Article Text

Abstract
Objectives Systemic sclerosis (SSc) is characterised by vasculopathy, an aberrantly activated immune system and excessive extracellular matrix deposition. Inflammatory chemokines control migration of cells to sites of tissue damage; their removal from inflamed sites is essential for resolution of the inflammatory response. The atypical chemokine receptor D6 has a critical role in this physiological balance. To explore potential deregulation of this system in SSc, inflammatory chemokine and D6 expression were compared with that in healthy controls (HC).
Methods Serum levels of inflammatory mediators were assessed by luminex analysis. Peripheral blood mononuclear cells (PBMCs) were used in molecular and immunocytochemical analysis. Platelet-rich plasma was collected and assessed by western blotting for D6 expression levels. Sex-matched HC were used for comparison.
Results 72 patients with SSc and 30 HC were enrolled in the study. The chemokines MCP-1/CCL2, MIP-1α/CCL3, MIP-1β/CCL4 and IL-8/CXCL8 were significantly increased in patients with SSc, regardless of disease subtype and phase. Quantitative PCR analysis revealed a significant 10-fold upregulation of D6 transcripts in patients with SSc compared with controls, and this was paralleled by increased D6 protein expression in the PBMCs of patients with SSc. Platelet lysates also showed strong D6 expression in patients with SSc but not in controls. Importantly, high levels of D6 expression correlated with reduced levels of its ligands in serum.
Conclusions Inflammatory chemokines and the regulatory receptor D6 are significantly upregulated in SSc and high D6 levels are associated with lower systemic chemokine levels, indicating that some patients control systemic chemokine levels using D6. These results suggest that chemokines may represent a therapeutic target in SSc.
Statistics from Altmetric.com
Introduction
Systemic sclerosis (SSc) is a chronic autoimmune disease with a complex and poorly understood pathogenesis. The features of SSc include vasculopathy, aberrant immune system activation and multiorgan fibrotic changes resulting from excessive extracellular matrix deposition.1 Currently, the link between these features in the pathogenic process is not entirely understood and it is unclear how the early inflammatory phases result in the later fibrotic stage that causes multiple end-organ damage and death.2 However, the clear involvement of inflammatory processes in the pathology suggests that understanding the molecular orchestration of inflammatory leucocyte accumulation in SSc will provide novel avenues for therapeutic intervention. Importantly, chemokines and their receptors have been implicated through human, animal and in vitro studies as being involved in the pathogenesis of SSc. In particular, chemokines such as CCL2, CCL5, CCL7 and CXCL8 have been implicated in the initiating phase and in the perpetuation of the inappropriate fibroblast activation and concomitant extracellular matrix deposition that characterise this disease.3,–,5 This therefore highlights the chemokine/chemokine receptor system as a potential therapeutic target in SSc.
Chemokines are small proteins and membership of this family is defined on the basis of the presence of variations of a conserved cysteine motif in the mature proteins.6 7 This system is crucial in a number of biological functions, although its major role is in regulating tissue-specific leucocyte migration under both inflammatory and homeostatic conditions.6,–,8 Inflammatory chemokines can be induced following tissue damage or infection, or upon exposure of cells to proinflammatory cytokines. In inflamed contexts, interaction of inflammatory chemokines with their cognate receptors on leucocytes results in inflammatory cell influx and accumulation at damaged or infected sites. Chemokines are therefore central to the initiation and maintenance of inflammatory responses and, subsequently, the fine tuning of their expression at inflamed sites contributes to the resolution of this response, promoting wound healing and repair of tissues. Importantly, the inflammatory response is compromised in SSc,1 but whether this results from problems at the initiation, maintenance or resolution phases is not currently known.
We have a particular interest in the molecular regulation of the resolution of chemokine-dependent inflammatory responses with emphasis on the roles for the D6 chemokine scavenging receptor in this process.9 10 D6 is a highly promiscuous (binding all inflammatory CC chemokines) and apparently non-signalling receptor for chemokines.11,–,13 In human tissues, sites of D6 expression include skin, lung and gut, with lymphatic endothelial cells being the predominant D6-expressing cells in these organs.14 In addition, D6 is strongly expressed in the placenta where it has been localised to the syncytiotrophoblast layer.15 16 More recently we have also demonstrated D6 expression by haemopoietic cells with the strongest expression being detected on B lymphocytes and dendritic cells.17 D6 immunoreactivity has also been detected in human inflamed tissues such as the atopic dermatitis skin or rheumatoid arthritis synovium.17 In vitro analyses point strongly to a role for D6 as a scavenger for inflammatory CC chemokines and demonstrate the ability of D6 to bind inflammatory chemokines, internalise them and target them for intracellular degradation.18 19 Subsequent in vivo studies have also borne this out, demonstrating exaggerated cutaneous,20,–,22 gut23 24 and lung25 inflammatory responses as well as a predisposition to inflammation-associated spontaneous abortion in D6 null mice.15 16 Together, these findings suggest that D6 plays a regulatory role in the resolution of the in vivo inflammatory response and highlights it as a possible point of dysfunction in a variety of inflammatory human pathologies.
The aim of the present study was to determine inflammatory cytokine and chemokine levels in patients with SSc presenting with various subsets and phases of disease. In addition, we analysed D6 expression in isolated peripheral blood mononuclear cells (PBMC) and platelet-derived lysates from patients with SSc.
Methods
Patients
Patients attending the Rheumatology Unit of the IRCCS Foundation San Matteo in Pavia, Italy who satisfied the LeRoy criteria for SSc26 or early SSc27 were enrolled after providing informed consent between July 2006 and August 2010. Sex-matched healthy subjects were included as controls (HC). Patients with diffuse cutaneous (dc)-SSc of <2 years duration from the first non-Raynaud symptom were considered to be in an ‘early’ phase. Organ involvement was evaluated according to the presence of signs and symptoms of disease at the visit and imaging data as follows. If either the chest x-ray, high-resolution CT scan of the thorax, pulmonary function tests measuring carbon monoxide transfer factor or echocardiography—followed eventually (if PAP >40 mm Hg) by right heart catheterisation—gave an indication of interstitial or vasculopathic lung disease, pulmonary involvement was recorded. For gastroenteric involvement, an x-ray of the oesophagus and endoscopic evaluation of the upper gastrointestinal tract were performed. Patients were also scored according to activity28 and severity29 scores. Laboratory tests included antinuclear antibodies (ANA) by indirect immunofluorescence on HEp-2 cells (Diamedix Co., Miami, Florida, USA) with pattern description to detect anticentromere antibodies (ACA). Other autoantibody specificities, including anti-topo I and anti-RNA polymerase III, were evaluated using commercially available kits (EliA or ELISA; Phadia, Uppsala, Sweden or MBL, Toronto, Canada).
Multiplex cytokine assay
Blood samples were collected into collection tubes, allowed to clot, centrifuged at 4000 rpm for 10 min and the serum was immediately stored at −20°C until use. Serum samples were used immediately after defrosting and were not subjected to further freeze-thaw cycles. Levels of inflammatory cytokines and chemokines (interleukin (IL)-1β, IL-1ra, IL-2, IL-2R, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-12 (p40), IL-13, IL-15, IL-17, tumour necrosis factor (TNF)-α, interferon (IFN)-α, IFN-γ, granulocyte-macrophage colony stimulating factor (GM-CSF), macrophage inflammatory protein (MIP)-1α, MIP-1β, IP-10, MIG, eotaxin, RANTES, monocyte chemoattractant protein (MCP)-1) were detected using a multiplex bioassay (Invitrogen, Paisley, UK). Protein concentrations were calculated by the Bioplex machine software using a standard curve derived from recombinant molecules according to the manufacturer's instructions. For RANTES, the results were confirmed by ELISA (Invitrogen). Only molecules that were significantly different between patients and HC were considered in further analyses and in clinical correlates.
PBMC isolation, cytospins and mRNA extraction
PBMCs were extracted from freshly drawn peripheral blood by Ficoll (Sigma-Aldrich, Dorset, UK) gradient and washed in phosphate buffered saline (PBS). The suspension was then divided in two aliquots: one cytocentrifuged with slides subsequently frozen at −80°C and the other used for mRNA extraction (RNeasy miniKit; Qiagen, Crawley, UK).
RT-PCR
After on-column purification and genomic DNA removal, first-strand cDNA was synthesised with oligod(T) (Stratagene, California, USA) according to the manufacturer's instructions. Quantitative PCR was then performed on a 7900HT real-time PCR system (Applied Biosystems, Warrington, UK) using SYBR-green containing mix and specific primers as previously described.17 Detected levels of D6 transcripts were normalised to TATA binding protein.
Immunocytochemistry
Frozen slides were defrosted, fixed in acetone for 10 min and air-dried. Non-specific binding sites were blocked by incubation with 2.5% horse serum TBS-Tween 20. Subsequently, a monoclonal anti-D6 antibody or appropriate isotype control (both from R&D Systems) were incubated overnight at 4°C. Next day, a biotinylated secondary antibody was incubated for 30 min, followed by ABC reagent (Vector Laboratories, Peterborough, UK), and the reaction was then developed with Impact Diaminobenzidine (Vector Laboratories). The slides were examined and the number of D6 positive cells scored over a total of 100 cells in random high power fields (hpf) with a BX40 Olympus microscope using 40× magnification. The results shown are the mean of three independent observations for each subject.
Platelet-rich plasma extraction
Platelet-rich plasma (PRP) extracts were obtained from peripheral blood; 1 ml of blood was mixed with Tyrode's buffer and centrifuged twice to separate the red blood cell fraction. Prostacyclin (1 μg/ml) was added to the clear platelet-enriched fraction and the suspension was centrifuged again and resuspended in MPER buffer and protease inhibitors (Thermo Scientific, Loughborough, UK). The protein extracts were frozen at −20°C until use.
Western blot analysis
One μg of sample was ultracentrifuged and electrophoresed on 4–2% acrylamide gels according to the manufacturer's instructions (Invitrogen). After electrophoresis, proteins were transferred to a nitrocellulose membrane and blocked in PBS-Tween 20 with 5% milk. Membranes were incubated overnight with a monoclonal anti-D6 antibody.14 A secondary antimouse antibody conjugated with horseradish peroxidase (Amersham Bioscience, Buckinghamshire, UK) was used to detect the binding and the reaction was developed with a chemiluminescence assay (Biorad, Hemel Hempstead, UK) and chemiluminescence detected following exposure to x-ray films. HEK and D6-transfected HEK (HEK-D6) served as negative and positive controls, as described previously.30
Statistical analysis
Continuous variables are expressed as mean±SD or median (range) according to their distribution. Qualitative variables are expressed as absolute numbers and percentages. Accordingly, parametric or non-parametric tests were run to investigate differences between groups, and exact tests when needed. A two-tailed p value <0.05 was considered significant. In the case of multiple comparisons, a Bonferroni or Kruskal–Wallis correction was applied to the test. Statistical analyses were performed using GraphPad4 for Macintosh (GraphPad Software).
Results
Main clinical features of the study patients
A total of 72 patients were enrolled in the study. Their main clinical features are shown in table 1. Age, sex distribution and percentages of ANA positivity were comparable between groups. As expected, clinical baseline differences between subsets were apparent in autoantibody distribution with a higher percentage of ACA in those with limited cutaneous (lc)-SSc, a higher percentage of antitopoisomerase I in those with dc-SSc and a higher median modified Rodnan Skin Score in the dc-SSc group.
Patient characteristics and clinical features
Separate analysis of early and established subgroups showed that there was a higher frequency of pulmonary involvement in both subsets of patients with established SSc (62% in lc-SSc and 81% in dc-SSc) compared with the respective subgroups in those with early SSc (p<0.01 for both). In lc-SSc, gastroenteric involvement was also present in a significantly higher percentage of patients with established disease than in the respective early disease controls (37% vs 11%, p<0.05). Overall, there was a significantly higher median disease activity index in patients with dc-SSc than in those with lc-SSc (1 (range 0–6) vs 0.5 (range 0–5), p<0.05), but the difference was not consistent across different phase categories of the disease.
Detection of inflammatory mediators in serum
Cytokines are well-characterised initiators and maintainers of immune and inflammatory responses and pathologies. In addition, chemokines are essential regulators of leucocyte migration during immune and inflammatory disorders and are likely to be fundamental contributors to the pathogenesis of SSc. Therefore, to provide novel insights into these mechanisms, we used multiplexing technology to measure the levels of inflammatory cytokines and chemokines in the serum from 62 patients (40 lc-SSc, 22 dc-SSc) and 30 HC. Using this approach, a number of differences in cytokine levels between patients and HC were detected. Note that only those cytokines and chemokines showing significant differences between SSc and HC are discussed. Specifically, IL-6, IL-1RA and IL-13 were significantly increased in SSc compared with HC (p<0.001 for both IL-6 and IL-1RA, p<0.05 for IL-13). No differences in the levels of any of these cytokines were noted between SSc subtypes (figure 1 and insets). The classic inflammatory chemokines CCL2, CCL3, CCL4 and CXCL8 all showed higher levels in patient versus control samples, again regardless of disease subtype and phase (p<0.001 for all, figure 2 and insets). The most striking difference was seen with CXCL8, which was markedly high in all phases and subtypes of SSc compared with HC. To examine associations, the serological values of these cytokines and chemokines and the main clinical parameters were correlated with each other. Indices such as modified Rodnan Skin Score and disease activity only significantly correlated to each other (Spearman's r=0.35, p<0.05). No clear associations were seen between these parameters and levels of any of the cytokines or chemokines measured, while direct significant correlations were noted between IL-6 and IL-1RA and between both of these cytokines and levels of CCL3 and CCL4, and between IL-1RA and CCL2. Examination of chemokine levels indicated that CCL2 correlated with each of the other major chemokines and that there was also a very significant correlation between the levels of CCL3 and CCL4. CXCL8 levels correlated with all of the CC chemokines considered (see table 2 for descriptive statistics presented as adjusted r values).

Levels of the inflammatory-related cytokines (A) interleukin (IL)-6, (B) IL-1RA and (C) IL-13 in healthy controls (HC) and patients with systemic sclerosis (SSc). *p<0.05, **p<0.01, ***p<0.001. Insets show details of the levels of IL-6, IL-1RA and IL-13 in different subsets (diffuse cutaneous (dc) SSc or limited cutaneous (lc) SSc) and phases of the disease (early vs established SSc).

Levels of the inflammatory chemokines (A) MCP-1 (CCL2), (B) MIP-1α (CCL3), (C) MIP-1β (CCL4) and (D) IL-8 (CXCL8) in the peripheral blood of healthy controls (HC) and patients with systemic sclerosis (SSc). ***p<0.001. Insets show details of the levels of MCP-1 (CCL2), MIP-1α (CCL3), MIP-1β (/CCL4) and IL-8 (CXCL8) in different subsets (diffuse cutaneous (dc) SSc or limited cutaneous (lc) SSc) and phases of the disease (early vs established SSc). IL, interleukin; MCP, monocyte chemoattractant protein; MIP, macrophage inflammatory protein.
Adjusted correlation values (r) between inflammatory markers elevated in systemic sclerosis
Analysis of D6 transcripts
The inflammatory CC chemokines (CCL2, CCL3 and CCL4) are all ligands for the D6 chemokine scavenging receptor9 which is known to be expressed on PBMCs.10 17 The upregulation of D6 ligands in the serum of patients with SSc therefore prompted us to examine whether D6 expression might be increased in response to this in PBMCs of patients with SSc. From a subset of 29 patients (8 dc-SSc, 21 lc-SSc) we isolated PBMCs and analysed both RNA and protein expression of D6 and compared it to that seen in 26 HC. Cytokine and chemokine levels in the serum samples of this subset of patients were similar to those reported for the main cohort (figures 1 and 2), except for IL-13 for which the difference between patients and controls did not reach statistical significance (not shown).
Real-time quantitative PCR analysis revealed a significant (approximately 10-fold) upregulation of D6 transcripts in patients with SSc compared with controls (p<0.001, figure 3) and, as with the inflammatory mediators, this was regardless of disease subtype and phase (not shown). To examine any correlations between D6 expression levels and inflammatory markers in serum we subcategorised the patients as being ‘D6 high’ or ‘D6 low’ in PBMC relative to the median D6 expression value (4.75). We then examined correlations between D6 expression levels and serum levels of the cytokines and chemokines that showed significantly higher levels in patients with SSc than in HC (figures 1 and 2). ‘D6 high’ and ‘D6 low’ patients showed significantly higher levels of IL-6 and IL1-RA than controls and, importantly, the significant increase in CXCL8 was still observed in both these subgroups. In contrast, however, ‘D6 high’ patients showed no differences in serum levels of the D6 ligands CCL2 and CCL4 compared with controls. Notably, these differences were seen to be maintained in ‘D6 low’ patients. A similar effect was seen for CCL3, although the serum levels in ‘D6 high’ patients remained significantly higher than in HC (figure 4).

Quantitative PCR analysis of D6 expression in leucocytes from patients with systemic sclerosis (SSc). Quantitation of D6 transcript levels normalised to TATA-binding protein (TBP) expression in healthy controls (HC) and patients with SSc. ***p<0.001.

Differences in inflammatory CC chemokine levels in patients with high and low levels of D6. Levels of (A) IL-6, (B) IL-1RA, (C) IL-8 (CXCL8), (D) MCP-1 (CCL2), (E) MIP-1α (CCL3) and (F) MIP-1β (CCL4) in healthy controls (HC), ‘D6 high’ or ‘D6 low’ patients with systemic sclerosis (SSc) relative to the median D6 expression value (4.75). *p<0.05, **p<0.01, ***p<0.001. IL, interleukin; MCP, monocyte chemoattractant protein; MIP, macrophage inflammatory protein.
D6 protein expression in PBMCs and PRP extracts
The increase in transcript levels was also paralleled by increased D6 protein expression as revealed by immunocytochemistry on cytospins of PBMCs from patients and HC. D6 was present mainly in mononuclear cells and, in keeping with the known subcellular distribution of D6,19 30 showed a predominantly cytoplasmic localisation. This cytoplasmic localisation—whereby more than 95% of D6 is in intracellular endosomes—is essential for the recycling and scavenging activity of D6.19 D6-positive cells were quantified on the stained cytospins, giving a mean of 16±5/100 positive cells per high power field (hpf) in patients with SSc versus 7±3/100 cells in HC (p<0.001, figure 5). There was a significant correlation between D6 transcript levels and numbers of D6-positive cells in individual patients (r=0.52, p<0.05) and, despite not reaching statistical significance, patients with dc-SSc had a slightly higher mean number of cells than those with lc-SSc (not shown).
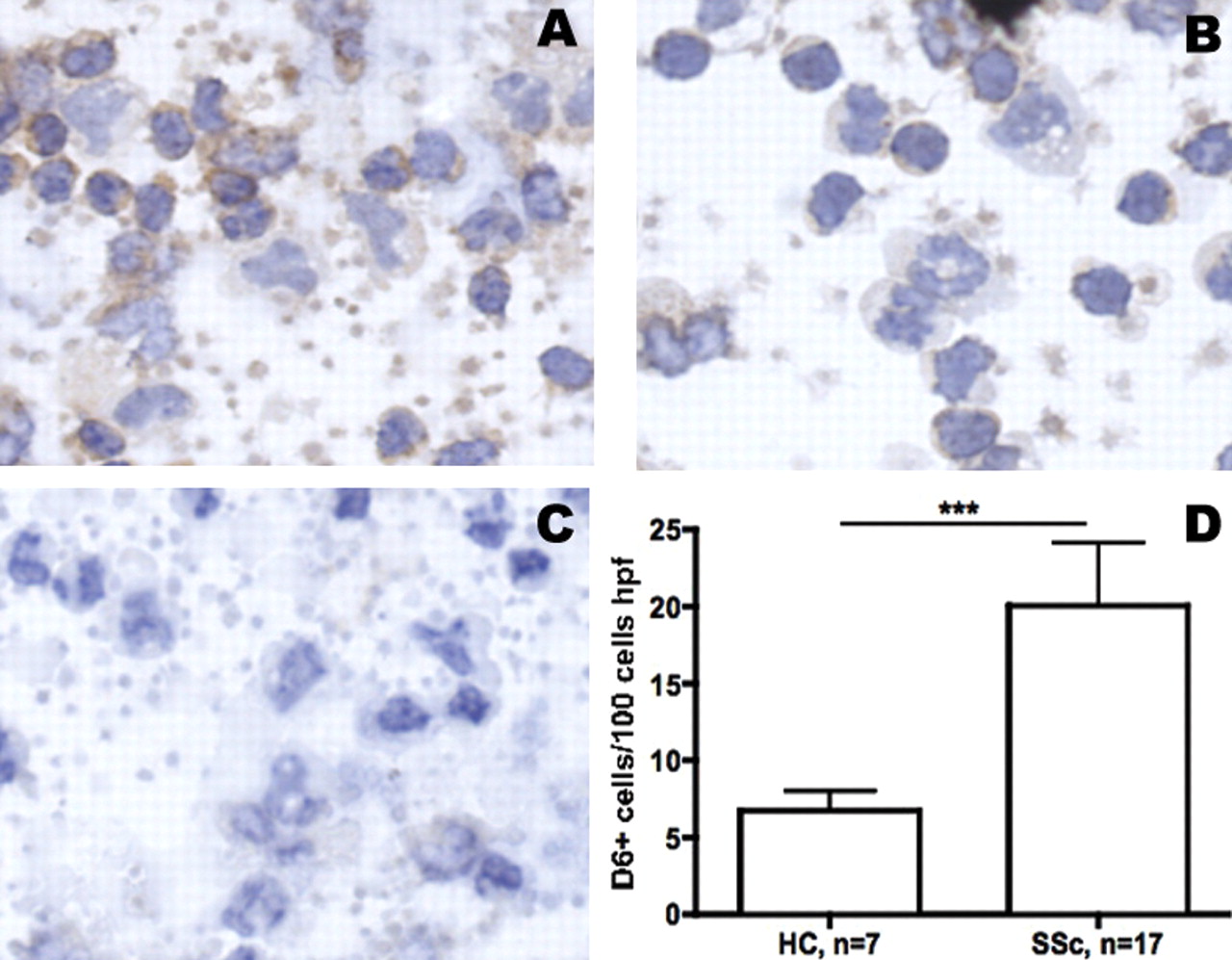
Immunochemical analysis of D6 expression in peripheral blood leucocytes from patients with systemic sclerosis (SSc) and healthy controls (HC). (A) Representative D6 staining in a patient with SSc. (B) D6 staining in an HC. (C) Isotype control from the same patient with SSc as in (A). (D) Mean and SEM values of positive D6 cells per high power field (hpf) in patients with SSc (n=17) and HC (n=7). ***p<0.0001.
Megakaryocytes and platelets have been shown to express D6.10 17 Recent attention has been paid to the role of platetets in patients with SSc as carriers of inflammatory cytokines and chemokines and therefore as potential mediators of fibrosis.31 We measured the levels of D6 in extracted PRP from patients with SSc (4 lc-SSc, 1 dc-SSc) and two HC to obtain a further index of D6 expression in SSc. Lysates of D6-transfected HEK cells were used as a positive control.30 Western blot analysis of PRP lysates revealed a strong band corresponding to D6 in four of the five patients with SSc compared with a weak band detected in controls (figure 6). Note that this band corresponds to the molecular weight of the upper band in the doublet in the HEK-D6 control lane. We have previously demonstrated this to be glycosylated D6, which suggests that the majority of D6 present in PRP is glycosylated.30

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Western blot analysis of D6 expression in healthy controls and patients with systemic sclerosis (SSc). D6 protein was detected using an anti-D6 antibody. The gel was loaded with 1 μg of protein extracts from transfected Hek-D6 (positive control, lane 1), platelet rich plasma extracts of healthy controls (lanes 3 and 4) and patients with SSc (lanes 5–9) and non-transfected Hek cells (lane 11). Lanes 2 ands 10 are blank on this gel.
Discussion
SSc is a complex connective tissue disease with pleiotropic features which results from a mutlifactorial poorly understood pathogenesis.1 2 Inflammatory chemokines and their receptors are key contributors to the pathogenesis of a range of inflammatory pathologies,32 and the chemokine system has been reported in SSc to be engaged in the perpetuation of the chronic damage and in the induction of fibrosis.33 In this context, specific attention has been paid to CCL2 which has previously been reported to be overexpressed in the skin and serum of patients with SSc and associated with a higher frequency of pulmonary involvement.34,–,37 High CCL2 levels have been described in early phases of the disease and in patients with higher frequencies of cardiac and vasculopathic or interstitial pulmonary involvement.38 There are also a number of reports linking CCL2 polymorphisms with SSc,39 although other studies do not support this association and this remains a controversial issue.40 Other inflammatory chemokines have been associated with SSc, and compound polymorphisms in CCL5 and CXCL8 appear to increase the risk of SSc.41 Thus SSc, like all other inflammatory and immune disorders, results from a significantly chemokine-dependent pathogenesis. Our present data confirm that inflammatory chemokines are high in the serum of patients, and the inflammatory status of these subjects is further indicated by the higher levels of IL-6 and of IL-1RA in SSc compared with controls. Importantly, increased cytokine and chemokine levels represent a feature of both main SSc subsets and are also seen at different phases of SSc: early (without any major clinical involvement) and later (when the damage caused by the disease is established and detectable at a clinical level).
Interestingly, the levels of inflammatory cytokines and chemokines are increased in SSc independently of the disease phenotypes and clinimetric measures suggesting that, while clearly associated with the pathogenesis of SSc, other factors may be critical for determining the level of disease activity and severity. There are, however, clear associations between the levels of cytokines and chemokines detected, suggesting that expression of a number of these inflammatory agents is coordinated in SSc. It was questioned whether chemokine measurements could be used in risk stratification for SSc patients with controversial results.38 42 Our data suggest that the inflammatory markers measured in this study are likely to be pathogenically important but represent poor biomarkers of SSc, whose detection might be of limited relevance in daily clinical practice.
The reason for a clear lack of correlation with disease features is not immediately apparent. It may be that circulating chemokines are essentially irrelevant to the pathogenesis and simply represent an epiphenomenon relating to leakage of chemokines directly from inflamed and damaged tissue sites. In addition, it is possible that the lack of correlation relates to blood-mediated homeostatic regulation of levels of the circulating inflammatory chemokines. In this respect, the CC chemokine-scavenging receptor D6 has a very important physiological role in the fine tuning of inflammatory chemokine signals, promoting their clearance from local sites of expression.9 Our report shows, for the first time, that the expression of D6 is markedly higher in PBMC and PRP of patients with SSc at both the transcript and protein levels, findings that are in line with other studies showing leucocyte and megakaryocyte expression of D6.17 These data represent the first report of increased D6 expression in leucocytes in an inflammatory pathology. Furthermore, we observed a correlation between the presence of high numbers of D6 transcripts and a lack of increase in serum levels of some of its ligands such as CCL2, CCL4 and (weakly) CCL3 in patients with SSc compared with HC. Notably, similar effects were not seen with the other cytokines examined or with CXCL8, a chemokine not targeted by D6. This therefore confirms the specificity of the effect observed. These results provide the first evidence of a homeostatic role for D6 in regulating systemic inflammatory CC chemokine levels in patients with an inflammatory disorder. Our ongoing studies indicate that elevated D6 is a hallmark of many other inflammatory pathologies, which suggests that it may play similar roles in a range of other diseases such as rheumatoid arthritis or psoriasis (data not shown). As already mentioned, D6 is not a scavenger for CXCL8 so it may be that other regulators of chemokine levels and function are also present in the blood. For CXCL8, this may include buffering of levels by DARC,12 43 44 a broadly promiscuous decoy receptor for inflammatory chemokines.
To our knowledge, only one previous study has investigated the expression of D6 in SSc.3 The target cells of this study were in vitro cultured dermal fibroblasts from affected skin and they were shown not to express transcripts for D6. However, it is probable that leucocytes represent a more functionally relevant cellular population for D6 and inflammatory chemokine regulation,17 and our study represents the first examination of D6 expression in this biologically critical cell population in SSc. It is worth noting that we could not detect any distinct clinical association with the presence of D6 in patients' blood although, while not significant, levels were higher in those with dc-SSc, which could reflect the higher disease activity seen in this subset of patients. Further studies are needed to determine how the systemic upregulation of inflammatory chemokines and D6 in blood seen in this study relates to peripheral sites of disease involvement such as the skin and lung that show clear evidence of an active and deregulated immune response in SSc.34 45
In conclusion, we describe here for the first time the high level of expression of the inflammatory chemokine-scavenging receptor D6 in PBMCs and PRP in the blood of patients with SSc. This is paralleled by the presence of high serum levels of some of its ligands in both lc-SSc and dc-SSc subsets, and in early and more advanced phases of the clinical course of the disease. In addition, D6 appears to be able to homeostatically regulate the systemic levels of its ligands in SSc. Our study highlights inflammatory chemokines and D6 as important promising targets for further investigation and potential therapeutic intervention. This is critical, especially in a disease like SSc where the therapeutic options are too limited to block the progression to end-organ damage that affects quality of life and increases mortality.
References
Footnotes
-
Funding This study was supported by grants from the MRC, CSO and ARC (to GJG). VC was supported by a Clinical Training Fellowship from Novo Nordisk.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Foundation Policlinico San Matteo.
-
Provenance and peer review Not commissioned; externally peer reviewed.