Article Text

Abstract
Objectives To estimate the global burden of rheumatoid arthritis (RA), as part of the Global Burden of Disease 2010 study of 291 conditions and how the burden of RA compares with other conditions.
Methods The optimum case definition of RA for the study was the American College of Rheumatology 1987 criteria. A series of systematic reviews were conducted to gather age-sex-specific epidemiological data for RA prevalence, incidence and mortality. Cause-specific mortality data were also included. Data were entered into DisMod-MR, a tool to pool available data, making use of study-level covariates to adjust for country, region and super-region random effects to estimate prevalence for every country and over time. The epidemiological data, in addition to disability weights, were used to calculate years of life lived with disability (YLDs). YLDs were added to the years of life lost due to premature mortality to estimate the overall burden (disability-adjusted life years (DALYs)) for RA for the years 1990, 2005 and 2010.
Results The global prevalence of RA was 0.24% (95% CI 0.23% to 0.25%), with no discernible change from 1990 to 2010. DALYs increased from 3.3 million (M) (95% CI 2.6 M to 4.1 M) in 1990 to 4.8 M (95% CI 3.7 M to 6.1 M) in 2010. This increase was due to a growth in population and increase in aging. Globally, of the 291 conditions studied, RA was ranked as the 42nd highest contributor to global disability, just below malaria and just above iodine deficiency (measured in YLDs).
Conclusions RA continues to cause modest global disability, with severe consequences in the individuals affected.
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is a systemic autoimmune disorder that causes pain and swelling of multiple joints of the body. Previous studies have estimated the burden of RA from data primarily obtained from Anglo-Saxon populations in the USA and Europe,1 ,2 with minimal information from other parts of the world. The Global Burden of Disease 2010 study (GBD 2010 Study) extended on these earlier studies and was a comprehensive effort to measure epidemiological levels and trends of 291 diseases covering 187 countries. Using these updated methods as part of the GBD 2010 Study, the current global burden of musculoskeletal (MSK) conditions was estimated.
While recent articles from the GBD 2010 Study report the overall global burden of the 291 conditions studied,3 ,4 this paper, on the global burden of RA, is one of a series of papers published in Annals of Rheumatic Diseases that report the burden of MSK diseases, including osteoarthritis, low back pain, neck pain, gout, other MSK conditions, osteoporosis and occupationally related low back pain.5–12 Here, detailed methods and results for estimating the global burden of RA for the GBD 2010 Study are reported.
Methods
The GBD 2010 Study methods paper published in Annals of Rheumatic Diseases describes in detail the process of the overall MSK group estimates.8 This paper, which should be read in conjunction with the MSK methods paper, will describe the RA aspect of the GBD 2010 Study.
The RA Expert Group established case definitions, health states and severity distributions, and performed the systematic reviews. The Institute of Health Metrics and Evaluation Core Team established disability weights (DW), mortality estimates and finalised years lived with disability (YLD), years of life lost (YLL) and disability-adjusted life years (DALY) estimates, the measures of disease burden.
The primary tool for estimating burden of disease in the GBD 2010 Study was the meta-regression tool, DisMod-MR.4 ,13 RA prevalence, incidence and mortality data were entered into DisMod-MR, which pooled the available heterogeneous data to adjust for methodological differences and checked these data for internal consistency. DisMod-MR used these data to predict values for countries and regions with little or no data using disease-relevant country characteristics and random effects for country, region and super-region (see online supplementary appendix 1). DisMod-MR produced a full set of age/sex/region/year-specific estimates for prevalence, which were used to calculate YLD.
Case definition
For the GBD 2010 Study, the 1987 American Rheumatism Association (ARA) criteria for RA14 were considered the optimal definition. Studies that used earlier criteria for the definition of RA, such as the 1958 ARA criteria, were included in the review and were flagged with a covariate in the DisMod analysis. The most recent 2010 American College of Radiology (ACR)/European League Against Rheumatism (EULAR) criteria15 that are more inclusive of early RA were not available when this study was undertaken.
While RA is known to affect internal organs (including disorders such as pericarditis, pulmonary fibrosis, peripheral neuropathy) in addition to the joints, these extra-articular effects are not factored into the models used in the GBD 2010 Study.
The studies included in this systematic review were those in which RA was diagnosed by a medical practitioner. Identification of potential cases was often through questionnaires (either self-administered or by research staff). Those people who identified they had been previously diagnosed with RA or those who reported symptoms indicative of RA were then examined by a medical practitioner, and based on this examination a diagnosis was made. Data from studies that solely relied upon self-administered questionnaires or self-report of a RA diagnosis were excluded.
Systematic review
A systematic review of the prevalence, incidence and mortality of RA was conducted (see online supplementary appendix 2 for details). All included studies were assessed for risk of bias using a tool specifically developed for the MSK estimation in the GBD 2010 Study.16
There were 8043 results from the initial prevalence search. After examination for eligibility of titles and abstracts, 56 published studies (268 age-sex-specific estimates) were included in the analysis. These were from 40 countries and 16 of the 21 GBD 2010 Study world regions (see online supplementary appendix 1). Prevalence data were not available for Central Asia; Australasia; Latin America, Andean; Sub-Saharan Africa, Central; and Sub-Saharan Africa, East; hence, estimates for these regions were calculated in DisMod-MR. Figure 1 shows the global distribution of prevalence data used for the DisMod-MR analysis and highlights where data are sparse or missing.

Prevalence data count for rheumatoid arthritis DisMod-MR analysis, Global Burden of Disease 2010 study.
In the incidence search, 7294 titles were examined, and 23 studies were deemed eligible for inclusion. These provided 191 estimates from 10 countries from 6 regions. Incidence data were not available from Asia, Central; Asia, East; Asia, Southeast; Australasia; Caribbean; Eastern Europe; Latin America (Andean, Central, Southern and Tropical); Oceania; and Sub-Saharan Africa (Central, East, Southern, West), and estimates for these regions were calculated in DisMod-MR.
The initial systematic review was conducted in March 2009 and included data published up to this time. To identify any additional data that had been published since the initial review, MEDLINE, Pre-MEDLINE, EMBASE and CINAHL were searched again in March 2013. As this search was completed after the DisMod-MR analysis, the data obtained from the updated search were not included in the ‘Results’ section. The details of this search are shown in online supplementary appendix 3.
For the purpose of the GBD 2010 Study, remission is classified as a complete cessation of symptoms, without ongoing treatment and thus differs from current clinical definitions of treatment-induced remission. While complete ongoing remission does occur in very few cases, it primarily occurs in early RA and the potential duration is unknown. For the DisMod-MR analysis, remission was assumed to be zero.
Twenty-three articles were included from the systematic review on the mortality of RA (77 estimates), providing data from eight countries covering two regions (North America, high income; and Western Europe) (see online supplementary appendix 2). Cause-specific mortality data were also available from the GBD 2010 Study mortality analyses described below. Mortality rates by age, sex and region for 1990, 2005 and 2010 were added to the DisMod-MR models to help guide differentials in prevalence estimates, particularly for countries and regions with little or no data.
Mortality analyses
Premature mortality due to RA was computed by the team at Institute for Health Metrics and Evaluation as YLLs based on cause of death estimates from 1980 to 2010 for 20 age groups, both sexes, and 187 countries. Cause of death estimates were developed using a comprehensive database of vital registration, verbal autopsy and surveillance sources. Ultimately 2290 country-years of data from 123 countries were used for the estimation of RA mortality. An ensemble modelling strategy was used for death estimation, employing mixed effects linear models and spatiotemporal Gaussian process regression models weighted by out-of-sample predictive validity. This process is described in detail elsewhere.17 Where data were sparse or missing, the models were informed by borrowing strength across space and time and by using relevant covariates. RA models included a transformed measure of average income per capita, education level and an aggregate measure of health system access, which takes into account indicators such as hospital beds per capita, in facility deliveries and vaccination coverage rates. The models also included smoking and obesity as these have been associated with increased risk of RA, vegetable consumption as it has been inversely associated with risk of RA and cholesterol because elevated levels have been observed in RA populations.18 The assumed direction of the covariate for alcohol consumption was erroneously included for a positive relationship rather than a protective effect. The covariate would have dropped out of the model unless data suggested that a positive relationship between alcohol and RA mortality improved the model fit. As a result, the alcohol covariate was not taken into account, but this is unlikely to have affected the model output as the presumed negative correlation with alcohol is small.
Uncertainty in cause of death model predictions was captured using standard simulation methods by taking 1000 draws for each age, sex, country, year and cause. The estimates for RA and an additional category of other MSK diseases were scaled to the total number of MSK deaths, taking into account the levels of uncertainty associated with each estimate. The resulting predicted numbers of deaths were converted to measure YLLs by multiplying deaths at any age with the remaining life expectancy for that age from a model life table.19
Modelling in DisMod-MR
RA prevalence, incidence and mortality data were entered into DisMod-MR for modelling and calculation of estimates. Remission was set to zero, and incidence and prevalence before the age of 5 years was assumed to be zero (see online supplementary appendix 4 for details of model settings). Study-level covariates for coverage (regional vs national) and variations from optimal case definition had very small coefficients and hence were not included as covariates in the final model. The coefficient for the age-standardised death rate for RA was close to zero and hence did not affect the estimates. DisMod-MR then generated an age pattern for each sex/region/year grouping, and results were checked for plausibility.
Severity and DW and finalising YLD estimates
Three sequelae were chosen to characterise the different levels of severity of RA, and the health state of each of these was defined in technical and lay terms (table 1). Surveys in five countries and an open-access internet survey were conducted by the GBD 2010 Study Disability Weights Group. In these surveys, pairwise comparisons were presented and respondents were asked to indicate which of the two hypothetical health states they considered to be healthier. Results were used to derive DWs to reflect the severity of each health state on a continuum between zero (equivalent to full health) and one (equivalent to death).20
Sequelae for RA and associated disability weight in the GBD 2010 Study
To determine the proportion within each of the severity levels (mild, moderate and severe), eight studies from three regions (North America, high income; Western Europe; and North Africa/Middle East) provided information on the severity of RA.21–28 Severity was classified according to Health Assessment Questionnaire (HAQ) scores, with the cut-off scores for each severity level taken from previous published studies. Estimates were pooled across studies, for males and females separately, using a quality effects model in meta-XL.29 The pooled proportions for females and males and combined DWs are shown in table 2.
Disability weights and proportions by severity levels for males and females
Finalise burden estimates
The DALY was the standard metric used to quantify burden30 and was calculated by combining YLL due to premature mortality and YLD. The combined DW was multiplied by the age/sex/region-specific prevalence for the years 1990, 2005 and 2010 to derive YLDs. The uncertainty interval around each quantity of interest was calculated from SEs around all data inputs and the uncertainty from all steps of data manipulations in DisMod-MR and the severity distributions. Uncertainty ranges are bounded by the 2.5 and 97.5 centile values of 1000 draws of the posterior distribution. Further detail on how uncertainty was calculated can be found elsewhere.3 Summary prevalence estimates were standardised using the 2001 WHO standard population.31
Results
The global prevalence of RA (from 5 to 100 years of age) in 2010 was estimated to be 0.24% (95% CI 0.23% to 0.25%) (figure 2) and was approximately two times higher in females (mean 0.35%; 95% CI 0.34 to 0.37) than males (mean 0.13%; 95% CI 0.12 to 0.13) (table 3). There was no discernible change in prevalence from 1990 (mean 0.25%; 95% CI 0.24 to 0.26—see online supplementary appendix 4 for regional data) to 2010 for either males or females.
Prevalence and DALYs for RA in the age range 5–100 years, by region and sex, GBD 2010 Study
{kind=link}
{kind=link}
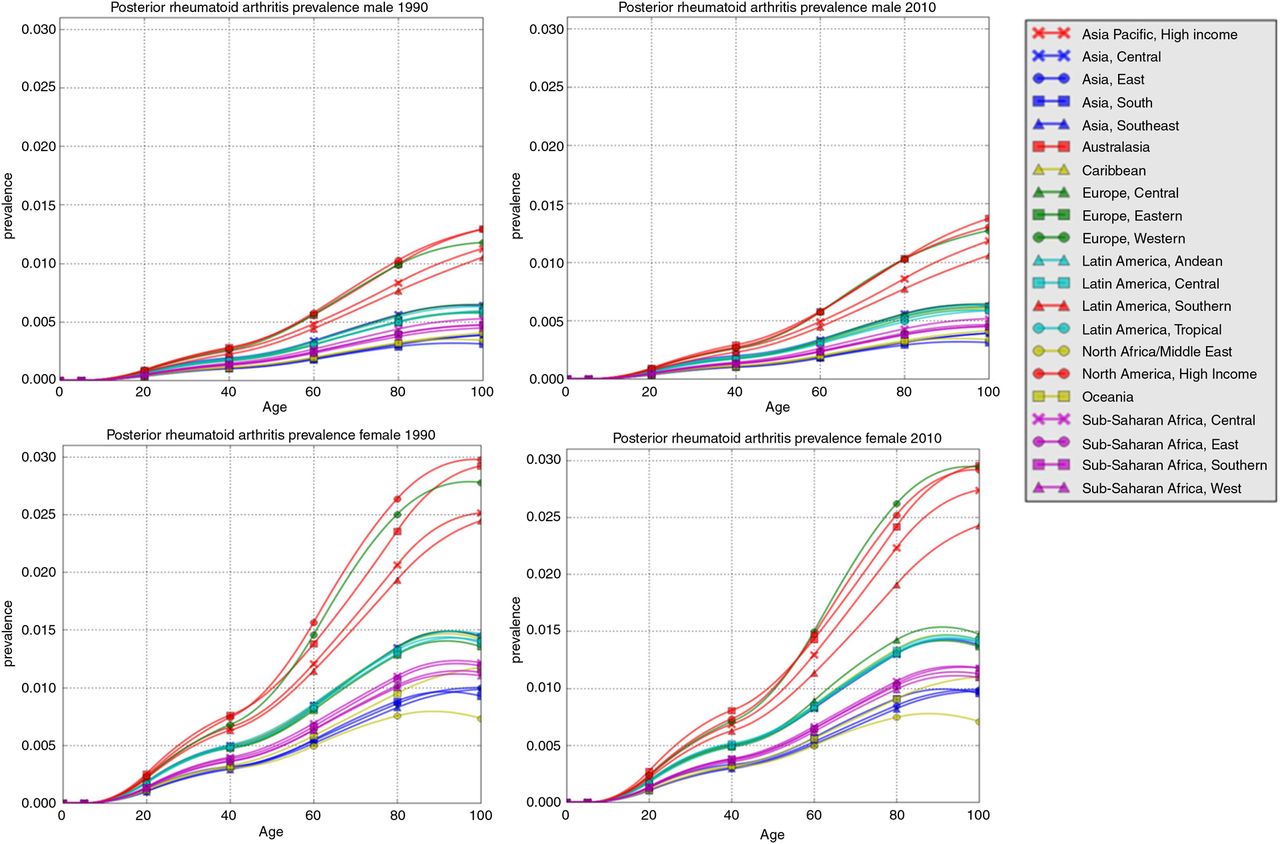
DisMod-MR-generated 1990 and 2010 prevalence of rheumatoid arthritis by region, Global Burden of Disease 2010 study.
Modelled age-standardised prevalence in 2010 was highest in the Australasian region (mean 0.46%; 95% CI 0.3 to 0.7), followed by Western Europe (mean 0.44%; 95% CI 0.4 to 0.5) and North America, high income (mean 0.44%; 95% CI 0.4 to 0.5); and lowest in Asia, East (mean 0.16%; 95% CI 0.15 to 0.18); Asia, Southeast (mean 0.16%; 95% CI 0.15 to 0.18); and North Africa/Middle East (mean 0.16%; 95% CI 0.14 to 0.19).
The age-standardised death rate from RA decreased by 9.9% from 1990 to 2010 and is approximately 0.8 per 100 000. However, there is considerable uncertainty surrounding this rate.
YLD and DALYs
Globally, of the 291 conditions studied,3 RA was ranked as the 42nd highest contributor to global disability (measured in YLDs; placed between malaria and iodine deficiency) and represented 0.49% (0.36–0.62%) of total YLDs. YLDs for RA increased from 2 566 000 (95% CI 1 831 000 to 3 381 000) in 1990 to 3 776 000 (95% CI 2 672 000 to 4 954 000) in 2010. Adjusting for the population increase over this period and aging of the population, YLDs for RA increased from 48/100 000 population in 1990 to 55/100 000 population in 2010. YLDs were highest in females (87.84/100 000; 95% CI 61.96 to 115.52) compared with males (22.46/100 000; 95% CI 15.99 to 29.66).
All ages DALYs for RA increased from 3 335 000 (95% CI 2 573 000 to 4 192 000) in 1990 to 4 815 000 (95% CI 3 705 000 to 6 056 000) in 2010, an increase of 44%. In 1990, RA was ranked 85th in global DALYs and accounted for 0.13% of total DALYs. In 2010, RA was ranked 74th in global DALYs, accounting for 0.19% of total DALYs.
Discussion
New estimates of the global burden of RA
Of the 291 conditions studied in the GBD 2010 Study, RA was ranked 74th in terms of burden as measured by DALYs, and 42nd in terms of disability as measured by YLDs, just below malaria and just above iodine deficiency. Global prevalence remained stable from 1990 to 2010. The major peak of RA prevalence occurred in older ages, and with aging populations throughout the world and a decline in mortality, particularly in low-income and middle-income countries, the number of people living with RA will increase substantially over coming decades.
In GBD terms, remission is classified as a complete cessation of the disease without ongoing treatment. In this analysis, remission was assumed to be zero despite the occurrence of ‘clinical remission’ that is emerging with treatment on biological disease-modifying antirheumatic drugs. For the purposes of estimating severity of RA in GBD terms, cases with low-disease activity on treatment would be classified as mild RA. The proportion of mild RA would be assumed to be higher in regions where early diagnosis and treatment is available. Given the small amount of information on the severity of RA, particularly over time, a change in severity in recent years in countries with access to biological drugs was unable to be captured.
Previous estimates of the global burden of RA
The previous estimates for RA were based on a small number of studies that primarily collected data from Western Europe and North America, reporting a prevalence of between 0.3% and 1%. Few studies from low-income and middle-income countries were included in these estimates as data were not available for these regions. The global burden of RA in 2004 was estimated to be 5 million DALYs, representing 0.3% of the overall global disease burden, primarily relying on data from high-income countries.1 Using the GBD 2010 Study methods, global burden of RA remained relatively stable from 2005 to 2010. In 2005, burden from RA accounted for 0.17% of total DALYs and in 2010 it accounted for 0.19% of total DALYs.
Strengths and limitations of the new estimates
The greatest strength of the study is the extensive series of systematic reviews that were undertaken to obtain data for the estimates. The reviews were completed in mid-2009 and included data up to this time. To verify if additional data were available since the initial review, MEDLINE, Pre-MEDLINE, EMBASE and CINAHL were searched for data published from 2009 to March 2013. An additional 44 titles regarding prevalence of RA were found.
The update of the systematic review to capture data published since the initial search showed overall prevalence rates in some regions that were similar to those included in the DisMod-MR modelling. However, some studies reported considerably higher rates, which may be due to the fact that these data are raw data only and have not been adjusted for the definition of RA the study used, nor methodological differences, as occurs in DisMod-MR. The inclusion of these data in future GBD studies would be helpful to determine change over time.
Despite these strengths, there were some limitations. RA has considerable impact on functional quality of life, participation and general well-being in addition to economic impact. These factors are not included in the GBD 2010 Study estimates. To gain a complete picture of the full impact of RA in a population, it is important that burden of disease estimates are supplemented with this information.
The distribution of severity of RA was based on recent population data in high-income countries. As such, there is a lack of data over time, with the current figures primarily based on treated patients, including those who may be prescribed the new biological treatments. The distribution of severity may be different in low-income and middle-income countries where access to these treatments may not be at the level of high-income countries. In addition, the data do not allow the assessment of the severity distribution over time.
RA population-based prevalence and incidence data could not be found for many countries and a number of regions and were sparse for most regions. In some instances, data were available for high-risk groups within a population, such as those who may have a genetic predisposition to the disorder; however, these were excluded as they were not representative of the entire population of that country. Consequently, in instances where data were not available for a country or region, DisMod-MR modelled the data for these regions. This raises a number of issues, including that estimates for regions with missing data may be imprecise.
Healthcare systems differ dramatically between countries and throughout continents, especially regarding non-acute events. It may be suspected that in low-income countries, where patients might not see a doctor, the prevalence and incidence data are not comparable to those in Anglo-Saxon countries, where cases are more readily identified. The data in this analysis used population-based studies that were conducted in low-income countries—primarily through the COPCORD programme (http://www.copcord.org). These studies identified cases of RA in the population through door-to-door surveys and subsequent examination and investigation where MSK cases were indicated and have formed clear incidence and prevalence figures for RA within these low-income countries. Where cases in low-income countries are not diagnosed, the prevalence of RA may be higher, and as a result the estimates presented here may in fact be an underestimate of the true global prevalence of RA.
Suggested further research
The availability of drug treatments may affect the impact of RA, both in terms of changes in disability over time and within different world regions. The availability of biological disease-modifying antirheumatic drugs, most commonly in high-income countries, may affect the DW calculated. As those receiving these treatments are likely to be considered to have ‘mild’ RA, the proportions that contribute to DW will differ between regions. Future research should assess the impact of these treatments on the severity distribution of RA in different world regions.
The future of RA is changing. While the GBD 2010 Study did not take into account the extra-articular effects of RA, these may be declining as a result of better treatment in the early stages of the disease. Declining mortality and the aging population may result in an increase in the prevalence of RA; however, this may be associated with a decline in severity due to improved treatment. In addition, cigarette smoking is associated with the occurrence of RA, and as the rate of smoking declines, RA incidence may decline.
In this recent GBD 2010 Study, self-reported RA was excluded and as a result prevalence data were not available from several countries. It could be argued that future GBD studies should include self-reported RA data, and the method of diagnosis be accounted for as a covariate in the regression modelling by DisMod-MR. In this way, data would be available for more countries, rather than data being estimated through the modelling process. However, there may be a bias in self-reported RA, in English-speaking countries at least, as the word ‘rheumatoid’ and also ‘arthritis’ are often associated with joint problems more generally and self-reporting may result in an overestimate of the prevalence of RA.
The new ACR/EULAR definition of RA, which includes early RA that may not be classified as definite RA under the 1987 ACR criteria, and which is influenced strongly by the presence of anti-citrullinated protein antibody positivity that is not universally available from population-based studies, may change the observed prevalence of RA in future studies. It may be that the earlier 1987 ACR classification criteria, not identifying early RA, may represent the severe spectrum of the disease. Future population-based studies of RA should clarify which definition was used for the collection of data.
Conclusion
Globally, RA causes significant YLD. The GBD 2010 Study did not include the effects of extra-articular symptoms associated with RA that also cause considerable disability and these may decline in treated patients. While mortality associated with MSK conditions overall increased from 1990 to 2010, mortality associated with RA decreased by 9%. Further research is needed to assess the impact of the newer medication treatments available for RA and their impact globally.
Acknowledgments
We would like to thank the following individuals who were kind enough to provide us with data upon request: Professor Freydoun Davatchi, Dr Arash Tehrani, Dr Rowsan Ara, Professor Atiqul Haq and Dr Zeinab Slim.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Handling editor Tore K Kvien
-
Contributors We declare that all authors included in this paper fulfil the criteria of authorship.
-
Funding Supported by the Bill and Melinda Gates Foundation (to DH and TV); the Australian Commonwealth Department of Health and Ageing (to ES and LM); the Australian National Health and Medical Research Council (Practitioner Fellowship to RB and Postgraduate Scholarship to DH); and the University of Sydney Institute of Bone and Joint Research (MC and ES).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Clinical and epidemiological research
- Clinical and epidemiological research
- Clinical and epidemiological research
- Clinical and epidemiological research
- Clinical and epidemiological research
- Editorial
- Clinical and epidemiological research
- Clinical and epidemiological research
- Clinical and epidemiological research
- Viewpoint