Article Text

Abstract
Objective Several prediction models for rapid radiological progression (RRP) in the first year of rheumatoid arthritis have been designed to aid rheumatologists in their choice of initial treatment. The association was assessed between RRP and disability and joint damage progression in 8 years.
Methods Patients from the BeSt cohort were used. RRP was defined as an increase of ≥5 points in the Sharp/van der Heijde score (SHS) in year 1. Functional ability over 8 years, measured with the health assessment questionnaire (HAQ), was compared for patients with and without RRP using linear mixed models. Joint damage progression from years 1 to 8 was compared using logistic regression analyses.
Results RRP was observed in 102/465 patients. Over 8 years, patients with RRP had worse functional ability: difference in HAQ score 0.21 (0.14 after adjustment for disease activity score (over time)). RRP was associated with joint damage progression ≥25 points in SHS in years 1–8: OR 4.6.
Conclusion RRP in year 1 is a predictor of worse functional ability over 8 years, independent of baseline joint damage and disease activity. Patients with RRP have more joint damage progression in subsequent years. RRP is thus a relevant outcome on which to base the initial treatment decision.
Statistics from Altmetric.com
Minimising joint damage (progression) to prevent disability is an important treatment goal of rheumatoid arthritis.1 Several prediction models have been designed to identify patients at risk of rapid radiological progression in the first year of treatment (RRP), in order to individualise initial treatment strategies.2 ,3 However, is there clinical relevance in whether or not a patient has rapid radiological damage progression? To our knowledge, it has not been investigated whether RRP is associated with functional disability in subsequent years. Therefore, we asked whether patients with RRP in year 1, defined as an increase in the Sharp/van der Heijde score (SHS) of 5 or more points,4 had worse functional ability in the first 8 years of treatment. Second, we investigated whether RRP is a predictor of subsequent joint damage progression.
Methods
Patients
All patients with radiological data at baseline and after 1 year of treatment from the BeSt cohort were analysed (465/508). Patients included in the BeSt study, a randomised controlled trial, were treated according to four treatment strategies, aimed at a disease activity score (DAS) of 2.4 or less. Initial therapy was sequential or step-up monotherapy (starting with methotrexate) or combination therapy with prednisone or with infliximab. If the DAS was 2.4 or less for 6 months or longer, medication was tapered to monotherapy. Details of the BeSt study were published previously.5
Study endpoints
To evaluate radiological progression, the SHS was used. Radiographs from baseline and year 1 were scored by two readers, blinded for patient identity and time order. The average progression score of these readers was used to classify patients as with RRP (change in SHS ≥5) or without (change <5). This threshold is similar to the smallest detectable difference (SDD) of the first study year.5 Radiological progression from years 0 to 8 was assessed by two other readers according to the same method, using radiographs of years 0–1–2–3–4–5–6–7–8. The interreader correlation coefficient was 0.96. Functional ability and disease activity were measured every 3 months using the health assessment questionnaire (HAQ) and DAS, respectively.
Statistical analysis
The HAQ score over 8 years was compared for patients with and without RRP using linear mixed models, to incorporate missing patient data, with a Toeplitz covariance structure. The estimate was adjusted for treatment group, baseline erythrocyte sedimentation rate (ESR), HAQ, SHS and the presence of rheumatoid factor (RF), anticitrullinated protein antibodies (ACPA) or both. To assess the contribution of disease activity to functional ability over time, the analysis was repeated adjusted for these variables and for DAS over time. The mean HAQ over time was calculated using these models and depicted in a graph. Because the definition of RRP was relatively arbitrary, we investigated whether patients with even more progression in year 1 would also show more disability. We divided all patients into deciles of SHS change in year 1. The lowest score of the 9th and 10th decile were 5.5 and 9.5, respectively. We used data-driven cut-offs to avoid multiple testing. HAQ over time was compared for patients with a progression score of less than 5.5 or 5.5 or greater and for patients with a progression score of less than 9.5 or 9.5 or greater, using linear mixed models as described above. To compare disease activity over time for patients with and without RRP, linear mixed models with a Toeplitz covariance structure were used. The analysis was adjusted for treatment group, baseline DAS, SHS and RF, ACPA or RF and ACPA. Adding age and gender to this model or the models with HAQ did not change the results, nor did adding an interaction term between RRP and the treatment group.
Joint damage progression from years 1 to 8 was compared for patients with and without RRP using the Mann–Whitney U test. Logistic regression analyses were then used to compare the risk of damage progression of 5 or greater (SDD) and 25 or more points (progression in the 10% of patients with highest progression scores in years 1–8), adjusted for treatment group, baseline ESR and SHS and RF/ACPA or RF and ACPA.
Results
RRP was observed in 102/465 (22%) patients. Patients with RRP were more often ACPA and RF positive and treated with initial monotherapy. Patients with RRP had a higher baseline ESR (54 vs 37 mm/h, p<0.001) and C-reactive protein (60 vs 31, p<0.001). They had worse functional ability (HAQ 1.5 vs 1.4, p=0.04) and more radiological damage: median baseline SHS 5.8 versus 1.5, p<0.001 (table 1). The number of treatment steps patients had failed on and the number of patients failed on all protocol steps after 8 years was higher in patients with RRP, p=0.001 and p<0.001. At year 8, 133/465 patients were lost to follow-up: 29% of patients without RRP, 27% of patients with RRP, p=0.6. Differences in baseline characteristics for patients with and without radiological progression of 9.5 or greater in year 1 were comparable with these results (see supplementary table S1, available online only).
Baseline characteristics of patients with and without RRP after 1 year of DAS-steered treatment
Functional ability
Over 8 years, there was a statistically significant difference (0.21; 95% CI 0.10 to 0.33) in the HAQ score for patients with and without RRP (figure 1). For groups 1 and 2 the difference was 0.20 (0.05 to 0.34), for groups 3 and 4 is was 0.27 (0.08 to 0.45). DAS over time in RRP patients was also higher than in non-RRP patients: difference 0.33 (95% CI 0.18 to 0.48) (see supplementary figure S1, available online only). After adjustment for DAS over time, the difference in the HAQ score was statistically but not clinically significant: 0.14 (95% CI 0.05 to 0.24). The difference in the HAQ score between the 10% of patients with the highest progression score in year 1 and the other 90% was 0.27 (95% CI 0.12 to 0.41), 0.20 (95% CI 0.08 to 0.33) after adjustment for DAS over time. The difference in the HAQ score for patients with and without damage progression of 5.5 or greater (top 20% of progression scores vs the other 80%) was 0.15 (95% CI 0.06 to 0.25) after adjustment for DAS over time.

Mean health assessment questionnaire score (HAQ) over 8 years for patients with and without rapid radiological progression (RRP) Sharp/van der Heijde score (SHS) of 5 or greater in year 1 (RRP) (A) and for patients with progression less than 9.5 or 9.5 or more points in year 1 (B), adjusted for baseline HAQ, treatment strategy, baseline erythrocyte sedimentation rate and SHS and the presence of rheumatoid factor and/or anticitrullinated protein antibodies (using linear mixed models, which take into account missing patient data).
Joint damage
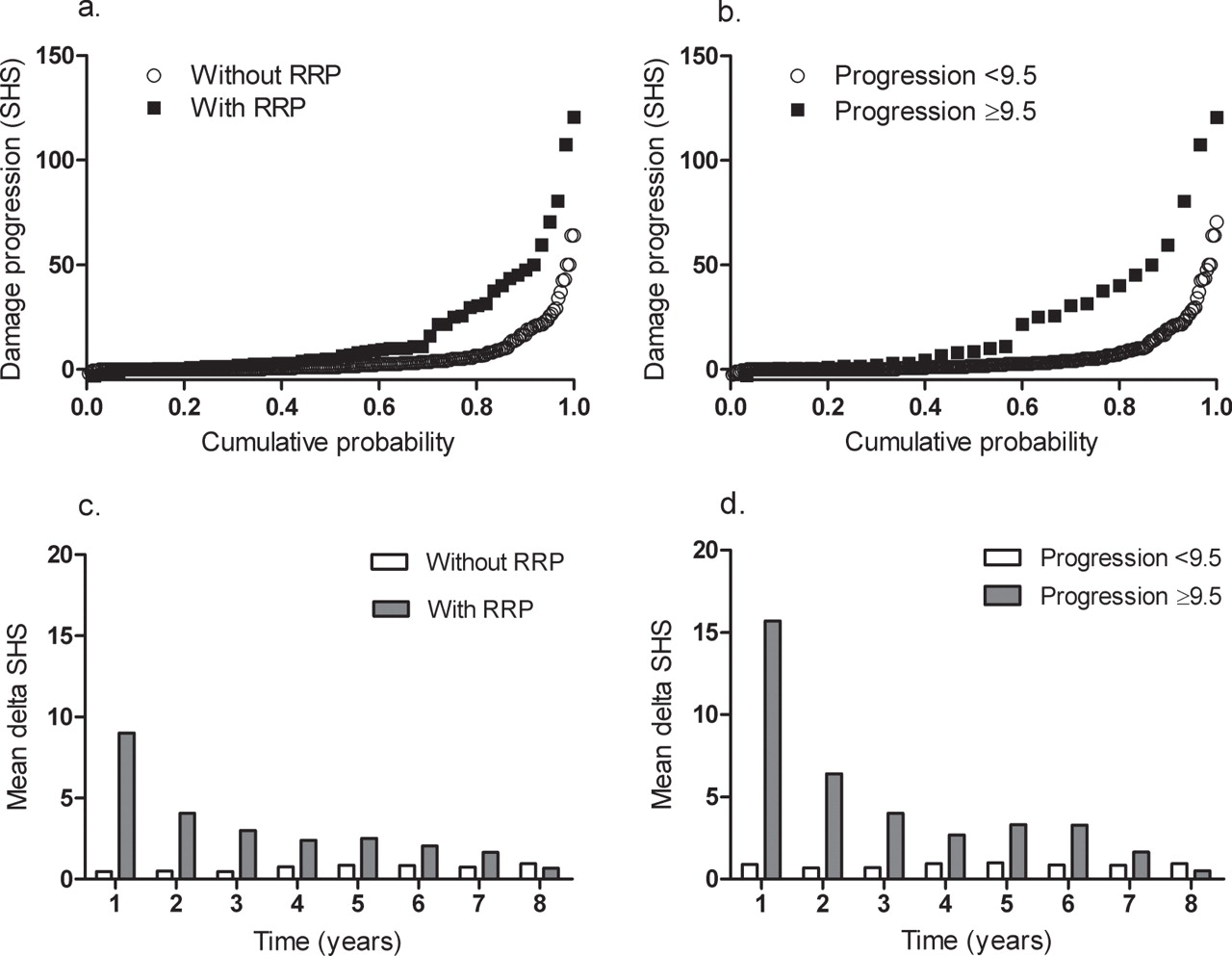
Patients with RRP in year 1 had more joint damage progression in years 1–8 (figure 2), with a median progression score of 5.0 (IQR 1.5–25.3) compared with 1.0 (IQR 0.0–5.0) for patients without RRP (p<0.001). The OR of 5 or more points progression was 2.0 (95% CI 0.96 to 4.2). Patients with RRP had an increased risk of damage progression of 25 units or greater in years 1–8: OR of 4.6 (95% CI 1.6 to 12.7). Of the patients without RRP, 5% had more than 25 units progression in years 1–8. The mean yearly progression score was never higher than the SDD (5) in either group.
{kind=link}
{kind=link}
Joint damage progression in years 1–8 and yearly joint damage progression over time for patients with and without rapid radiological progression (RRP) Sharp/van der Heijde score of 5 or greater in year 1 (RRP) (A and C), and for patients with less than 9.5 or 9.5 or more points progression in year 1 (B and D) n (no RRP/RRP) year 1: 363/102; year 2: 326/85; year 3: 305/81; year 4: 296/82; year 5: 272/78; year 6: 236/64; year 7: 221/61; year 8: 216/61.
When comparing the 10% of patients with the highest progression score in year 1 with the other 90% (cutoff 9.5), similar results were seen for progression of 5 or greater in years 1–8: OR 1.8 (95% CI 0.7 to 4.5). The risk of being in the top 10% of progression scores again in years 1–8 (progression ≥25) was higher: OR 6.6 (95% CI 2.2 to 19.8). The median progression score in year 1 in these patients was 15.5 points SHS (IQR 12.5–22.0).
Discussion
RRP, defined as an increase of 5 or more points in SHS in the first year of treatment, is associated with worse functional ability in later years and more radiological damage progression. This can only be partly explained by higher disease activity in these patients. Our results show that RRP is a clinically relevant outcome to be used in prediction models that can help choose the best initial treatment for patients with newly diagnosed rheumatoid arthritis.
The impact of RRP with this threshold on functional ability is relatively small. Based on an estimated minimally important difference of the HAQ score of 0.20–0.24,6 the statistically significant difference in HAQ over 8 years explained by RRP, not disease activity, was not clinically relevant. This is probably because the follow-up period of 8 years is still short. More importantly, after the first 1–2 years yearly damage progression in all patients is much lower and shows a tendency to decrease with time (figure 2C,D). This is most likely due to the continuous 3-monthly DAS 2.4 or less steered treatment adjustments in the BeSt cohort, resulting in low disease activity in the vast majority of patients. Still, yearly progression in patients with RRP continues to be higher than in patients without RRP, who hardly progress at all. We found that patients with RRP have an increased risk of subsequent joint damage progression. Combined with the effect of ageing,7 after a longer follow-up period, this continuous damage progression may lead to significantly more functional disability.
Our results also show that the 10% of patients who had an increase of 9.5 or more points SHS in the first year have even worse functional ability after 8 years. We found a clinically meaningful difference in the mean HAQ score between these 10% and the other patients after adjustment for disease activity over time.
In conclusion, RRP in the first year of treatment is an independent predictor of later functional disability, and thus not only a radiologically but also a clinically relevant early outcome on which to base the initial choice of treatment. This may mean that, as earlier studies have shown,2 ,3 patients with a low risk of RRP require less intensive initial therapy to prevent radiological damage progression than patients with a high risk, provided that this therapy offers early symptom relief and provided treatment remains ‘treat to target’.
Acknowledgments
The authors would like to thank all patients as well as the following rheumatologists (other than the authors) who participated in the Foundation for Applied Rheumatology Research (all locations are in The Netherlands): W M de Beus (Medical Center Haaglanden, Leidschendam); C Bijkerk (Reinier de Graaf Gasthuis, Delft); M H W de Bois (Medical Center Haaglanden, The Hague); H Boom (Spaarne Hospital, The Hague); M de Buck (Medical Center Haaglanden, Leidschendam); G Collée (Medical Center Haaglanden, The Hague); J A P M Ewals (Haga Hospital, The Hague); A H Gerards (Vlietland Hospital, Schiedam); R J Goekoop (Haga Hospital, The Hague); B A M Grillet (Zorgsaam, Terneuzen); J H L M van Groenendael (Franciscus Hospital, Roosendaal); K H Han (Medical Center Rijnmond-Zuid, Rotterdam); M V van Krugten (Admiraal de Ruyter Hospital, Vlissingen); L Lard (Medical Center Haaglanden, Leidschendam); H van der Leeden (retired); W F Lems (VUMC, Amsterdam); M F van Lieshout-Zuidema (Spaarne Hospital, Hoofddorp); P A H M van der Lubbe (Vlietland Hospital, Schiedam); C Mallée (Kennemer Gasthuis, Haarlem); E T H Molenaar (Groene Hart Hospital, Gouda); M van Oosterhout (Groene Hart Hospital, Gouda); A J Peeters (Reinier de Graaf Gasthuis, Delft); N Riyazi (Haga Hospital, The Hague); H K Ronday (Haga Hospital, The Hague); A A Schouffoer (Groene Hart Hospital, Gouda); P E H Seys (retired); P B J de Sonnaville (Oosterschelde Hospital, Goes); I Speyer (Bronovo Hospital, The Hague); K S S Steen (Kennemer Gasthuis, Haarlem); G M Steup-Beekman (Bronovo Hospital, The Hague); J Ph Terwiel (retired); A E Voskuyl (VU Medical Center, Amsterdam); M L Westedt (Bronovo Hospital, The Hague); S ten Wolde (Kennemer Gasthuis, Haarlem); D van Zeben (Sint Franciscus Gasthuis, Rotterdam). The authors would also like to thank all other rheumatologists and trainee rheumatologists who enrolled patients in this study, and all research nurses for their contributions.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Funding The study was designed by the investigators and supported by a government grant from the Dutch College of Health Insurance Companies, with additional funding from Janssen BV and Schering-Plough.
-
Competing interests None.
-
Ethics approval This study was approved by the medical ethics committees of all participating centers.
-
Provenance and peer review Not commissioned; externally peer reviewed.