Article Text

Abstract
Aim: The aim of this study was to examine the frequency and characteristics of macular lesions observed in juvenile idiopathic arthritis (JIA) uveitis, using optical coherence tomography (OCT).
Methods: In this cross-sectional study, 38 consecutive patients were recruited from a tertiary referral center in uveitis. All eyes with JIA uveitis underwent complete ophthalmic examination including OCT 3. Exclusion criterion was the inability to obtain OCT scans. Flare and visual acuity were also analysed by using linear regression.
Results: We analysed foveal thickness (FT) and central foveal thickness (CFT), using software mapping, to describe macular lesions in 61 eyes. Maculopathy was observed in 51 eyes (84%) compared with 12% in the literature (p<0.0001) and comprised four types: perifoveolar thickening in 45 eyes (74%), macular oedema in 29 eyes (48%), foveal detachment in 11 eyes (18%) and atrophic changes in six eyes (10%). Only four eyes did not demonstrate any lesion.
Conclusions: Among children with JIA uveitis, macular involvement is frequent and characterised by perifoveolar thickening and serous retinal detachment. OCT is a non-invasive instrument. It can easily identify this maculopathy, which could impair visual function, and require therapeutic intensification.
Statistics from Altmetric.com
Although most cases of pediatric uveitis are idiopathic, aetiological factors can be ascertained in some cases, with juvenile idiopathic arthritis (JIA) being the most common systemic association of chronic uveitis in childhood.1 This associated aetiology of uveitis represents a fairly high number in recent studies, ranging from 9.4% of incidence to 47%, compared with 5.1% to 12% in the 1960s.2–6
Despite the reported variations of JIA-associated disease among children with uveitis, it is unanimously observed that ocular complications and morbidity can be high.7 Asymptomatic uveitis is an important ocular manifestation in children with JIA, occuring in about 20% of patients with oligoarthritis and less often (5–10%) in those with antinuclear antibody (ANA) negative arthritis.8 The rate of complications is the higher than for other diseases, the main ones being cataract, glaucoma, band keratopathy, posterior synechiae and hypotony. The most severe ocular complications are associated with a female sex, age of uveitis diagnosis below 4 years and pauciarticular involvement.9
Manifestations involving the posterior segment in patients with acute and recurrent anterior uveitis have been widely reported in the literature; however, there are very few reports of macular lesions in JIA associated uveitis or its frequency.
The purpose of this study was to analyse OCT 3 (Carl Zeiss Meditec, Dublin, CA, USA) profiles of maculopathy in JIA-associated uveitis, and to describe the characteristic and frequency of serous retinal detachment (SRD) observed in such cases. We also analysed intraocular inflammation using laser flare cell meter (FC 2000 – Kowa, Tokyo, Japan) to correlate with the amount of retinal swelling and with the presence of a SRD.
METHODS
This was a cross-sectional case series involving patients undergoing optical coherence tomography (OCT) examination for JIA-associated uveitis between April 2005 and March 2006. Thirty-eight consecutive patients with chronic anterior uveitis and diagnosed with JIA were examined at the department of ophthalmology of Pitie-Salpetriere Hospital (Paris, France). These patients were new patients in nine cases and 29 patients who were attending the clinic in others.
There are three main classification criteria for JIA, but we adopted the definition of the International League Against Rheumatism (ILAR), defined by a duration of joint symptoms necessary for the diagnosis of arthritis of 6 weeks, with an age of the patient at disease onset under 15 years and with exclusion of other diseases. Some of our patients were referred from the Rheumatology Department of a paediatric hospital for the management of JIA and others were referred for a chronic anterior uveitis and were diagnosed as having JIA.
Ophthalmic and medical history was recorded for every patient. All patients underwent a complete examination during their first visit, including visual acuity (VA) using Snellen charts or illiterate E charts, biomicroscopy, applanation tonometry, fundus examination, optical coherence tomography and laser flare photometry (FC 2000 – Kowa) (performed in 35 patients). Fluorescein angiography and visual fields were obtained when indicated and in older children. The informed consent of the parents was obtained in each case before undergoing ophthalmic examination and optical coherence tomography (OCT). An institutional review board approval was obtained for the design of this study.
OCT examination was performed with stratus OCT 3 (Carl Zeiss Meditec) and comprised in all patients a 6 mm mapping of the macula, with additional scans to improve the assessment of macular profile. All six radial scans of each mapping were examined. We excluded from the study six eyes with severe vitreous haze, dense cataract or extensive posterior synechiae because of inability to obtain OCT scans, and also eight eyes in which uveitis was strictly unilateral. Therefore, the data from 62 eyes were analysed.
Foveal thickness (FT), the mean retinal thickness of the central 1000 µm ring, was derived from the software mapping. Central foveal thickness (CFT), the mean retinal thickness at the fixation point, was derived from the software as the average of the six measurements at the fixation point. We selected the retinal map analysis protocol on the OCT 3 to reconstruct a surface map as a false-colour topographic image displayed with numerical averages of the measurements for each of the nine map sectors as defined by the Early Treatment Diabetic Retinopathy Study.10 The inner ring was segmented into quadrants, with a radius of 1.5 mm. We defined perifoveolar thickness (PFT) as the average thickness in the central 3000 µm diameter. PFT was manually calculated using the software mapping, with averaging the four values of mean thickness in each of the quadrants in the inner ring. Particular attention was paid to the appearance of the inner–outer segment junction of the photoreceptor (IS/OS PR) line.11 As our study did not include any control group, we compared FT and CFT values with the range of normal values provided by Chan and colleagues (FT = 212±20 µm, CFT = 170±18 µm).12 These values were determined in 37 eyes from 37 healthy patients, who were aged 22 to 71 years (median 43 years). But Chan et al demonstrated by using linear regression analysis, the lack of relationship between age and foveal thickness within the 1000 µm diameter (p = 80).12
For each patient, we calculated PFT using their values in the quadrants of the inner circle (PFT = 258±15 µm). According to these values, macular oedema was defined by a FT greater than 252 µm, macular atrophy was defined by a FT lower than 154 µm, and we calculated perifoveolar thickening as a PFT greater than 288 µm. On the retinal map analysis of the OCT 3, the PFT appeared as an orange to red inner circle, instead of a yellow one as observed in a normal subject.
Statistical analysis
Results are expressed as mean with standard deviation (SD). Statistical comparison between the groups was made by using the t test, with exact p values. The most important descriptive values were expressed with 95% CI. The α level was set at 0.05 in all tests.
RESULTS
Thirty-eight patients were prospectively seen in our department between April 2005 and March 2006. Of these, 62 eyes were included because uveitis was strictly unilateral in eight patients, and because OCT could not have been performed in the other six eyes.
The mean age at the time of initial examination was 13.7 years, ranging from 5 to 52 years. The median age at onset of uveitis was about 5 years old. There were six male (16%) and 32 female (84%) participants. The main demographic and clinical characteristics of the study population are presented in Table 1.
We also recorded the medication initiated at the time of examination for each patient; only six patients did not receive any systemic medication. Treatments prescribed are presented in Table 2.
Among these patients, 38 eyes were phakic (50%), with eight eyes unaffected by JIA uveitis; 27 eyes were pseudophakic (36%) and 11 eyes were aphakic (14%).
Best corrected visual acuity (BCVA) was measured in every patient (76 eyes) using the Snellen charts. In eyes suffering from JIA uveitis, VA of 20/40 or better was found in 41 eyes, and 20/400 to light perception in eight eyes at the time of examination.
On OCT analysis, abnormalities were noted on radial scans, and were present in each of the six scans. Maculopathy was observed in 51 eyes (82%) and included four types of lesions: perifoveolar thickening in 45 eyes (73%), macular oedema in 29 eyes (47%), foveal detachment in 11 eyes (18%) and atrophic changes in six eyes (10%). These different findings were variously combined, and only four eyes with JIA uveitis did not demonstrate any maculopathy. The main characteristics of the OCT scans are given in Table 3 for each patient.
PFT was defined as previously reported in this article, by a PFT greater than 288 µm, and an orange to red inner circle on the retinal map (fig 1). This lesion was the most frequently reported and was associated with a macular oedema in 29 eyes (47%). In contrast, macular oedema (cystoid or diffuse) was always associated with a perifoveolar thickening.

Macular oedema was the second most frequent lesion, and there were only two patterns of macular oedema represented: diffuse macular edema (DME) in 28 eyes (fig 2) and cystoid macular oedema (CME) in a single eye. At initial examination, we did not observe any CME with serous retinal detachment.

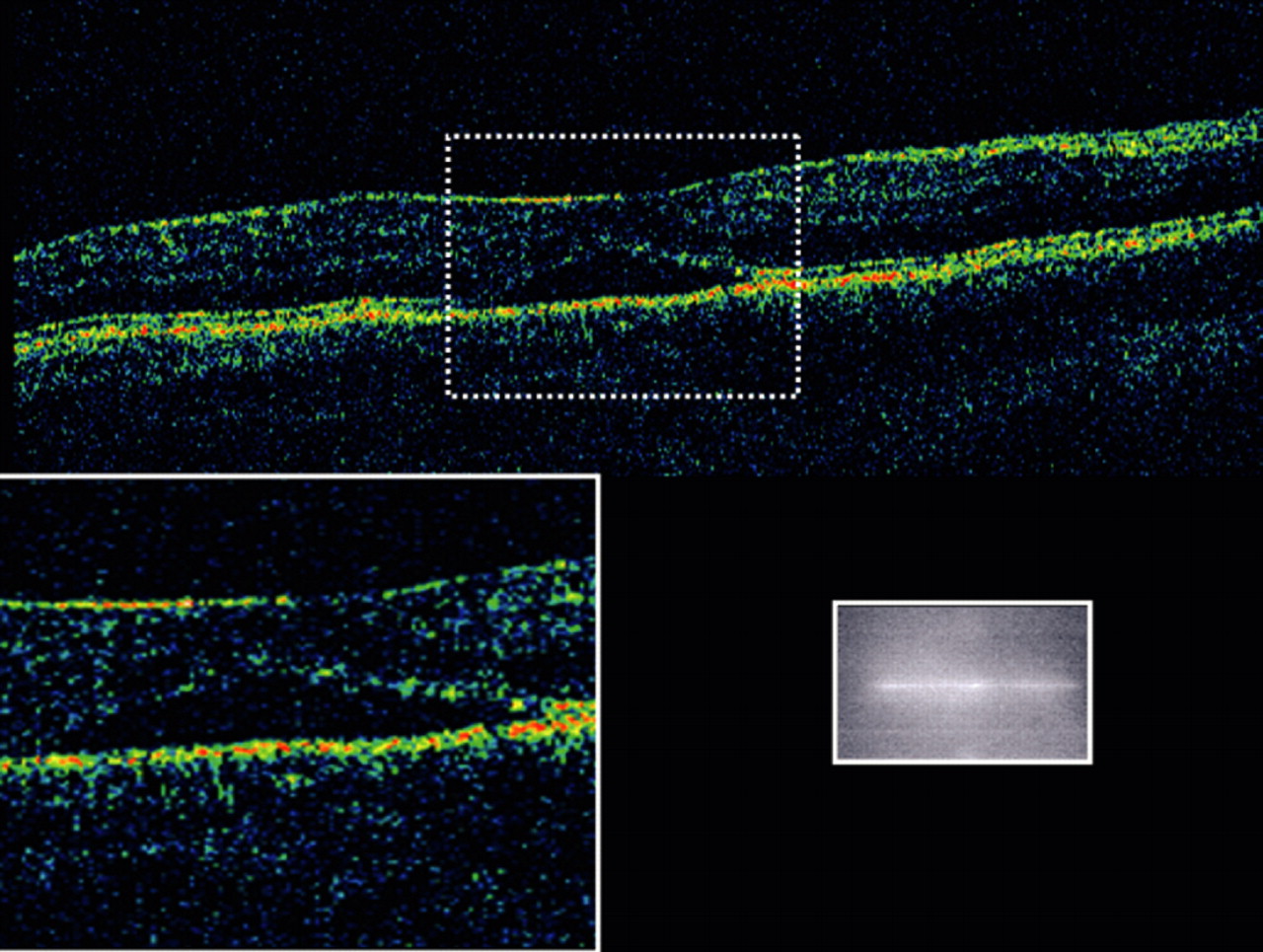
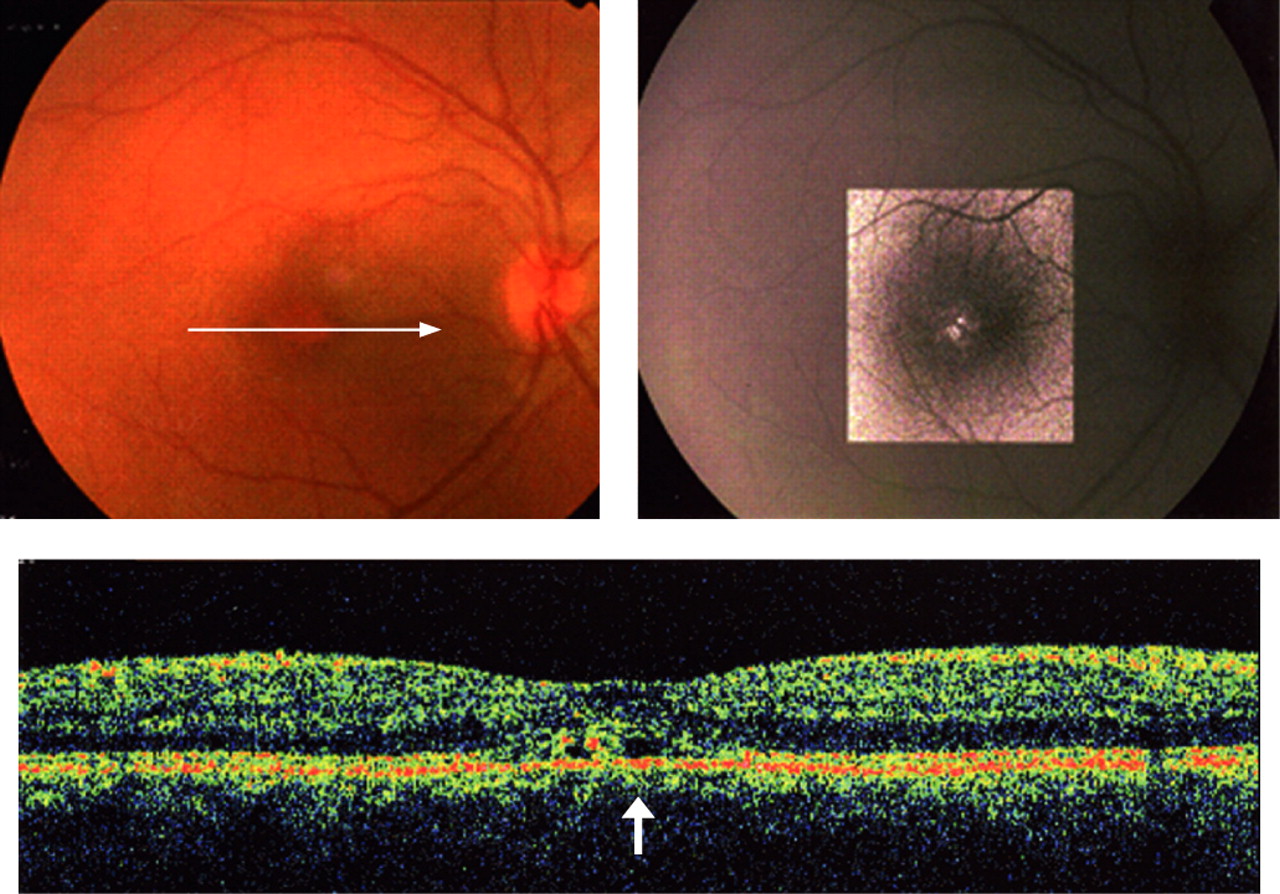
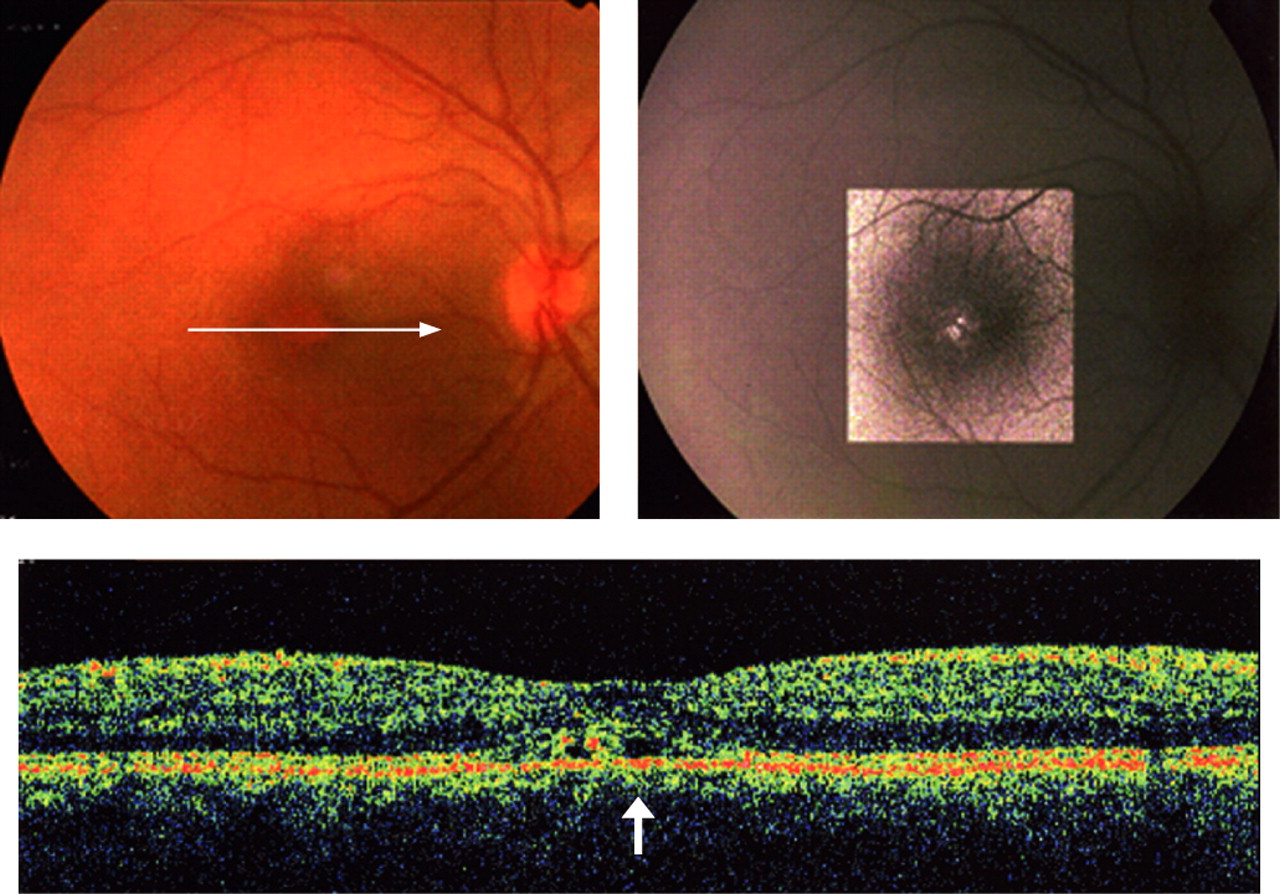
Foveal detachment was the third most common type of lesion; in 11 eyes (18%) of nine patients, we observed a very limited foveal detachment (fig 3), defined as a shallow elevation of the retina with an optical clear space between the retina and the retinal pigment epithelium. We also used calipers to measure accurately the retinal thickness of the foveolar centre in these 11 cases of foveal detachment. Despite the presence of this foveal detachment associated in most of cases with the PFT, no macular oedema was observed, and foveolar reflex was conserved. In patient 5, we performed autofluorescence retinography to avoid fluorescein injection. This picture of the right eye demonstrated an autofluorescent lesion in the foveolar area, which correlated with a small foveal detachment and with a perifoveolar thickening found on OCT horizontal scan (fig 4). This autofluorescent finding is very similar to what is observed in pseudoviteliform macular dystrophy. In these 11 eyes, intensification in anti-inflammatory treatment with an adjunction of an immunosuppressive agent allowed a complete resolution of the foveal detachment at 1 month of follow-up.
Atrophic changes of the macula were the least frequent type of macular lesions and were observed in patients who experienced end-stage glaucoma with optic nerve atrophy. This macular atrophy was determined according to FT.
We also analysed intraocular inflammation at the same visit and we performed a laser flare cell meter photometry in 36 patients. As uveitis was unilateral in seven patients, and two eyes could not have be analysed, we studied 63 values of eyes suffering from JIA uveitis. Mean laser flare meter measurements was 75.43 photons/ms.
We studied the relationship between FT (calculated as mean of FT in each eye) and intraocular inflammation measured with laser flare photometry (fig 5). Values could be analysed for 57 eyes and FT did not correlate with intraocular inflammation (r2 = 0.03 and p = 0.34).

We also analysed the relationship between FT and VA converted into the logarithm of the minimum angle of resolution (logMAR) (fig 6). Values were analysed in the 61 eyes, and we found a significant correlation using linear regression (r2 = 0.078 and p = 0.029). Visual impairment increased with FT. In these eyes presenting with a thickening in FT, VA could not have been impaired enough by occurrence of a cataract or other opacities because of the ability to obtain a good OCT scan. In the subgroup of 11 eyes presenting with a foveal detachment, seven reached a VA of 20/40 or better (64%) at the initial examination.

DISCUSSION
This study represents the largest reported group of patients with JIA-associated uveitis who have been prospectively screened for macular lesions. This chronic anterior uveitis is the most frequently associated systemic disease in children, and its frequency in cases of pediatric uveitis has been reported to be as high as 47%, but macular oedema is observed in only 3% and epiretinal membrane in 4%.4 In a recent series, the proportion of JIA-associated uveitis was higher than previously noted.7
The incidence of complications observed during the evolution of uveitis in children is highest rate in the JIA group, before idiopathic anterior uveitis and intermediate uveitis.7–9 These complications include: cataract, glaucoma, band keratopathy, posterior synechiae and hypotony. By contrast, maculopathy is more common in intermediate uveitis, and develops in more than 55% of children.7 In a recent study on JIA, only glaucoma and cataract were reported as sight-threatening complications in the course of ocular inflammation. Moreover, macular lesions are defined as the presence of macular thickening seen on clinical examination, reaching only 7% of patients, according to Woreta et al, with epiretinal membrane and macular oedema.4 But OCT analysis performed in our patients did not illustrate any macular membrane, but a frequent perimacular glittering which correlated with PFT.
Our study design was defined to determine the frequency of macular lesions associated with such an anterior and chronic uveitis, and to describe two types of particular macular involvement, determined with PFT and foveal detachment. Due to the systematic use of OCT to analyse macular thickness and retinal layers on each scan, maculopathy in JIA-associated uveitis is much more frequent (84%) than in the literature (up to 37%).7 Biomicroscopy in this specific disease is not sensitive enough to evaluate structural abnormalities or retinal thickness; OCT provides an additional technique to study cross-sectional images of the retina and to measure retinal thickness, based on the mapping software.11
The concept of PFT has not been previously reported and is very well illustrated in the 45 eyes reported on this study. We found that the thickness measurements in the peripheral inner quadrants were greater than 300 µm, with a loss of the anatomical presentation previously reported by Chan et al.12 In fact, normally, the nasal quadrant is the thickest region within the central 3 mm diameter, which is consistent with the converging of nerve fibres towards the optic disc.12
In nine patients (11 eyes), OCT examination disclosed a foveal detachment, defined as a shallow elevation of the retina, with an optical clear space between the retina and the retinal pigment epithelium, without FT. The presence of this limited SRD without a cystoid macular oedema is an interesting finding. In other types of uveitis, SRD is very frequently associated with a thickening of inner retinal tissues with cystoid space, as observed in cystoid macular oedema with SRD.13 Moreover, in all these nine patients, under therapeutic intensification, such as an adjunctive immunosuppressive agent, this foveal detachment resolved without any scar.
We observed only a single CME at initial examination, whereas there is a trend toward developing case of CME after 5 and 8 years in patients with non-idiopathic chronic anterior uveitis compared with those with idiopathic disease.14 Another patient presented a CME during follow-up; this patient did not receive any treatment during 4 months because of an adverse event with TNF blockers, and CME appeared after occurrence of a foveolar SRD (fig 7a, b). CME has already been reported associated with JIA-uveitis in a previous report, but according to our study this macular pattern is under-represented compared with other types of macular oedema in term of frequency.15

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Typically, in B27-associated uveitis, posterior segment involvement has been reported to occur secondary to anterior segment inflammation, and such lesions were also more frequent in cases of hypopyon.16 By contrast, in our study we did not find any correlation between intraocular inflammation and macular thickness. Perhaps macular involvement is linked to a prolonged and high intraocular inflammation, and this maculopathy begins with a foveolar SRD, before occurrence of a cystoid macular edema, as illustrated in fig 7.
Fig 6 demonstrates that visual impairment increased with FT. In these eyes presenting with a decrease in VA and a thickening in FT on OCT, a therapeutic intensification has to be proposed, before occurrence of chronic macular lesions. OCT is useful for studying retina, especially for assessing macular alteration, even in children. In many studies, macular oedema is still defined by ophthalmoscopic examination, or angiographic findings with fluorescein leakage, which is not sensitive enough.2 4 7 OCT, however, provides reproducible results and measures to adapt treatment and to monitor follow-up.
CONCLUSION
Despite the selection bias of our study and the results being preliminary, we analysed the frequency of maculopathy in JIA-associated uveitis, with more than 80% of eyes suffering from uveitis. Maculopathy is a very frequent ocular complication in JIA-associated uveitis. Previous studies have already documented the high rate of ocular complications at the time of diagnosis in patients with JIA, but macular involvement with foveal detachment has not been prospectively reported. These lesions may reflect a chronic level of inflammation, and SRD could appear before occurrence of CME. It is important to determine the evolution of macular involvement under appropriate anti-inflammatory regimens in order to discuss the visual prognosis in children with JIA-associated uveitis. Optical coherence tomography is a useful tool for taking care of uveitic patients.
Acknowledgments
The authors have no commercial interest in this work.
REFERENCES
Footnotes
Competing interests: None.
Linked Articles
- Correction