Article Text

Abstract
Objective Τo report outcomes of breakthrough COVID-19 in comparison with COVID-19 in unvaccinated patients with systemic rheumatic diseases (SRDs).
Methods Patients with SRD with COVID-19 (vaccinated and unvaccinated) were included by their rheumatologists in a registry operated by the Greek Rheumatology Society in a voluntarily basis. Type, date and doses of SARS-CoV-2 vaccines were recorded, and demographics, type of SRD, concurrent treatment, comorbidities and COVID-19 outcomes (hospitalisation, need for oxygen supplementation and death) were compared between vaccinated and unvaccinated patients.
Results Between 1 March 2020 and 31 August 2021, 195 patients with SRD with COVID-19 were included; 147 unvaccinated and 48 vaccinated with at least one dose of a SARS-CoV-2 vaccine (Pfizer n=38 or AstraZeneca n=10). Among vaccinated patients, 29 developed breakthrough COVID-19 >14 days after the second vaccine dose (fully vaccinated), while 19 between the first and <14 days after the second vaccine dose (partially vaccinated). Despite no differences in demographics, SRD type, treatment or comorbidities between unvaccinated and vaccinated patients, hospitalisation and mortality rates were higher in unvaccinated (29.3% and 4.1%, respectively) compared with partially vaccinated (21% and 0%) or fully vaccinated (10.3% and 0%) patients.
Conclusions Vaccinated patients with SRD with breakthrough COVID-19 have better outcomes compared with unvaccinated counterparts with similar disease/treatment characteristics.
- COVID-19
- autoimmune diseases
- vaccination
Data availability statement
Data are available upon reasonable request.
This article is made freely available for personal use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is already known about this subject?
Breakthrough COVID-19 may occur in patients with systemic rheumatic diseases (SRDs).
What does this study add?
Breakthrough COVID-19 in patients with SRD has better outcomes in terms of hospitalisation and mortality compared with unvaccinated patients with SRD with similar characteristics.
How might this impact on clinical practice or future developments?
The critical importance of full SARS-CoV-2 vaccination in patients with SRD is highlighted.
Introduction
COVID-19 has affected millions of people around the world, including those with systemic rheumatic diseases (SRDs). Vaccination against the SARS-CoV-2 virus has managed to curb the pandemic with an excellent safety profile.1–5 On the other hand, breakthrough infections (COVID-19 after vaccination) have been observed in the general population of healthcare workers,6 7 whereas few data are available for patients with SRD.8 9 Moreover, a handful of studies suggest that immunogenicity is impaired in these patients, especially in those treated with rituximab or mycophenolate mofetil.5 10 Awaiting results from studies that will assess the effectiveness of vaccination in patients with SRD, we aimed to report the characteristics and outcomes of COVID-19 in vaccinated patients compared with unvaccinated patients with SRD.
Patients and methods
Since March 2020, patients with SRD with COVID-19 are being consecutively recorded by their rheumatologists, who participate in a voluntary basis, in an ongoing registry established by the Greek Rheumatology Society. The following characteristics are recorded: age, gender, body mass index (BMI), smoking status, disease-related characteristics (type of SRD, ie, type of inflammatory arthritis, connective tissue diseases and systemic vasculitis), treatment currently received, comorbidities (based on comedication received and/or diagnosis by a specialist) and disease activity status as per clinician’s judgement (remission and low, moderate and high disease activity), vaccination-related characteristics (type of vaccine, date of vaccination, number of doses) and COVID-19 infection-related characteristics (date of SARS-CoV-2 infection confirmed by nasopharyngeal PCR, presenting symptoms, outcomes such as hospitalisation, need for oxygen supplementation, ICU admission and death).
Comparisons were made between unvaccinated patients and vaccinated patients with COVID-19. Patients who had received both doses of vaccination and presented with COVID-19 ≥14 days after the second vaccine dose were considered as ‘fully vaccinated’; those who were infected between the first dose and <14 days after the second dose were considered as ‘partially vaccinated’.11 Continuous variables were expressed as mean (±SD) and categorical variables were expressed as percentages (%). Two-sided Fisher’s exact test and Mann-Whitney test were used to compare categorical and continuous characteristics, respectively. Statistical package SPSS V.21.0 was used.
Results
Between 1 March 2020 and 31 August 2021, 195 patients with SRD (73% women with a mean age of 51.3±14.1 years) and COVID-19 were recorded. Of these patients, 147 were unvaccinated, while 48 had received at least one dose of SARS-CoV-2 vaccine, namely, Pfizer or AstraZeneca in 38 (79%, mean±SD age: 48.6±13.4) and 10 (21%, mean±SD age: 61.0±7.7), respectively. Of the 48 patients, 12 (25%) had temporarily discontinued their treatment, which is in partial agreement with published data.12 Among the 48 vaccinated patients with breakthrough COVID-19, 29 were fully vaccinated. As depicted in figure 1, the median time from the first vaccine dose to COVID-19 diagnosis (positive PCR) was 70 (range 19-200) days.

Timepoints of breakthrough COVID-19 in 48 vaccinated patients with systemic rheumatic disease after the first or second dose of Pfizer or A-Z vaccine. A-Z, AstraZeneca.
As shown in table 1, there were no differences in terms of demographic and clinical characteristics of SRDs (disease type, treatment profile and disease remission status), as well as in terms of comorbidities, between unvaccinated and vaccinated patients.
Comparable demographic and clinical characteristics between unvaccinated and vaccinated patients with SRD with COVID-19
Most of the patients with SRD enrolled in this cohort suffered from inflammatory arthritis (57%), including rheumatoid arthritis, psoriatic arthritis and axial spondyloarthritis. The remaining patients had various connective tissue diseases and vasculitis (online supplemental table 1). About one-third of our patients were receiving glucocorticoids with figures being similar for treatment with biological and targeted synthetic DMARDs. Noteworthy is that seven patients who were on rituximab (one with rheumatoid arthritis (RA), one with systemic lupus erythematosus (SLE), three with systemic sclerosis (SSc) and two with ANCA-associated vasculitis (AAV) recovered fully, although three out of five unvaccinated patients were hospitalised. With regard to mycophenolate mofetil, which has also been associated with blunted immune responses against SARS-CoV-2,5 10 from the 11 patients who were on this drug; 6 had not received the vaccine; 4 were fully vaccinated; and 1 was partially vaccinated. Three patients (one from each group) were hospitalised, while one unvaccinated patient died. Comorbidities were present in about 70% of our patients, with arterial hypertension being the most common.
Supplemental material
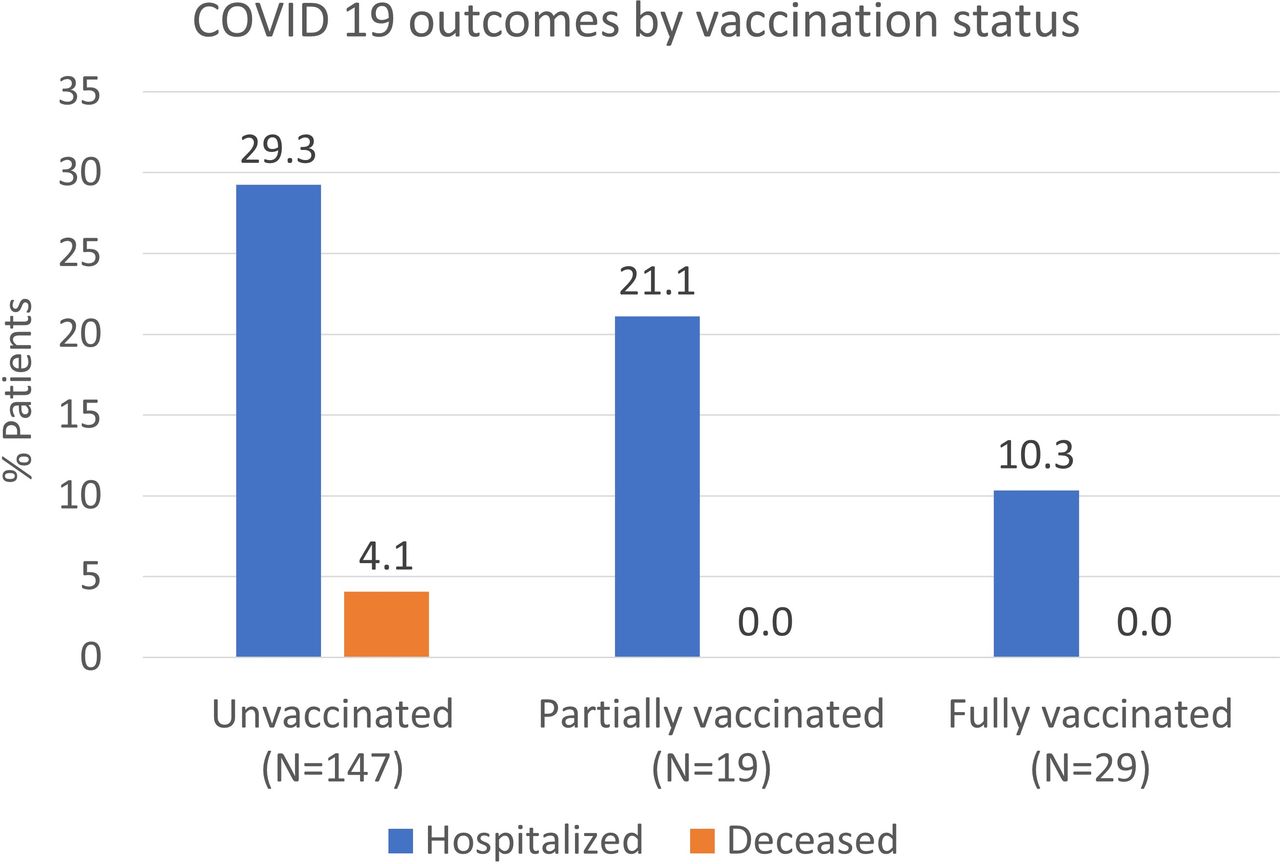
Despite the lack of differences between unvaccinated and vaccinated patients, there were differences in terms of COVID-19 outcomes. Need for oxygen supplementation was more commonly required in unvaccinated (27.9%) compared with vaccinated (14.6%, p=0.08) or fully vaccinated (10.3%, p=0.06) patients. Similarly, no vaccinated patient required invasive ventilation in contrast to 2.7% of the unvaccinated patients (n=4). More importantly, as shown in figure 2, hospitalisation rates were higher in unvaccinated (43/147, 29.3%) compared with partially (4/19, 21%, p=0.59) or fully vaccinated (3/29, 10.3%, p=0.0377) patients. There were six deaths among unvaccinated (4.1%) compared with none among vaccinated patients with COVID-19.

{kind=link}
{kind=link}
COVID-19 outcomes according to vaccination status.
Discussion
This is the first study showing the outcomes of breakthrough COVID-19 in vaccinated patients with SRD compared with a control group of non-vaccinated ones. Our results suggest that COVID-19 is associated with a better outcome in fully vaccinated patients compared with unvaccinated patients. Statistical significance was not reached for partially vaccinated patients, possibly due to their low number. It should be noted though, that no deaths were reported in this subgroup of patients. Moreover, across compared groups, no differences were recorded regarding demographic and clinical characteristics, including disease activity status which may affect COVID-19 outcome.13
Both hospitalisation and death rates were much lower in our unvaccinated patients, compared with that reported.8 9 This might be due to the larger number of patients in our study and/or to the different disease/treatment characteristics between patient cohorts. Of note, hospitalisation and death rates in our unvaccinated patients were comparable to those described by a previous observational study examining COVID-19 outcomes in patients with SRD in our country.14
As shown in figure 1, and in accordance with other reports,8 9 about half of our patients got infected during the first 10 weeks after the second vaccine dose. Although it is well known that vaccine efficacy declines overtime, therefore most breakthrough infections would be expected to occur closer to the end of the observational period; it should be noted that temporal fluctuations of the viral load in the community, during spring 2021 in Greece,15 explain our results.
Our study has certain limitations. First, antibody response to vaccination were not routinely measured in our patients; this might have been weakened by treatment received, although, as already mentioned, there were no differences in medication use between groups. Second, selection bias cannot be excluded as the participation of rheumatologists who referred their consecutive patients in the registry was on a voluntary basis. Third, an inevitable limitation was that most of the unvaccinated patients were infected by COVID-19 in an earlier time period, presumably with different SARS-CoV-2 variants, compared with their vaccinated counterparts. Actually, based on the genomic surveillance of COVID-19,15 the delta variant became prevalent in Greece after the first week of July 2021. Thereafter, 3 unvaccinated, 1 partially vaccinated and 27 fully vaccinated patients were recorded and 3/27 were hospitalised. Fourth, the different time of recruitment into the groups could reflect different therapy options in 2020 and 2021, thus affecting outcomes of hospitalised patients. However, using as a cut-off 1 March 2021,when the vaccination programme for patients with SRD started in our country, we found that the data are largely similar between the two periods. While up to 28 February 2021, 90 unvaccinated patients contracted COVID-19 and 2 (2.2%) died, 105 other patients contracted COVID-19 thereafter and 4 (3.8%, all unvaccinated) died. Finally, the number of patients who died was low (n=6). Therefore, conclusions about mortality should be interpreted with caution.
In conclusion, the preliminary results presented herein show that breakthrough COVID-19 may occur in patients with SRD. However, compared with non-vaccinated patients, the outcome seems to be better, irrespective of the type of SRD or concurrent treatment. Continuous efforts to increase primary vaccination coverage especially towards vaccine-sceptical patients, as well as booster vaccination in patients with SRD, are needed.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Due to the anonymised and non-interventional nature of the survey, ethics approval and patient consent were not required.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Lay summary
Disclaimer : This is a summary of a scientific article written by a medical professional (“the Original Article”). The Summary is written to assist non medically trained readers to understand general points of the Original Article. It is supplied “as is” without any warranty. You should note that the Original Article (and Summary) may not be fully relevant nor accurate as medical science is constantly changing and errors can occur. It is therefore very important that readers not rely on the content in the Summary and consult their medical professionals for all aspects of their health care and only rely on the Summary if directed to do so by their medical professional. Please view our full Website Terms and Conditions.
Copyright © 2022 BMJ Publishing Group Ltd & European League Against Rheumatism. Medical professionals may print copies for their and their patients and students non commercial use. Other individuals may print a single copy for their personal, non commercial use. For other uses please contact our Rights and Licensing Team.
Footnotes
Handling editor Josef S Smolen
Twitter @FragoulisGeorge, @Dr_C_Koutsianas
Contributors Drafting of the manuscript and data analysis: CP, GEF, DV and PPS. Data acquisition and revision of the manuscript: all authors. guarantor: PPS
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.