Article Text

Abstract
Objective To determine the magnitude of the risk of incident cardiovascular disease (CVD; fatal and non-fatal), including acute myocardial infarction (MI), cerebrovascular accidents (CVA) and congestive heart failure (CHF), in patients with rheumatoid arthritis (RA) compared to the general population through a meta-analysis of controlled observational studies.
Methods The authors searched the Medline, Embase, LILACS and Cochrane databases from their inception to June 2011. Observational studies meeting the following criteria were included: (1) prespecified RA criteria; (2) predefined CVD criteria for incident CVD (MI, CVA or CHF); (3) a comparison group; and (4) RR estimates, 95% CI or data for calculating them. The authors calculated the pooled RR using the random-effects model and tested for heterogeneity using the bootstrap version of the Q statistic.
Results Fourteen studies comprising 41 490 patients met the inclusion criteria. Overall, there was a 48% increased risk of incident CVD in patients with RA (pooled RR 1.48 (95% CI 1.36 to 1.62)). The risks of MI and CVA were increased by 68% (pooled RR 1.68 (95% CI 1.40 to 2.03)) and 41% (pooled RR 1.41 (95% CI 1.14 to 1.74)). The risk of CHF was assessed in only one study (RR 1.87 (95% CI 1.47 to 2.39)). Significant heterogeneity existed in all main analyses. Subgroup analyses showed that inception cohort studies were the only group that did not show a significantly increased risk of CVD (pooled RR 1.12 (95% CI 0.97 to 1.65)).
Conclusions Published data indicate that the risk of incident CVD is increased by 48% in patients with RA compared to the general population. Sample and cohort type influenced the estimates of RR.
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease that is associated with an increased risk of mortality.1 ,2 Recent evidence has demonstrated that the increased risk is largely attributable to cardiovascular disease (CVD). Overall, RA increases the risk of cardiovascular (CV) mortality by up to 50%.3 This excess risk mainly reflects higher rates of death from ischemic heart disease and cerebrovascular accidents (CVA) observed among patients with RA. Since an association between chronic inflammation and atherosclerosis has been established,4,–,7 several studies have examined the relationship between RA and specific CV events, including myocardial infarction (MI),8,–,12 CVA10 ,11 ,13,–,17 and congestive heart failure (CHF).18 However, several studies have observed a significantly increased incidence of MI but not of CVA,10 ,11 suggesting that RA may have a differential effect on the vasculature of the brain and heart. The increased risk of CVD in RA seems to be independent of traditional risk factors (eg, hypertension, diabetes).15 Patients with RA have a substantially increased risk of 30-day case death following MI but not stroke, compared with patients without RA.19 Furthermore, in a previous study, we found that glucocorticoid use increases the risk of MI20 but not of CVA.21
Previous studies that evaluated the risk of incident CV events in RA have shown that factors such as cohort type, disease duration, length of follow-up and incident versus prevalent cohorts seem to influence the association between RA and CVD.1 ,3 ,22
Our objective was to conduct a meta-analysis of published observational studies to determine the magnitude of the risk of incident CVDs combined (fatal and non-fatal), as well as cause-specific incidence from MI, CVA and CHF in patients with RA compared to the general population.
Materials and methods
Search strategies
The Medline, Embase, LILACS and Cochrane databases were searched by an experienced librarian from their inception (1966, 1980 and 1982, respectively) to June 2011 to identify published studies and reviews in the field of CVD in RA. The following search terms were used alone and in combination: RA, CVD, CVA, risk, risk factors, mortality, comorbidity, causality, cause of death, heart death, cohort study, case–control study and longitudinal study. The authors also hand-searched the reference lists of text books and key articles retrieved for additional references.
We selected peer-reviewed articles (case–control and cohort studies) that met the following inclusion criteria: (1) predefined RA criteria; (2) predefined CVD criteria for incident (first ever event per person) CVD (MI, CVA or CHF); (3) RR estimates, 95% CI or data for calculating them; and (4) a comparison group. We only included studies where patients with RA had no history of CVD prior to RA onset. Furthermore, only the first CV event during follow-up was considered. If data from a single study were reported in more than one article, only the results from the most recent study were included in the meta-analysis.
Data extraction
Two researchers (JAA-Z and DL) independently assessed studies for eligibility and extracted data on year of publication, type of study, source of the RA sample, RA definition, sample size, enrolment period, RA duration at study entry, mean time of follow-up, extent of loss to follow-up, reference group, outcome definition, number of observed and expected CV events for all patients by gender if available, and matching or adjustment for CV risk factors. Any differences among the two authors were discussed until consensus was reached.
Quality scores of included studies
We assessed study quality based on a 12-point scale that included elements of previously published scales for observational studies,23 ,24 which was also used in our previously published meta-analysis of CV mortality in RA.3 Each study was scored according to six characteristics related to its patient sample and methods. Each item was scored as 0, 1 or 2. Specifically, we determined the source of the patient sample (community-based: 2, clinic-based: 1, undefined: 0); cohort type, if applicable (inception: 2, non-inception: 1); RA definition (use of American College of Rheumatology classification criteria for RA25: 2, other validated criteria: 1, other predefined but non-validated criteria: 0); ascertainment of CVD outcome (validated criteria (eg, Framingham diagnostic criteria): 2, non-validated but clearly defined criteria (eg, international classification of diseases): 1, not mentioned: 0); extent of loss to follow-up (<20%: 2, 20–40%: 1, >40%: 0); and matching by or adjustment for Framingham risk factors (≥5 risk factors: 2, <5 risk factors: 1, none: 0). For stratification purposes, studies that scored 10 or more were considered to be of higher quality, and the rest were considered to be of lower quality. Quality scoring was performed independently by two reviewers (JAA-Z and DL). Disagreement was resolved by consensus.
Statistical analysis
We calculated weighted–pooled summary estimates of relative risks (pooled RR) for all CVDs combined, as well as for each disease individually (MI, CVA and CHF). The pooled RR represents a summary estimate of the increased risk of CVD in patients with RA compared to the general population, weighted by a factor that is influenced by the sample size of each study. Separate pooled RRs were calculated for men and women when data were available. Calculations were performed on the log of RR from the individual studies, and the resulting pooled values were then transformed back to the RR scale. We used the random-effects model and tested for heterogeneity using the bootstrap version of the Q statistics and Stata statistical software V. 10.0.26
Because heterogeneity is expected in meta-analyses of observational studies, subgroup analyses were carried out to assess the degree and source of such heterogeneity. Studies were stratified based on patient sample (community-based versus clinic-based), cohort type (inception versus non-inception), design (cohort versus case–control studies), case ascertainment (American College of Rheumatology criteria versus others) and quality score (<10 vs ≥10). Statistical inferences about the difference in pooled RR between subgroups of studies were performed using a multivariate meta-regression analysis that evaluated the adjusted effect of the above study characteristics on the pooled log RR.
Robustness of the results was evaluated using jackknife sensitivity analysis, that is, the analysis was repeated multiple times, each time with removal of a single study from the baseline group of studies.27
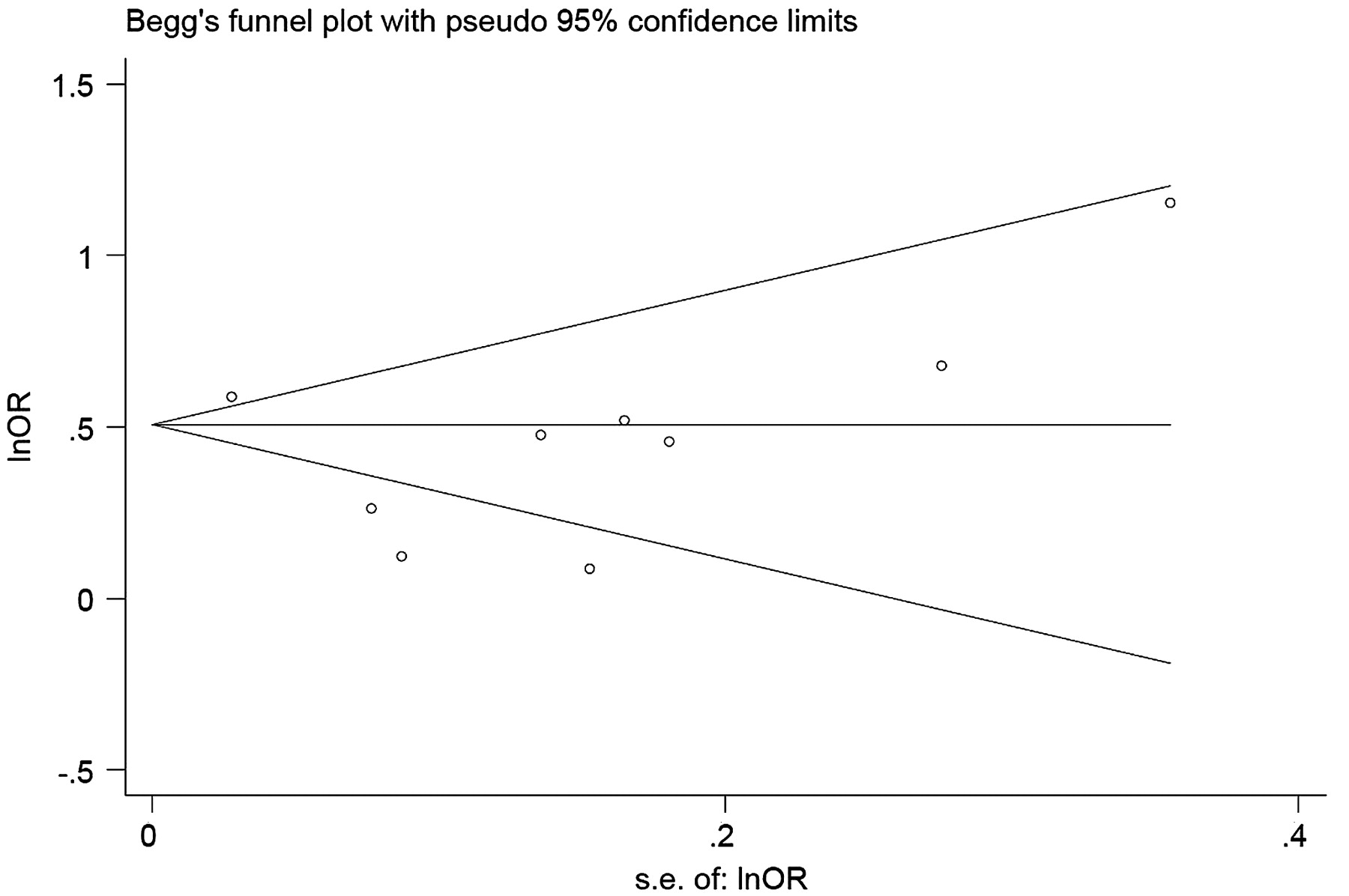
To detect the presence of publication bias (ie, the bias resulting from the greater likelihood of publication of studies reporting positive results) or small-study effect (the tendency for treatment effect estimates in small studies to differ from those in larger studies),28 we constructed a funnel plot, in which a measure of the study size is plotted as a function of the measure of interest.29 If publication bias and small-study effect are absent, the distribution of the data points will be symmetrical. In addition, Egger's regression test was used to provide an objective quantitative test statistic (p value) for the presence of asymmetry in the data.30
Results
Overall risk of CVD
We screened 841 abstracts published over the last 45 years (figure 1). We identified 16 studies (two were repeated studies on the same sample) evaluating the risk of MI, CVA or CHF and comprising a total of 41 490 patients with RA, with 3155 CV events8 ,10,–,18 ,31,–,35 (table 1).

Flow diagram of study selection.
Characteristics of the 14 studies included in the meta-analysis to assess the risk of new cardiovascular events in patients with RA
Nine studies (n=39 901 RA cases with 2047 CV events) assessed the overall risk of CVD, and four studies also reported risks by gender (figure 2). Overall, the risk of incident CVD was significantly increased by 48% in patients with RA compared to the general population (pooled RR 1.48 (95% CI 1.36 to 1.62)). Among the studies that reported the stratified results by gender, the risk increased similarly in both genders (female: pooled RR 1.50 (95% CI 1.24 to 1.80); male: pooled RR 1.53 (95% CI 1.38 to 1.70)).

Meta-analysis of studies on overall and cause-specific cardiovascular diseases in patients with rheumatoid arthritis.
We identified significant heterogeneity among studies (Q=25.6, p=0.001). Subgroup analyses showed that a number of factors influenced CVD risk (table 2).
Overall risk of CVD and sensitivity analysis for the nine studies assessing combined CVDs in patients with rheumatoid arthritis
Overall, pooled RRs were higher in studies with lower-quality scores (<10), studies from clinic-based samples and non-inception cohorts. The two inception cohorts8 ,17 were the only studies that did not show an increased overall risk of CVD (combined events) among patients with RA even after pooling data from both studies (pooled RR 1.12 (95% CI 0.97 to 1.30)). Despite the observed differences in CVD risk among subgroups, only cohort type was significantly associated with the observed heterogeneity in the meta-regression analysis (p=0.009). Results of the jackknife sensitivity analysis for all CV events combined suggested that the results were robust (table 3).
Sensitivity analysis using a jackknife approach whereby each study is removed individually to test the robustness of the pooled RR
The pooled RR remained significantly increased when studies were excluded one at a time, with the pooled RR ranging from 1.47 to 1.55 and with the corresponding 95% CI bounds remaining above 1. Funnel plot showed some asymmetry, as there seemed to be a dearth of studies with high precision (large sample size) and large RR (these studies would occupy the northeastern part of the plot) (figure 3). Nevertheless, the result of Egger's regression test for asymmetry was not significant (p=0.32).
{kind=link}
{kind=link}
{kind=link}
Funnel plot of nine studies evaluating the risk of cardiovascular disease in patients with rheumatoid arthritis compared to the general population. Each dot represents individual studies. The horizontal line is the random-effects pooled estimate of log (RR).
Myocardial infarction
We identified 10 studies with 3178 patients with RA that assessed the risk of MI.8 ,10,–,12 ,14,–,17 ,31 ,33 Two studies12 ,16,–,18 used the same sample; therefore, the more recent publication was included.12 ,33 Overall, there was a 68% increase in the risk of MI in patients with RA (pooled RR 1.68 (95% CI 1.40 to 2.03)), as shown in figure 2. Six studies reported on the risk of MI according to gender.8 ,10,–,12 ,31 ,34 The risk of MI was significantly increased in both women (pooled RR 1.93 (95% CI 1.64 to 2.27)) and men (pooled RR 1.67 (95% CI 1.18 to 2.36)).
Cerebrovascular accident
We identified seven studies with 39 520 patients with RA that assessed the risk of CVA10 ,11 ,14,–,17 ,31 (figure 2). Overall, there was a 41% increase in the risk of CVA in patients with RA (pooled RR 1.41 (95% CI 1.14 to 1.74)). Five studies reported estimates according to gender.8 ,10 ,11 ,16 ,31 The risk of CVA was significantly increased in both women with RA (pooled RR 1.29 (95% CI 1.12 to 1.48)) and men with RA (pooled RR 1.36 (95% CI 1.21 to 1.53)).
Congestive heart failure
We identified only one study that evaluated the risk of CHF.18 Overall, there was an 87% increase in the risk of CHF in patients with RA when compared to non-RA cases (RR 1.87 (95% CI 1.47 to 2.39)). However, the risk was only significantly increased in patients who tested positive for rheumatoid factor (RR 2.59 (95% CI 1.95 to 3.43)) but not in patients who tested negative for rheumatoid factor (RR 1.28 (95% CI 0.93 to 1.78)).
Discussion
This is the first systematic review and meta-analysis of published observational studies assessing the risk of incident CVD in patients with RA. We found that there was a 48% increased risk of first ever CV events in patients with RA compared to the general population. The excess risk was due to an increased risk of MI (68%), CVA (41%) and CHF (70%). The risks of MI and CVA were increased in both genders. The risk of CHF was increased only in patients who tested positive for rheumatoid factor based on the only study assessing this outcome.
All but two studies evaluating MI found an increased risk in RA. In contrast, most studies on CVA did not find an increased risk of CVA in RA. However, large studies tended to report a positive association between RA and CVA, which caused a significant association after pooling them. This suggests a lack of power due to an insufficient number of CVA events in smaller studies, or a weaker association between RA and CVA than between RA and MI. A recent nationwide study based on approximately 10 000 patients with RA (published after the literature search period of the current meta-analysis) found an increase in the risk of MI that was similar to our pooled estimate (70% increased risk).36 In this study, the risk of MI in patients with RA was similar to the risk of MI in patients without RA who were 10 years older. This may suggest that patients with RA age at a faster rate than the general population and experience CVD at an earlier age.
In a previous meta-analysis on the risk of CV mortality, we found that estimates for CV mortality varied among the primary studies, depending on the sample and cohort type.3 ,22 Risks were lower than and rates of CV mortality were closer to those of the general population in studies with community-based and inception cohorts than in studies with clinic-based or non-inception cohorts. We observed similar findings in the current meta-analysis. Van Doornum et al19 demonstrated that patients with RA had an increased 30-day CV mortality with respect to non-RA cases. Collectively, this evidence suggests that individuals with RA have a higher risk of developing new CV events at an earlier age and a higher case death.
Therefore, as recently proposed by the European League Against Rheumatism,37 focus on CVD risk prevention in RA should be included in rheumatological care. In addition, aggressive primary CVD prevention should be part of the standard of care in patients with RA. Longitudinal studies assessing management strategies and their impact on patients with RA are warranted.
Our study has some limitations. We included cohorts with different clinical settings, diagnostic criteria, age at enrolment, period at risk and study design. As expected, we found statistically significant heterogeneity in the results. As recommended, we used the random-effects model to include an estimate of variability.38 We found that cohort type (inception versus non-inception) explained some of the observed heterogeneity. Of interest, inception cohorts were the only studies that did not find a statistically significant increase in the risk of incident CVD. We believe that this is likely due to a shorter RA duration upon their entry into the study, overall less disease severity and shorter follow-up than non-inception RA studies. All of these factors influence the risk of CVD in patients with RA, as eloquently discussed by Ward.1 Visual inspection of the funnel plot indicated a potential lack of studies with large sample sizes, which also reported a largely increased RR (a manifestation of the small-study effect). The associated Egger's regression test did not reveal this effect, but this might be due to the relatively small number of studies and the resulting lack of power in the test.
In summary, our meta-analysis of published observational studies indicates that people with RA have a 48% (pooled RR 1.48 (95% CI 1.36 to 1.62)) increased risk of incident CVD when compared to the general population. Also, people with RA have a 68% (pooled RR 1.68 (95% CI 1.40 to 2.03)), 41% (pooled RR 1.41 (95% CI 1.14 to 1.74)) and 87% (RR 1.87 (95% CI 1.47 to 2.39)) increased risk of MI, CVA and CHF, respectively, when compared to the general population. Finally, the increased overall risk of CVD, as well as the increased risks of MI and CVA, is similar between genders. The risk of CHF was increased only in women with RA, but further research in this area is needed given that only one study has been published to date.
Acknowledgments
The authors would like to acknowledge Kathy Hornby and Jenny Leese for performing the literature search and for editing the manuscript, respectively.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.