Article Text

Abstract
Objectives The performance of spondyloarthritis (SpA) classification criteria is not well-established in general early arthritis cohorts. Therefore, the authors tested their performance in the Leiden Early Arthritis Clinic (EAC) cohort and assessed whether these criteria can assist rheumatologists in diagnosing patients.
Methods The authors identified all SpA and psoriatic arthritis (PsA) patients in the EAC cohort according to the diagnosis of the treating rheumatologist. A control group consisting of arthritis patients with other diagnoses was matched to the SpA and PsA patients on gender, age and symptom duration. The authors assessed the fulfilment of SpA criteria in all three groups.
Results Of the patients in the EAC cohort (n=2011), 7.5% was diagnosed with PsA and 3.8% with SpA. In the PsA group, the ClASsification criteria for Psoratic ARthritis (CASPAR) criteria had the highest sensitivity (88.7%). In the SpA group, the Assessment of SpondyloArthritis international Society (ASAS) peripheral SpA and European Spondylarthropathy Study Group (ESSG) criteria had the highest sensitivity (both 48.7%). Specificity of all criteria sets was good: ranging from 88.5% (ESSG) to 100% (Amor).
Conclusions In early arthritis, sensitivity of SpA classification criteria is modest except for the CASPAR criteria in PsA. However, specificity of classification criteria, including the new ASAS-peripheral SpA criteria, is high.
Statistics from Altmetric.com
Introduction
Early recognition of spondyloarthritis (SpA) is challenging since the concept of SpA comprises a heterogeneous group of diseases.1 Over the years, several classification criteria have been developed. The European Spondylarthropathy Study Group (ESSG) criteria and the Amor criteria were developed to classify patients with all subtypes of SpA.2 ,3 Recently, two new sets were developed by the Assessment of SpondyloArthritis International Society (ASAS) to distinguish between patients with predominantly axial SpA (axSpA) and with predominantly peripheral SpA (pSpA).4 ,5 Furthermore, the ClASsification criteria for Psoriatic ARthritis (CASPAR), is a classification set especially for psoriatic arthritis (PsA).6
The performance of all classification criteria was good when tested in the original validation population, frequently with longstanding symptoms.2 ,3 ,6,–,8 The performance was less known in general early arthritis cohorts like the Leiden Early Arthritis Clinic (EAC) cohort. It is known that 67% of the SpA-patients with a disease duration <2 years report arthritis as the first symptom.9 So, in an EAC, SpA and PsA are important parts of the differential diagnosis. Therefore, it is important to test the performance of classification criteria in early disease cohorts.
First, we described the prevalence of SpA and PsA among patients presenting with peripheral arthritis in the Leiden EAC cohort. Thereafter, we tested the performance of the described classification criteria and investigated whether these criteria sets can assist rheumatologists in diagnosing patients with peripheral arthritis.
Methods
Patients
Data from the Leiden EAC cohort were used; a population-based prospective cohort including patients with recent-onset arthritis. Since 1993, general practitioners in the Leiden area referred patients with suspected arthritis as quickly as possible to the rheumatology department of the Leiden University Medical Centre to detect and treat inflammatory disorders early. Patients with an objective evidence of arthritis, with a symptom duration <2 years and a signed informed consent, were included.10
A database was built consisting of, among others: medical history, physical examination and laboratory tests according to the EAC protocol. Besides these parameters, individual patients' charts were reviewed for additional extra-articular SpA features (past and/or present), necessary to apply the criteria sets (online supplementary table S1). Furthermore, in all patients, human leucocyte antigen (HLA)-B27 typing was performed if possible. All collected data (baseline to 1 year) was used for analysis. The diagnosis of the treating rheumatologist recorded from a list of proposed diagnoses including PsA and SpA after 1 year served as the gold standard.
Between 1 February 1993 and 1 February 2009, 2011 patients with early arthritis were included in the EAC cohort. All PsA and SpA patients, according to the treating rheumatologist (n=226) at 1-year follow-up visit, were included in the present analysis.
In the SpA group, 13 patients dropped out after 3 months; in the PsA group, 8 patients; and in the control group 36 patients. Of these patients, we used all available data which is until the third visit after 3 months.
Furthermore, a control group (n=226) was selected from the EAC cohort, matched to the combined SpA-PsA group on gender, age and symptom duration (p=0.978, p=0.637 and p=0.03, respectively). Thereafter, the combined SpA-PsA group was split into the SpA group and PsA group. The control group included patients with the following diagnoses at 1 year: 82 with rheumatoid arthritis (1987-ACR criteria); 60 with undifferentiated arthritis; 13 with post-streptococcal reactive arthritis; 12 with osteoarthritis; 8 with gout; 15 with sarcoidosis; and 26 patients with other diagnoses like palindromic arthritis and post-traumatic arthritis.
Data analysis
Baseline characteristics of the three groups (SpA, PsA and control group) were analysed using t-tests and χ2 tests.
For each patient with SpA or PsA, we assessed the fulfilment of the criteria sets and compared this with the fulfilment of the criteria in patients in the control group using cross-table analysis. Missing values for the presence of SpA features were interpreted as being absent. The checked diagnosis after 1 year was used as the gold standard.
Furthermore, the performance of the various criteria sets was determined by calculating sensitivity, specificity, positive likelihood ratio (LR+), and negative likelihood ratio (LR−). All analyses were performed using SPSS V. 17.0; p values <0.05 were considered significant.
Results
Patient characteristics during the first year of inclusion
Of the 2011 patients included in the EAC cohort, 150 (7.5%) were diagnosed with PsA and 76 (3.8%) with SpA.
The control group was matched to the combined group of patients with SpA and PsA on gender, age and symptom duration. After splitting the patients into the SpA group and PsA group, differences with the control group were observed. The mean age of the SpA group was significantly lower (p<0.001), and of the PsA group significantly higher (p=0.03) compared with the control group. In the SpA group, 55 (72.3%) patients, in the PsA group, 64 (42.6%) patients, and in the control group, 121 (53.5%) patients were diagnosed before the age of 45 years.
Moreover, patients within the SpA group with a preceding infection had a significantly shorter self-reported symptom duration (6.4 (SD 9.4) vs 22.1 (SD 27.9) weeks; p<0.001), while patients without a preceding infection in the SpA group and PsA patients had a longer duration than patients in the control group (30.3 (SD 42.6) and 35.5 (SD 58.0) weeks; p=0.10 and p=0.01, respectively).
In the SpA group, all patients had at least one other SpA feature in addition to arthritis. In the control group, 66.4% of the patients had 1 or 2, and 22.1% had 3 or more SpA features in addition to the arthritis, while in the PsA group and SpA group, respectively, 16.0% and 21.0% had 1 or 2 SpA features, and 82.7% and 79.0% of the patients had 3 or more SpA features (see online supplementary figure S1).
The most frequently reported SpA features in the PsA group were psoriasis (94.0%), positive family history (89.2%) and dactylitis (36.7%). The PsA group differed significantly from the control group on these SpA features, and on a higher prevalence of enthesitis, HLA-B27 positivity and rheumatoid factor (RF) negativity. By contrast, inflammatory back pain was significantly less frequent, and C reactive protein levels significantly lower in the PsA group than in the control group. In the SpA group, HLA-B27 positivity (47.5%), positive family history (47.4%) and preceding infection (36.8%) were the most frequent SpA features. SpA patients differed significantly from the control group on these features and on the presence of inflammatory back pain, enthesitis, uveitis, inflammatory bowel disease, negative RF and elevated erythrocyte sedimentation rate levels (table 1).
Baseline characteristics
Performance of classification criteria
In the PsA group, 133 patients fulfilled the CASPAR, and 78 the ASAS-pSpA criteria, (sensitivity of 88.7% and 52.0%, respectively). In the SpA group, 37 patients fulfilled the ASAS-pSpA and ESSG criteria each, (sensitivity both 48.7%). Specificity of all criteria sets was good, ranging from 88.5% (ESSG criteria) to 100% (Amor criteria). In the PsA group, LR+ and LR− of the CASPAR criteria were the best (20.04 and 0.12). In the SpA group, the best LR+ was identified for the ASAS-aSpA criteria, and the best LR− was identified for the ASAS-pSpA criteria (7.3 and 0.57, respectively) (table 2).
Number of patients fulfilling the various criteria sets and performance of the various criteria sets
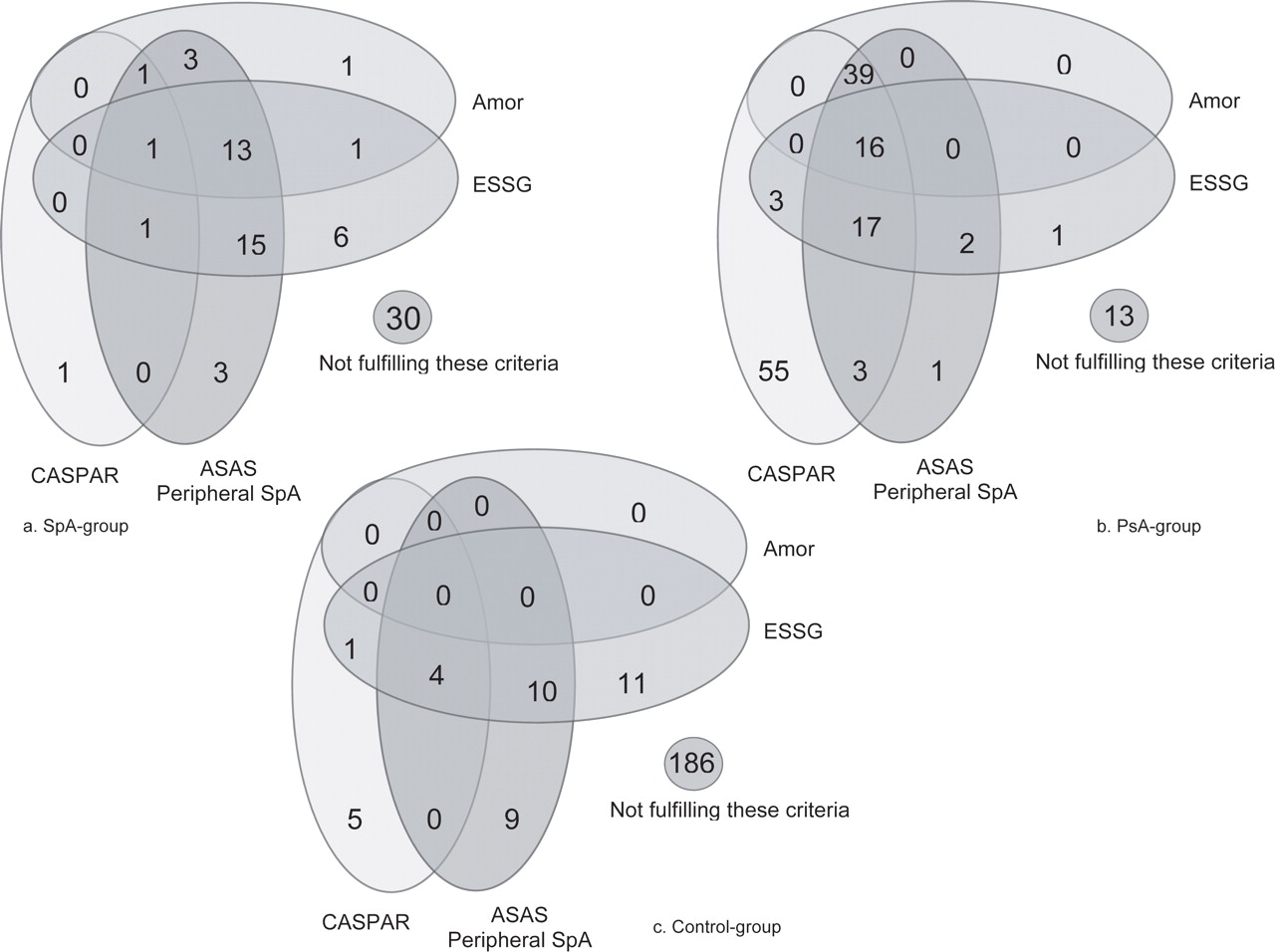
In the control group, 186 patients (82.3%) did not fulfil any of the four classification criteria, and 13 (8.7%) in the PsA group and 30 patients (39.5%) in the SpA group. The overlap of the criteria is presented in figure 1. In the PsA group, 16 patients fulfilled all four criteria sets and 39 fulfilled the combination of Amor, ASAS-pSpA and CASPAR criteria. Also in the SpA group many patients fulfilled at least two criteria sets (1 patient fulfilled all four criteria, 13 the combination of ASAS-pSpA, ESSG and Amor, and 15 the combination of ASAS-pSpA and ESSG criteria). In contrast in the control group, very few patients fulfilled more than one criteria set, and none of them all four criteria.
{kind=link}
Venn diagram representing the number of patients from the Leiden Early Arthritis Clinic meeting different criteria for spondyloarthritis. ESSG, European Spondylarthropathy Study Group; ASAS, Assessment of SpondyloArthritis International Society; CASPAR, ClASsification criteria for Psoriatic ARthritis in the SpA group (a), in the PsA group (b) and in the control group (c)
Furthermore, the concordance between the CASPAR and ASAS-pSpA criteria was calculated. In the PsA group, 75 patients fulfilled both the CASPAR and the ASAS-pSpA criteria, 58 patients fulfilled the CASPAR criteria and 3 fulfilled the ASAS-pSpA criteria only (59.3% agreement). Only 3 patients in the SpA group fulfilled both the CASPAR and the ASAS-pSpA criteria, 34 fulfilled the ASAS-pSpA criteria only, and one patient fulfilled the CASPAR criteria only (53.9% agreement).
Discussion
More than 10% of the patients in the EAC cohort were diagnosed with PsA or SpA. Unquestionably, this discovered prevalence is not representative for the whole concept of SpA among patients referred to rheumatologists since this cohort does not include patients with dactylitis or enthesitis, or patients with predominantly axSpA (back pain).
The sensitivities found in this report are lower for all criteria sets than the reported sensitivities as tested in the original cohorts with established disease patients.2,–,4 ,6 ,8 A different patient selection in the EAC cohort compared with the original cohorts can explain this difference. The EAC cohort consists of patients with early arthritis, while the original cohorts included patients with various presenting features, not only arthritis, and a longer symptom duration. The longer the symptom duration, the more chance that (extra-articular) features develop.
Except for these issues related to symptom duration there are also factors related to more specific characteristics of the criteria sets. The sensitivity of the ESSG criteria may be limited by the lack of HLA-B27 in the list of SpA features. The poor sensitivity of the Amor criteria in the EAC cohort may also partially be explained by the strict definition of peripheral arthritis as oligoarthritis (2–4 joints). Besides, to fulfil the Amor criteria, at least six points are necessary corresponding to 3–4 items. Since some of these items are more seen in axSpA patients, this seems quite difficult to reach for patients with peripheral manifestations only.5 Although it was expected that the sensitivity was lower than reported in the original cohorts it may also indicate that it is difficult to cover all pSpA-patients according to rheumatologists by existing criteria in recent onset disease, which confirms that these criteria are classifications and not diagnostic criteria sets.5
On the other hand, it is very reassuring that the specificity of all sets were in accordance with the reported specificities, even in this cohort of early arthritis.2,–,4 ,6 ,8 This is especially of note for the ASAS-pSpA criteria as these are quite new, and there was a fear that they might not be specific enough.
In conclusion, the various criteria sets are very good in classifying patients, but are limited in assisting rheumatologists in diagnosing patients.
Acknowledgments
The authors would like to thank J. van Schonkeren for his technical assistance in HLA-B27 typing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Competing interests None.
Ethics approval This study was approved by the local medical ethical committee of the Leiden University Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.