcerative colitis (UC) and Crohn’s disease (CD) were investigated.
Methods: Mucosal samples were obtained from surgically resected specimens (controls, n = 12; UC, n = 17; CD, n = 22). IL17 production by isolated peripheral blood (PB) and lamina propria (LP) CD4+ cells was examined. Quantitative PCR amplification was performed to determine the mRNA expression levels of IL17, interferon γ (IFNγ), IL23 receptor (IL23R) and retinoic acid-related orphan receptor γ (RORC) in LP CD4+ cells, and IL12 family members, such as IL12p40, IL12p35 and IL23p19, in whole mucosal specimens. The effects of exogenous IL23 on IL17 production by LP CD4+ cells were also examined.
Results: IL17 production was higher in LP CD4+ cells than in PB. Significant IL17 mRNA upregulation in LP CD4+ cells was found in UC, while IFNγ was increased in CD. IL23R and RORC were upregulated in LP CD4+ cells isolated from both UC and CD. IL17 production was significantly increased by IL23 in LP CD4+ cells from UC but not CD. Upregulated IL23p19 mRNA expression was correlated with IL17 in UC and IFNγ in CD.
Conclusions: IL23 may play important roles in controlling the differential Th1/Th17 balance in both UC and CD, although Th17 cells may exist in both diseases.
Statistics from Altmetric.com
Crohn’s disease (CD) and ulcerative colitis (UC) are the two major forms of inflammatory bowel disease (IBD). Although the aetiology of IBD remains unclear, accumulating evidence suggests that dysfunction of the mucosal immune system plays important roles in IBD pathogenesis.1 2 Among a variety of inflammatory cells in the gut, mucosal CD4+ lymphocytes are thought to play central roles in both the induction and persistence of chronic inflammation by producing proinflammatory cytokines. Since the 1980s, T helper (Th) lymphocytes have been classified into two distinct subsets, Th1 and Th2, according to their cytokine production profiles.3 From this aspect, CD is considered to be a typical Th1 disease, and characterised by excess interferon γ (IFNγ) production in the inflamed gut.4–7 On the other hand, UC is referred to as a “Th2-like” or “mixed” phenotype because it does not exhibit clearly distinct phenotypes in this regard.4 8
Recent studies have demonstrated a tertiary subset of Th cells, designated Th17 cells, which are characterised by interleukin (IL17) production.9–11 Although important roles for IL17 in IBD pathogenesis have been proposed,12–16 in addition to the well-known “Th17 diseases” such as encephalomyelitis17 and arthritis,18 the Th1/Th17 balance of mucosal CD4+ helper T lymphocytes in IBD has not yet been investigated. Furthermore, the differences between CD and UC from this viewpoint also remain to be elucidated.
IL23 is a cytokine that shares the p40 subunit with IL12.19 It has been reported to drive chronic inflammation and is now the leading cytokine in the field of intestinal innate immunity research. Although IL12 was predominantly focused upon prior to the discovery of IL23, many recent studies using animal models have indicated that IL23 plays more important roles than IL12 in the pathogenesis of various inflammatory diseases.20 21 Furthermore, IL23 has been shown to promote the survival of Th17 cells.22 Regarding IBD, especially CD, we have focused on the role of IL12, with special reference to its Th1-promoting effect,5 7 while increased IL12 production in CD has been reported by other groups.13 23 Since the discovery of IL23, there have been several reports discussing the role of IL23 in IBD.24–30 However, further studies are needed to clarify the important roles of IL23 in human IBD, especially in relation to Th17 cells.
In the present study, we evaluated the Th1/Th17 balance in IBD by examining IL17 production by CD4+ lamina propria (LP) T cells from inflamed and non-inflamed gut using various methods, including quantitative PCR amplification, intracellular cytokine staining (ICCS), ELISA and immunohistochemistry. We also examined the expression levels of several genes associated with Th17 polarisation. Furthermore, we analysed IL17 production after stimulation with IL23 and finally concluded that IL23 may play differential roles in each disease. Specifically, it appears to enhance IL17 in UC and IFNγ in CD.
MATERIALS AND METHODS
Patients and samples
A total of 75 mucosal specimens were obtained from inflamed and non-inflamed mucosa in surgically resected specimens from 51 patients (tables 1 and 2). UC and CD patients were diagnosed based on clinical, radiographic, endoscopic and histological findings by established criteria. Samples of normal controls were taken from patients with colonic adenocarcinoma, in whom the absence of inflammation was histopathologically confirmed. CD4+ T cells in the LP were isolated unless the resected specimens were too small for the procedure (control, n = 13; UC, n = 23; CD, n = 25). The severity of local inflammation was evaluated macroscopically (0, none; 1, minimal; 2, moderate; 3, severe). Grades 0 and 1 were classified as non-inflamed, while grades 2 and 3 were classified as inflamed.
Isolation of LP CD4+ T cells
Lamina propria mononuclear cells (LPMCs) were isolated using enzymatic techniques as previously described.5 Briefly, dissected mucosa was incubated in calcium- and magnesium-free Hanks’ balanced salt solution (Sigma, St Louis, Missouri, USA) containing 2.5% fetal bovine serum (BioSource, Camarillo, California, USA) and 1 mM dithiothreitol (Sigma) for 5 min, followed by incubation in medium containing 1 mM EDTA (Sigma) for 60 min at 37°C. Next, tissues that contained LPMCs were collected and incubated in medium containing 0.02% collagenase type IV (Worthington Biochemical Corporation, Freehold, New Jersey, USA). The resulting suspension was centrifuged into a pellet, resuspended and centrifuged over a 40–60% Percoll solution (Amersham Biosciences Corporation, Piscataway, New Jersey, USA) density gradient. For isolation of CD4+ LPMCs, cells were magnetically separated using iMag CD4 MicroBeads (BD PharMingen, San Diego, California, USA). The purity of the resulting cell preparation was confirmed by flow cytometric analysis. Peripheral blood mononuclear cells (PBMCs) were isolated as previously described.31
Cell culture and stimulation
Cells were counted after Trypan blue staining to exclude dead cells, and then cultured at a density of 1×106 cells/ml in RPMI 1640 medium (Sigma) supplemented with 10% fetal bovine serum, 100 U/ml penicillin and 100 mg/ml streptomycin (Invitrogen, Carlsbad, California, USA). For stimulation of LPMCs, 10 μg/ml of immobilised anti-CD3 monoclonal antibody (mAb) (UCHT1; BD PharMingen) and 5 μg/ml of anti-CD28 mAb (CD28.2; BD PharMingen) were used. In some experiments, the cells were cultured in the absence or presence of recombinant IL23 (20 ng/ml; R&D Systems, Minneapolis, Minnesotta, USA), IFNγ (100 ng/ml; R&D Systems) or IL12 (20 ng/ml; R&D Systems) with or without the anti-CD3 and CD28 mAbs mentioned above.
ELISA and cytometric bead array
The IL17 contents in culture supernatants of sorted CD4+ cells were measured using a specific ELISA (R&D Systems). According to the manufacturer’s instructions, the minimum detectable IL17 concentration was 10.9 ng/ml. To measure the concentrations of other cytokines, a Cytometric Bead Array Human Th1/Th2 Kit (BD PharMingen) was used according to the manufacturer’s instructions.
Quantitative real-time reverse transcription-PCR
Tissue samples and isolated LP CD4+ cells were stabilized in RNA Later (Qiagen, Hilden, Germany) or RLT buffer (Qiagen) and maintained at −20°C until homogenisation. After homogenisation using a QIA shredder (Qiagen), total RNA was extracted using an RNeasy Mini Kit or RNeasy Micro Kit (Qiagen), and treated with DNase (Qiagen) to remove any contaminating genomic DNA. Complementary DNAs were synthesised with a Quantitect Reverse Transcription Kit (Qiagen) according to the manufacturer’s instructions. Quantitative real-time PCR was performed using TaqMan PCR master mix (Applied Biosystems, Foster City, California, USA) and a VIC-labelled probe for β-actin, together with FAM-labelled probes for IL17, IFNγ, IL21, IL22, IL6, tumour necrosis factor α (TNFα), retinoic acid-related orphan receptor-γ (RORC), IL12p40, IL12p35 and IL23p19 obtained from Assays On Demand (Applied Biosystems), in a DNA Engine Opticon 2 System (MJ Research, Waltham, Massachusetts, USA). The relative mRNA expression level of each molecule (in arbitrary units (AU)) was calculated by dividing the expression level by the average level in control samples after normalisation to the corresponding β-actin mRNA level.
ICCS using a fluorescence-activated cell sorter
For intracellular staining, sorted LP CD4+ cells were stimulated with phorbol myristate acetate (100 ng/ml) and ionomycin (1 μg/ml) (Sigma) in the presence of monensin (Goldistop; BD PharMingen). After 6 h, a Cytofix/Cytoperm Kit (BD PharMingen), anti-CD3 mAb (BD PharMingen), anti-IL17 mAb (eBioscience, San Diego, California, USA) and anti-IFNγ mAb (BD PharMingen) were used according to the manufacturer’s instructions. Stained cells were analysed using a FACSCalibur and the CellQuest software (Becton Dickinson, San Jose, California, USA).
Immunohistochemistry
Tissues were paraffin embedded using standard techniques. Masked antigens were retrieved by microwaving for 20 min in 1 mM EDTA buffer (pH 8.0). After blocking with 3% bovine serum albumin in phosphate-buffered saline (PBS) for 30 min, the sections were incubated for 1 h at room temperature with the following primary antibodies: goat anti-human IL17A antibody (AF-317-NA, R&D Systems), mouse anti-human CD4 antibody (Novocastra, Newcastle, UK) and normal immunoglobulin fraction as an isotype-matched control antibody. After three 5-min washes with PBS, the sections were incubated with Alexa Fluor 488-conjugated anti-mouse IgG (Molecular Probes, Eugene, Oregon, USA) or Alexa Fluor 568-conjugated anti-goat IgG (Molecular Probes) for 1 h at room temperature. Finally, the sections were washed with PBS, mounted with Fluorescent Mounting Medium (DakoCytomation), and examined using a confocal fluorescence microscope (LSM 410 inverted laser scan microscope; Carl Zeiss, Jena, Germany)
Ethical considerations
All experiments were approved by local Ethics Committees. Informed consent was obtained from all patients before obtaining samples.
Statistical analysis
The results are shown as the mean (SD). The probability of significant differences was calculated by one-way analysis of variance followed by Bonferroni’s multiple comparison test. Paired samples were compared by the Wilcoxon signed rank test. The relationship between two parameters was assessed by Spearman’s correlation coefficient test. Values of p<0.05 were considered significant.
RESULTS
IL17 is highly expressed in the intestinal LP
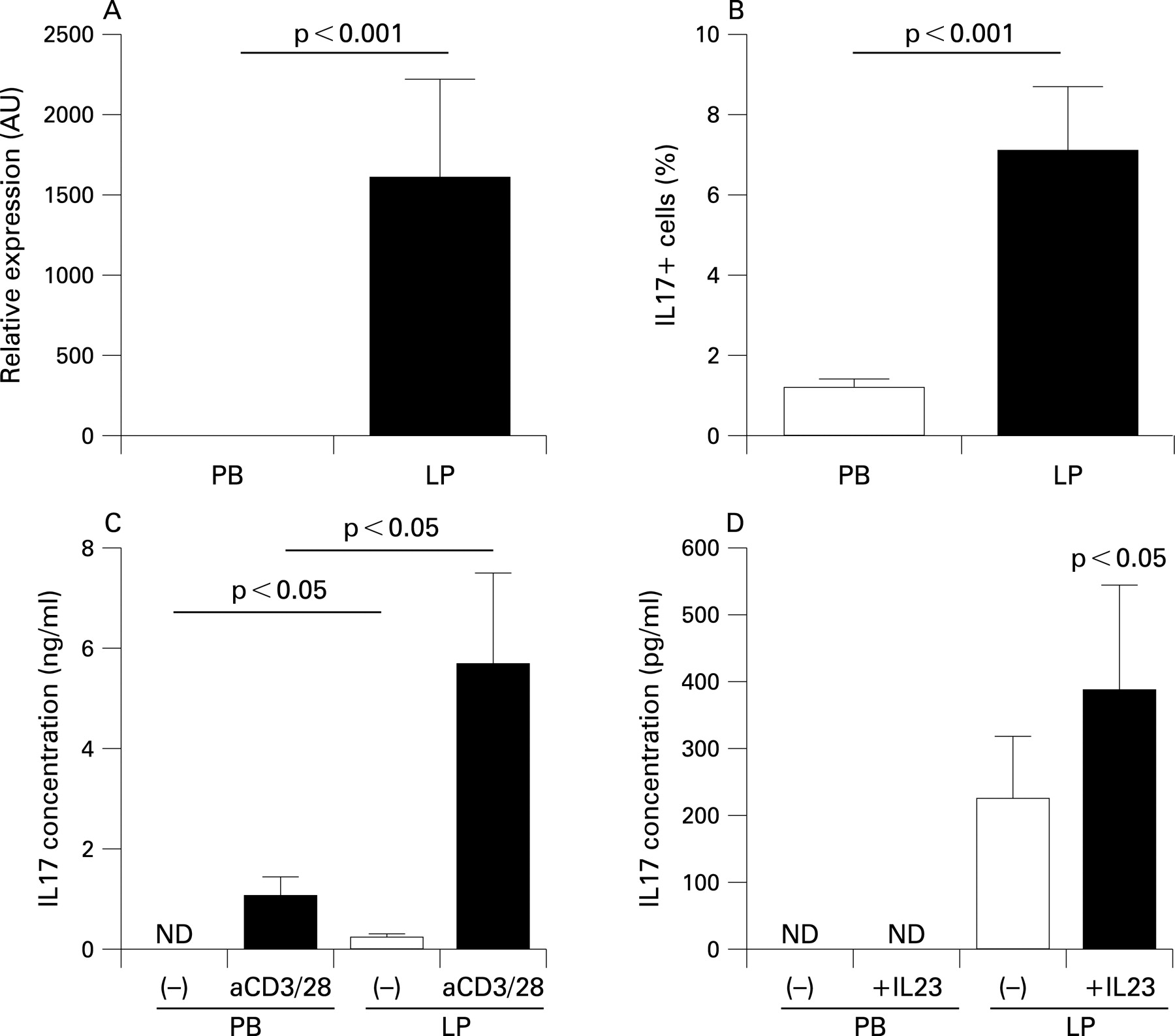
First, we investigated the physiological distribution of IL17 by comparing peripheral blood (PB) and LP samples from normal controls. To this end, we assessed isolated CD4+ T cells by quantitative PCR amplification, ICCS and ELISA. The IL17 mRNA level was higher in LP CD4+ T cells than in PB, and IL17-producing CD4+ T cells were also more abundant in the LP (fig 1A,B). When CD4+ T cells were cultured without any stimulation, only LP CD4+ T cells produced IL17 (fig 1C). T cell activation induced IL17 production by both PB CD4+ and LP CD4+ cells, but the concentration was significantly higher in supernatants from LP CD4+ cells (fig 1C). However, IL17 production by PB CD4+ cells was not detected without T cell receptor (TCR) stimulation, even in the presence of IL23 (fig 1D). These results suggest that the IL23/IL17 axis may play more important roles in intestinal mucosal immunity than in systemic immunity.

IL17 mRNA expression is upregulated in IBD, especially in LP CD4+ cells from UC
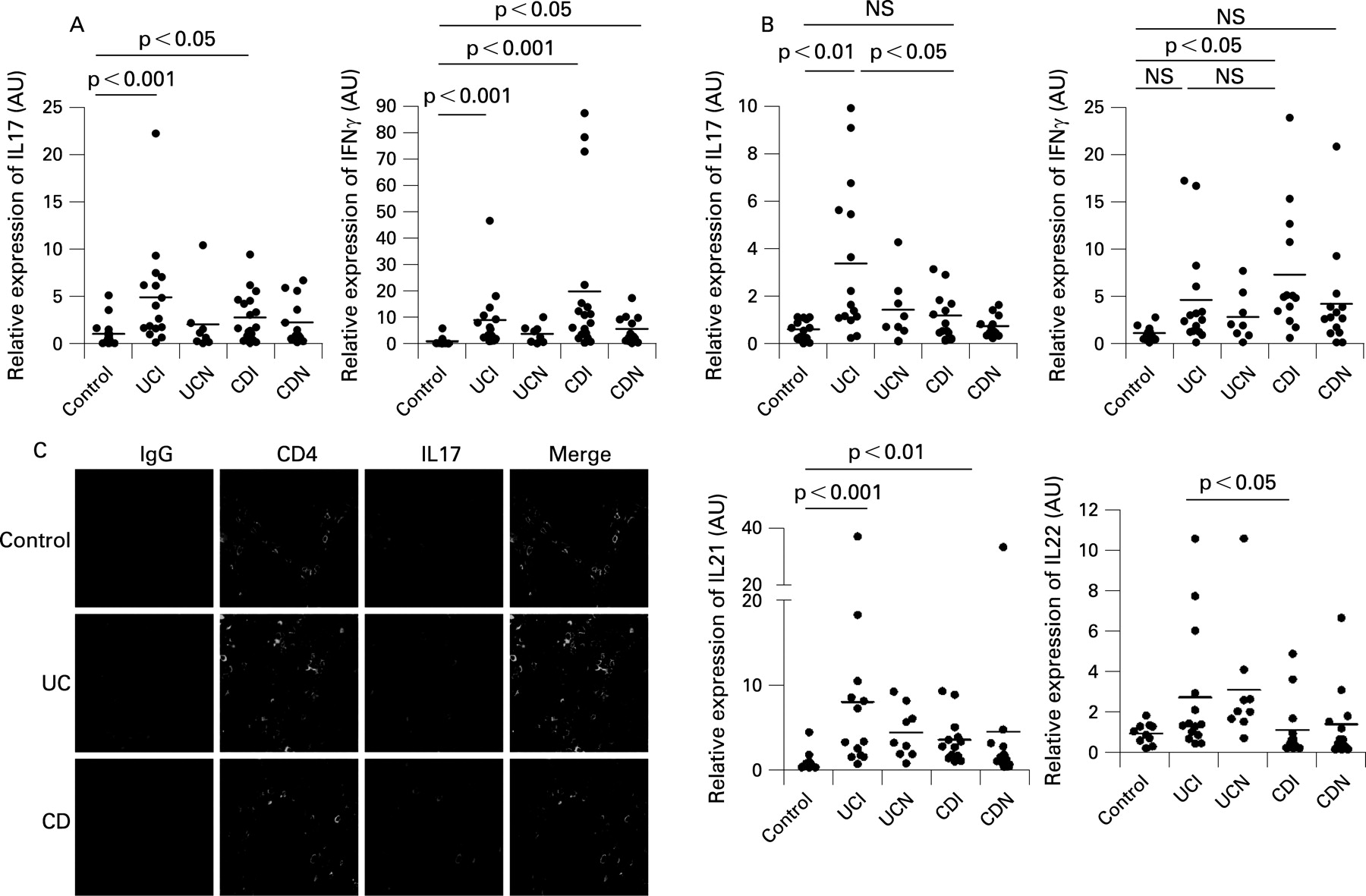
Next, we compared the IL17 mRNA expression levels in mucosal tissue specimens and isolated CD4+ T cells from IBD patients and normal controls. As previously reported,12 IL17 mRNA expression was upregulated in the mucosal samples from both UC and CD patients (fig 2A). In contrast, when we examined isolated LP CD4+ cells, IL17 mRNA expression was only significantly upregulated in cells from the inflamed LP of UC patients, and not in cells from CD patients (fig 2B). IFNγ mRNA expression was increased in the inflamed mucosa of both UC and CD patients, but its upregulation in LP CD4+ cells was only significant for inflamed mucosa of CD patients. Upregulation of T-bet (T-box expressed Tcells) was also detected in LP CD4+ cells and very strongly associated with IFNγ mRNA expression (r2 = 0.69, p<0.001; and data not shown).

Since IL17-producing CD4+ T cells, designated Th17 cells, were increased in LP samples from UC patients, we examined the mRNA expression levels of the Th17-related cytokines IL21 and IL22. These Th17-related cytokines are also produced by Th17 cells32 33 and have been proposed to play roles in IBD.34 35 IL21 was upregulated in inflamed areas of samples from both UC and CD patients and showed a tendency to be higher in UC. Similarly, IL22 expression was higher in UC than in CD (fig 2C). In contrast, TNFα was only significantly upregulated in LP samples from CD patients, while IL6 mRNA expression was higher in both types of diseases than in control samples (data not shown). We performed immunohistochemistry for IL17 to confirm its in vivo expression. As shown in fig 2D, the IL17-positive cell patterns were consistent with the CD4+ cell patterns in all three groups, and a large number of CD4+ cells were positively stained for IL17 in UC. Overall, the expression levels of IL17 and IL17-related cytokines may be more enhanced in UC than in CD.
“Potential Th17 cells” may be upregulated in both forms of IBD
Since the data in fig 2 suggested that Th17 cells may be increased in UC mucosa compared with CD mucosa, we next investigated the expression of IL23 receptor (IL23R), one of the Th17 marker candidates, on LP CD4+ cells. Quantitative PCR revealed upregulation of IL23R mRNA in LP CD4+ cells from both UC and CD patients, regardless of the presence of inflammation (fig 3A). Recently, RORγt was reported to be essential for the development of murine Th17 cells36 37 and RORC is the human orthologue of RORγt.38 RORC mRNA expression was also upregulated in both UC and CD with or without inflammation (fig 3B). Next, we evaluated the IL17 production capacity of CD4+ T cells following stimulation with anti-CD3 and anti-CD28 mAbs. As shown in fig 3C, IL17 production was increased in both UC and CD compared with normal controls, although there was no difference between the two diseases. Moreover, when we performed ICCS, IL17-producing cells were increased in both UC and CD (fig 3C and table 3), consistent with a previous report.16 IFNγ and IL17 double-positive cells did not differ significantly among the three groups. Next, we examined IL23R expression on CD4+ cells, and found that it was not limited to IL17-positive cells but was also present on IFNγ-producing cells (data not shown).

These results suggest that both UC and CD may contain mucosal CD4 cells capable of producing IL17 in response to ex vivo TCR stimulation, which may be defined as “potential Th17 cells”.
IL17 upregulation by IL23 is significantly induced in LP CD4+ cells from UC patients
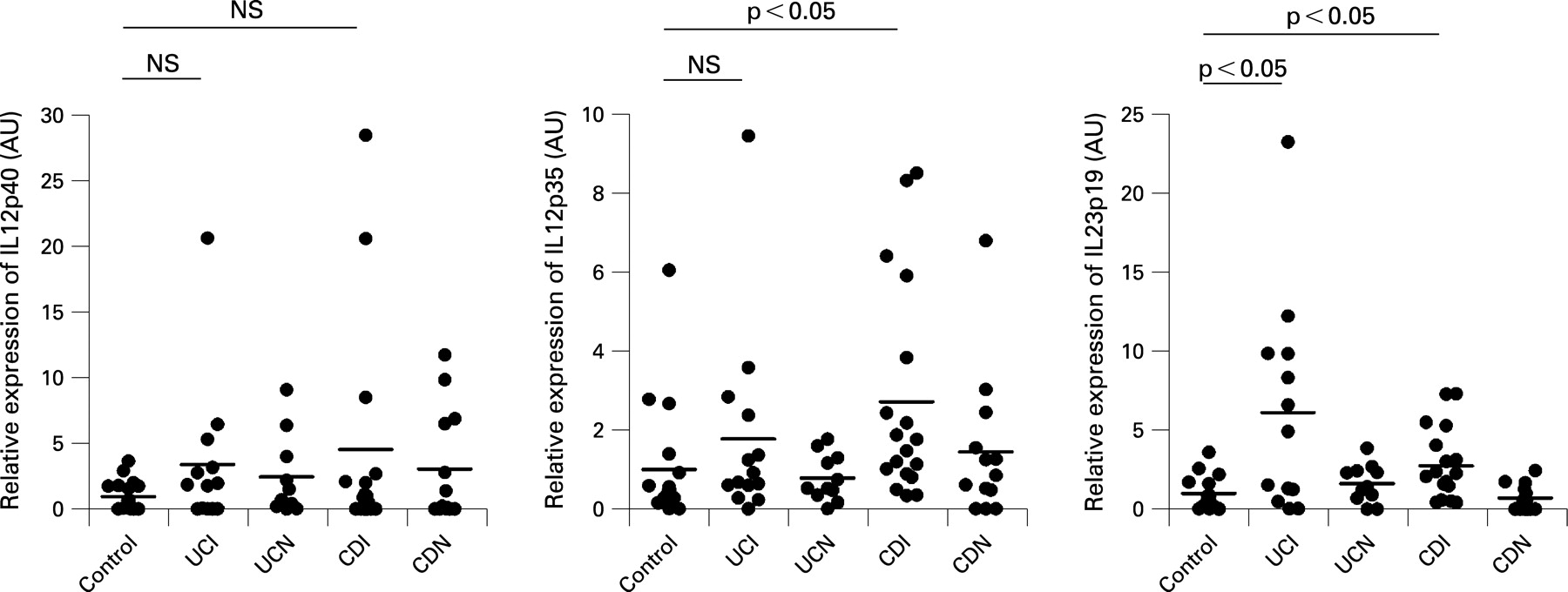
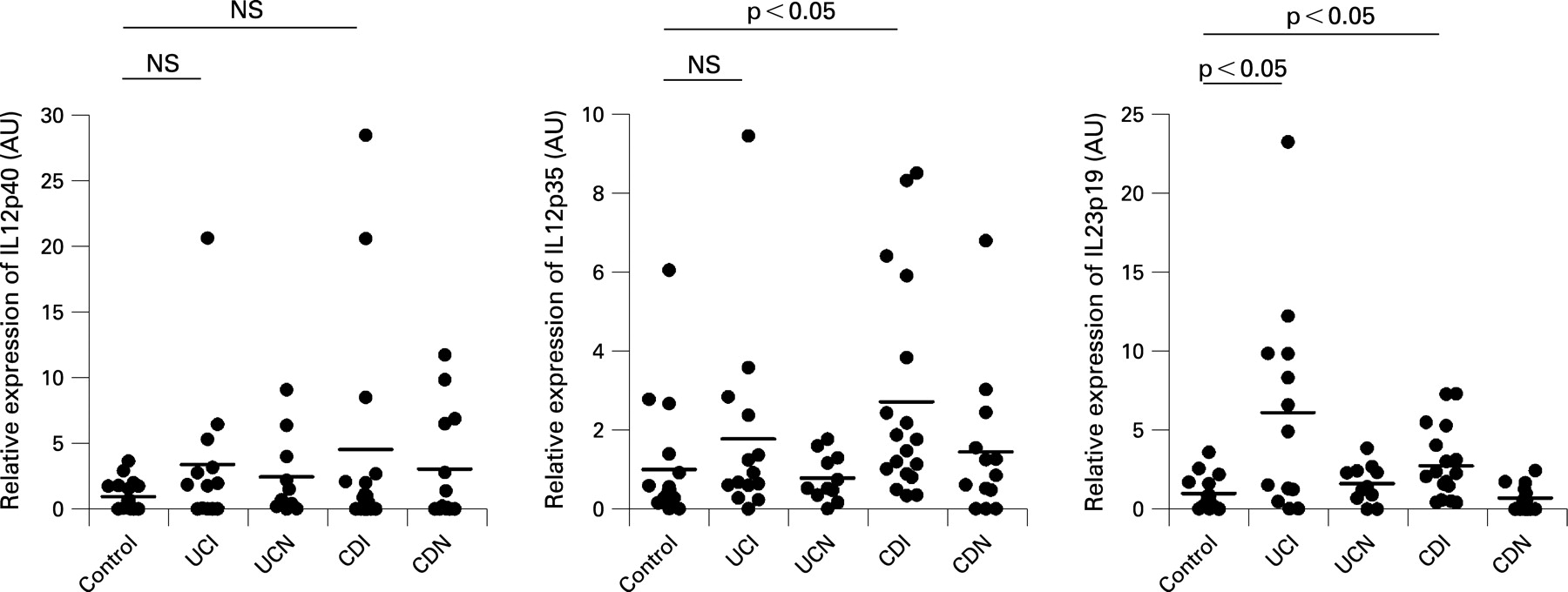
The data presented in fig 3 suggested that potential Th17 cells may exist similarly in both UC and CD. Hence, the question arises as to why IL17 is increased in UC intestinal mucosa compared with CD intestinal mucosa, as shown in fig 2. Therefore, we next examined the expression levels of IL12 family members in whole mucosa from IBD patients by quantitative reverse transcription-PCR (fig 4). Consistent with a previous report,23 IL12p40 mRNA expression showed a tendency to be higher in inflamed tissues than in non-inflamed tissues from both UC and CD patients, although the differences did not reach statistical significance. However, IL12p35 was only significantly increased in inflamed tissue samples from CD patients. In contrast, IL23p19 mRNA was markedly upregulated in inflamed UC mucosa, in addition to its significant upregulation in inflamed CD tissue.
Next, we evaluated IL17 production by LP CD4+ cells after IL23 stimulation. As shown in fig 5A, the increase in IL17 induced by IL23 was only significantly enhanced in UC LP CD4+ cells. Intriguingly, and in contrast, IFNγ production was much higher in CD LP CD4+ cells than in UC LP CD4+ cells (fig 5B). Since these results indicated that IL23 enhanced IL17 in UC and IFNγ in CD, we examined the correlation of their mRNA expression levels in whole intestinal mucosa. Consistently, IL23p19 mRNA expression was positively correlated with IL17 mRNA, but not IFNγ mRNA, in UC. In striking contrast, a positive correlation of IL23 with IFNγ mRNA, but not IL17 mRNA, was found in CD (fig 5C). Although the difference in IL23 responsiveness between UC and CD cannot be explained by IL23R expression (fig 3A), we speculated that Th1 cytokines may affect IL17 production, since several basic studies have indicated that IFNγ and T-bet can antagonise Th17 cells.39–41 To examine this hypothesis, we investigated the effects of exogenous IFNγ or IL12 on IL17 production by LP CD4+ cells. As expected, these Th1-related cytokines significantly decreased IL17 production (fig 5D). These results suggest that although potential Th17 cells may exist in CD as well as UC, their in vivo capacity for producing IL17 may be disturbed by the enhanced Th1 milieu in the CD intestinal mucosa.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
These results suggest that IL-23 may enhance the production of distinct cytokines between UC and CD, thereby contributing to the local Th1/Th17 balance in irritable bowel disease.
DISCUSSION
CD4+ effector T cells can be categorised into two distinct subsets, designated Th1 and Th2.3 However, emerging data for IL17-producing cells, designated Th17 cells, suggest that this novel CD4 subset may play very important roles in immunity and disease.9–11 For >20 years Th1 cells have been considered to mediate tissue damage centrally in many chronic inflammatory diseases. However, several reports investigating animal models have demonstrated that these cells do not sustain or play decisive roles in autoimmunity, allergy and microbial immunity,42 43 while major roles for IL17 have now been described in these diseases. In this context, rheumatoid arthritis and multiple sclerosis, which were previously considered to be Th1 diseases, are now being recategorised as Th17 diseases at least on the basis of animal studies.39–41
Regarding human IBD, the importance of the Th1 pathway in the pathogenesis of CD has long been believed to be definitive,4 5 7 24 30 while UC has not been well defined in this regard. There have been a few papers concerning IL17 in human IBD. IL17 mRNA was found to be increased in inflamed mucosa from both UC and CD, and immunohistochemistry revealed that CD3- or CD68-positive cells expressed IL17.12 13 Another study reported that upregulated expression of IL17 transcripts was detected in biopsy specimens from both UC and CD.16
The present study is the first to examine isolated LP CD4+ cells and precisely analyse Th17/Th1 cells in IBD mucosa. We found that most of the transcripts for Th17-related cytokines were increased in both UC and CD compared with normal controls, but were more abundant in UC than in CD when the two diseases were compared. In contrast, upregulation of IFNγ mRNA was marked in CD LP CD4+ cells.
To date, IL23 appears to be the key cytokine that promotes IL17 production by Th17 cells. There have been two previous reports regarding IL23 expression in human IBD. First, upregulation of IL23p19 mRNA was detected in colonic mucosa from both UC and CD patients.24 Secondly, LP macrophages from CD patients, but not UC patients, were found to produce large amounts of IL23.25 In our experiments, IL23p19 mRNA was upregulated in both UC and CD patients. Since we obtained mucosal samples and LPMCs from surgically resected specimens, differences in the surgical indications for the two diseases may have affected the severity of inflammation in the obtained samples. Most UC patients have very severe, sometimes fulminant, inflammation compared with the relatively chronic lesions in CD. In addition, we should take into consideration the fact that each patient was given various treatments.
The significance of Th17 immunity in UC was further supported by the finding that recombinant IL23 actually enhanced IL17 production by LP CD4+ cells in UC, but had a lesser effect on LP CD4+ cells in CD. The IL23R expression levels on LP CD4+ cells were similar between UC and CD. As shown in figs 2 and 4, not only IL23p19 but also IFNγ and IL12p35 were upregulated in CD, consistent with the classical view that CD is a typical Th1 disease. The Th1 pathway was reported to antagonise the Th17 pathway via various mechanisms.39–41 As shown in fig 5, IFNγ or IL12 could actually suppress IL17 production by human LP CD4+ cells. Therefore, we can hypothesise that excess IFNγ production by Th1 cells may negatively affect the IL17 production by Th17 cells in CD, despite that the finding that Th17 cells are present in CD mucosa. As a result, in terms of the Th1/Th17 balance, UC may be classified as a Th17 disease while CD remains a typical Th1 disease.
We recently reported that IL23 can enhance IFNγ production by LPMCs from CD patients,30 and further found that IFNγ was upregulated in LP CD4+ cells in the present study. Consistent with these results, the mucosal IL23p19 expression levels were correlated with IL17 in UC and IFNγ in CD. These results suggest that IL23 may enhance the production of distinct cytokines between UC and CD, thereby contributing to the local Th1/Th17 balance in IBD.
This idea may also be consistent with genetic studies on IL23R gene polymorphisms that have demonstrated altered prevalences of both UC and CD in patients with IL23R gene variants.26 44 Indeed, an anti-IL12/IL23p40 antibody has already been reported to be effective for CD,45 although IL23 and IL23R may represent more important targets for both forms of IBD, in terms of therapeutic strategies as well as basic research.
In summary, these data suggest that, in terms of the Th1/Th17 paradigm, UC may actually be classified as a Th17 disease, while CD remains a Th1 disease. Moreover, enhanced mucosal IL23 may regulate this balance differently in UC and CD.
Acknowledgments
We sincerely thank Drs M Naganuma, T Yajima, T Takayama, T Sato, A Sakuraba, K Arai, T Nakai, Y Wada and M Shibata for helpful discussions and technical assistance.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: All experiments were approved by local Ethics Committees.
Linked Articles
- Digest