Article Text

Abstract
Objectives Human leucocyte antigen shared epitope (SE) alleles are associated with joint destruction, the presence of anticitrullinated protein antibodies (ACPA) and the ACPA fine specificity repertoire in rheumatoid arthritis (RA). A large variation in joint destruction is seen within the ACPA-positive patient population, and it is conceivable that certain ACPA reactivities contribute to radiological damage. The authors investigated whether ACPA fine specificities, which are formed under the influence of SE alleles, associate with the extent of radiographic joint damage.
Methods Antibodies recognising six citrullinated epitopes were determined in sera of 330 ACPA-positive RA patients genotyped for SE alleles. The association between SE alleles, ACPA fine specificity and radiographic joint damage was assessed using radiographic follow-up data. A second cohort of 154 RA patients with 5 and 10-year radiographic follow-up was used for replication.
Results SE alleles predisposed to the recognition of certain citrullinated epitopes. However, none of the ACPA fine specificities studied influenced radiographic joint damage. Importantly, although SE alleles associated with radiographic damage in the total RA population, this association was no longer detectable after stratification for the presence of ACPA.
Conclusions SE alleles are instrumental in shaping the ACPA repertoire. However, ACPA fine specificities formed under the influence of SE alleles do not seem to affect joint destruction.
Statistics from Altmetric.com
Human leucocyte antigen (HLA) shared epitope (SE) encoding genes are the most prominent genetic risk factor for rheumatoid arthritis (RA). SE alleles exert their risk effect by predisposing to anticitrullinated protein antibody (ACPA)-positive RA.1 This and other findings have led to the concept that RA represents at least two distinct disease entities (ACPA-positive and negative RA), with different pathogenetic mechanisms.2 3
The strength of the SE effect on susceptibility to ACPA-positive disease depends on the number of SE alleles present, with two alleles conferring a higher risk of disease than one allele. The fact that ACPA are also found in SE-negative patients, albeit in lower frequency, indicates that SE alleles are not absolutely required for the development of ACPA.1 It has been postulated that SE alleles primarily facilitate the priming and activation of T-helper cells, which can then provide help to ACPA-producing B cells. Such help is required for isotype switching and the generation of a potent and long-lasting antibody response.
It is conceivable that certain citrullinated antigens are more potent than others in activating T cells in the context of SE alleles. Only very few T-cell epitopes have so far been found, and no skewing of T-cell responses has been described. However, SE alleles were found to associate with antibodies targeting peptides from citrullinated vimentin, but not with the presence of antibodies recognising citrullinated fibrinogen.4 This differential modulation of the ACPA response by SE alleles, and the fact that disease phenotypes vary greatly among ACPA-positive patients, has raised the question as to whether certain ACPA fine specificities might associate with a more severe disease phenotype. If so, designing assays that test for these specificities would be of prognostic value and could influence treatment decisions in the clinic.
In the present study, we analysed the relation between SE alleles, different ACPA fine specificities and their independent effects on disease outcome.
Methods
Patients and radiographs
ACPA fine specificity was determined on baseline serum samples of RA patients participating in the Leiden Early Arthritis Clinic (EAC).5 The present study included patients who presented between March 1993 and November 2006 and who fulfilled the 1987 revised American College of Rheumatology criteria for RA within the first year of follow-up. Annual radiographs of hands and feet were assessed as previously described.6
Replication of the association between SE alleles and radiographic progression in relation to ACPA status was performed using data of Norwegian RA patients with a maximum disease duration of 4 years included in 1992–3 in the European Research on Incapacitating Disease and Social Support (EURIDISS) project.7,–,9 Radiographs of the hands were available for 154 patients at baseline and were assessed according to the Sharp–van der Heijde method10 by one experienced reader with known time order.
Anti-CCP2 assays
Anticyclic citrullinated peptide 2 (anti-CCP2) antibody levels were measured by ELISA (EAC: Immunoscan RA Mark 2; Eurodiagnostica, Arnhem, The Netherlands; EURIDISS: INOVA Diagnostics, San Diego, California, USA).
ACPA fine specificity assays
Antibodies against the citrullinated and the arginine-containing form of two peptides derived from vimentin (Vim1-16; Vim59-74), two peptides derived from fibrinogen (Fibα 27-43; Fibβ 36-52), one peptide derived from α-enolase (Eno 5-20) and against citrullinated myelin basic protein (MBP) were determined by in-house ELISA as previously described.4 11
Cut-off values were defined as the mean plus three times the SD of the values of 30 control subjects (anti-CCP-negative EAC patients diagnosed with gout). Recognition was deemed to be citrulline-specific when the following requirements were met: (1) OD value citrullinated peptide greater than cut-off and (2) OD difference (OD citrullinated peptide – OD arginine-containing peptide) of 0.1 or greater. The number of patients recognising both the citrullinated and the arginine variant above cut-off levels was small (∼3%).
Statistical analysis
Association between fine specificity recognition and SE alleles was assessed using χ2 tests. Association of fine specificities with the rate of joint destruction was assessed using a repeated measurement analysis on log-transformed radiological data. Adjustments were made for age, gender and treatment strategy used at the time of inclusion as previously described.5 6 No association between the inclusion period and the recognition of separate ACPA fine specificities was found (data not shown). For the EURIDISS cohort, non-parametric Mann–Whitney U-test was used because of non-normal distribution of the data despite log-transformation. For comparison, the Mann–Whitney U-test was also applied to the Leiden EAC when indicated.
Results
HLA SE alleles associate with several ACPA fine specificities
SE alleles associate with the presence of certain ACPA fine specificities.4 We first extended these findings by analysing the reactivity to more citrullinated epitopes, by increasing the number of patients studied, and by analysing the effect of the SE gene dose on ACPA fine specificity. Three out of six citrullinated epitopes studied associated with the presence of SE alleles (table 1). Reactivity to citrullinated vimentin 59-74, citrullinated α-enolase 5-20 and citrullinated MBP was found in significantly increased frequency in SE-positive patients, whereas no such effect was observed for the other three antigens. The effect was independent of the number of SE alleles, as patients with one or two SE alleles displayed a comparable profile of ACPA epitope recognition. These data indicate that one SE allele is sufficient to facilitate the development of certain ACPA fine specificities, and that presence of a second SE allele does not further skew the ACPA profile towards more frequent recognition of a specific epitope.
Association of HLA SE alleles with ACPA fine specificity
The ACPA fine specificity repertoire does not predict future radiographic progression
ACPA-positive patients have more severe disease than ACPA-negative patients. However, it is unknown whether distinct ACPA fine specificities are pathogenetically driving the inflammatory process and thus lead to a more severe disease outcome. Considering radiographic joint damage as the most objective sign of disease severity in RA, we analysed the association between baseline recognition of specific citrullinated antigens and the progression of radiographic joint damage in ACPA-positive patients over the course of 5 years (figure 1A,B). The ACPA fine specificity repertoire in individual patients did not change during this time period.12 We did not detect a difference in radiographic outcome in patients who harbour ACPA of one of the fine specificities tested. Also, patients with ACPA that recognised more citrullinated peptides did not have a higher degree of progression of joint damage than patients with a limited ACPA repertoire (figure 1C). These data indicate that harbouring ACPA of any of the specificities tested has no direct influence on the progression of radiographic joint damage.
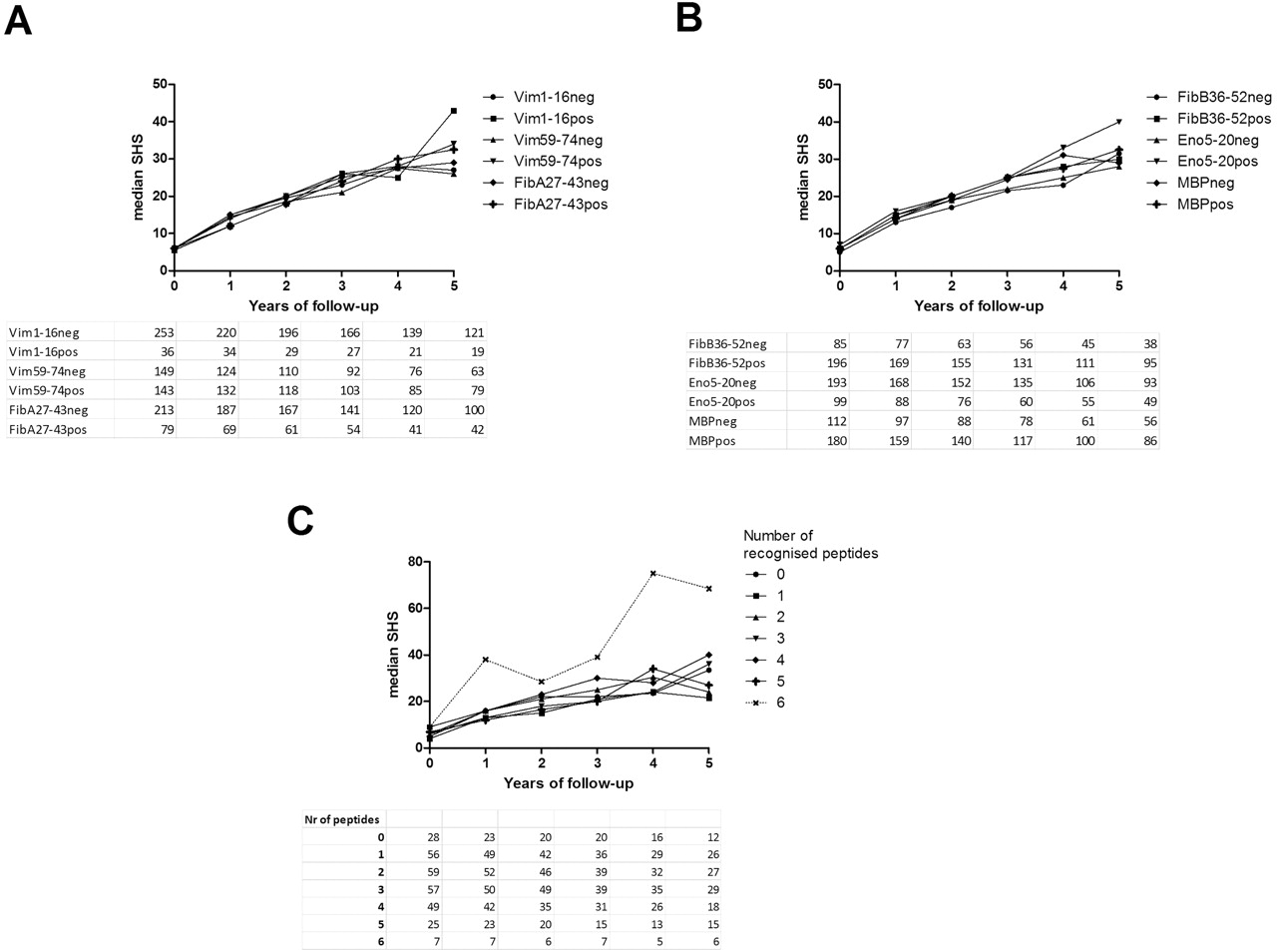
Association between different anticitrullinated protein antibodies (ACPA) fine specificities and radiographic progression. (A, B) Median Sharp–van der Heijde scores (SHS) during 5-year follow-up of ACPA-positive patients from the Leiden Early Arthritis Clinic testing positive or negative for six different ACPA fine specificities at baseline. (C) Median SHS in ACPA-positive patients grouped by the number of ACPA fine specificities recognised. All statistical comparisons (repeated measurement analysis) were non-significant (p>0.05). Numbers of patients in each group are given in the table below each figure. The line representing the group of patients recognising six fine specificities diverts from the rest due to the low number of patients in this group. In order to highlight this, this group is depicted with a dotted line. Radiographic data were available for 266 ACPA-positive patients at baseline and 132 at year 5. MBP, myelin basic protein.
Stratification for ACPA status abolishes the effect of HLA SE alleles on radiographic joint damage
None of the fine specificities tested was found to associate with radiographic progression. A drawback of this analysis is that lack of association does not exclude the possibility that the investigation of other citrullinated peptides would have revealed a positive association with long-term joint damage. As this limitation can persist in case more (non-associating) reactivities would be analysed, we reasoned that an additional way to investigate the relationship between the ACPA recognition profile and radiographic outcome is to study the effect of SE alleles on joint damage in ACPA-positive disease only. As SE alleles affect the recognition of certain citrullinated epitopes (table 1), SE alleles can be interpreted as a surrogate marker for the constitution of the ACPA response.
While SE alleles associated with the degree of radiographic joint damage in the total RA population (figure 2A), they no longer contributed to radiographic joint damage in ACPA-positive disease (figure 2B). We sought replication of this observation in the Norwegian EURIDISS cohort. The findings in that cohort with 5 and 10-year radiographic follow-up confirmed our results: there was no association between the presence of SE alleles and radiographic damage in ACPA-positive disease (figure 2C,D).

{kind=link}
{kind=link}
Shared epitope (SE) alleles exert no effect on radiographic progression after stratification for anticitrullinated protein antibodies (ACPA). Median Sharp–van der Heijde scores (SHS) in relation to SE positivity in the entire rheumatoid arthritis population and after stratification for ACPA-positive disease in patients of the Leiden Early Arthritis Clinic (EAC) (A/B) and of the European Research on Incapacitating Disease and Social Support (EURIDISS) cohort (C/D). For the Leiden EAC: radiographic data were available for 481 patients at baseline and 214 at year 5, of which 266 were ACPA positive (data for 132 available at year 5). (A) Repeated measurement analysis: p=0.013; Mann–Whitney U test p<0.001 at year 1, p<0.001 at year 2, p=0.007 at year 3, p=0.005 at year 4, p=0.012 at year 5; (B) repeated measurement analysis: p>0.05; all Mann–Whitney U p values greater than 0.05. For the EURIDISS cohort: radiographic data were available for 154 patients at baseline and 142 at year 10, of which 94 were ACPA positive (data for 83 available at year 10). (C) Mann–Whitney U test p=0.029 at baseline, p<0.001 at year 5, p<0.001 at year 10; (D) Mann–Whitney U test p=0.36 at baseline, p=0.93 at year 5, p=0.97 at year 10.
Discussion
Recent findings on ACPA fine specificity and its association with SE alleles have fuelled a hypothesis in which ACPA are pathogenetically driving the disease and in which certain ACPA fine specificities (developing preferentially under the influence of SE alleles) could be more pathogenic than others, leading to more severe joint destruction over time.4 13 Further insights into which ACPA fine specificities might be associated with disease severity could therefore have prognostic value and contribute to our understanding of disease pathogenesis.
In this study we could not detect an association between ACPA fine specificities and radiographic joint damage. An anticitrulline immune response to three out of six of the epitopes studied developed preferentially in patients harbouring SE alleles, but this did not translate into a more severe radiographic outcome. Also, the number of citrullinated epitopes recognised by an individual patient did not influence the degree of joint destruction. Although we accounted for baseline treatment strategy in this analysis, and although no association between the year of inclusion and recognition of the separate ACPA fine specificities was found, we cannot fully exclude the possibility that treatment effects later in the disease course could have influenced our results. The number of citrullinated epitopes also limits our study, and it cannot be excluded that other epitopes would have been more useful for this purpose. We addressed this issue by using SE alleles as a surrogate marker for those ACPA fine specificities that develop under the influence of SE alleles. After stratification for ACPA, SE alleles no longer contributed to joint damage. Based on this finding, we consider it unlikely that a SE-associated ACPA fine specificity can be identified that predicts disease course in RA. If such a predictive recognition profile exists, antibodies recognising this epitope are likely to be generated independent of SE alleles.
Our findings are relevant for strategies aimed at identifying patients who are at risk of rapidly progressive disease, and provide evidence that the recognition profile of the ACPA response is unlikely to have a relevant impact on radiographic progression.
References
Footnotes
-
Funding This study was supported by grants from the Kassenaarfonds, the Centre for Medical Systems Biology and the National Proteomics Center within the framework of The Netherlands Genomics Initiative (NGI); the European Union (Sixth Framework Program integrated project Autocure and Seventh Framework Program integrated project Masterswitch); NWO ZonMW AGIKO, VENI and VICI grants from The Netherlands Organization for Scientific Research and from The Netherlands Organization of Health Research.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Leiden University Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.