Article Text

Abstract
Objective To assess cause-specific incidence and its trend of musculoskeletal (MSK) disorders at global, regional and national levels.
Methods Data on MSK disorders were downloaded from the Global Burden of Disease 2017 study website. Estimated annual percentage change (EAPC) was calculated to quantify the temporal trend in age-standardised incidence rate (ASR) of MSK disorders, by age, sex, region and cause.
Results Between 1990 and 2017 incident cases of MSK disorders increased globally by 58% from 211.80 million to 334.74 million, with a decreasing ASR of 0.18% annually (95% CI −0.21% to −0.15%). The ASR decreased for low back pain (LBP), remained stable for neck pain (NP), and increased for rheumatoid arthritis (RA), osteoarthritis (OA) and gout, with EAPCs (95% CI) of −0.24 (−0.29 to –0.20), −0.09 (−0.13 to −0.05), 0.36 (0.28 to 0.43), 0.32 (0.28 to 0.36) and 0.22 (0.21 to 0.23), respectively. It appears women have higher increase in EAPC than men for RA (1.3 times) and gout (1.6 times). The absolute EAPC was strikingly high in high or high-middle sociodemographic index (SDI) regions for overall, LBP and gout, and in low SDI regions for NP. EAPC was significantly associated with baseline ASR for LBP (nonlinear), RA (ρ=−0.41) and gout (ρ=−0.42), also with 2017 human development index for LBP (ρ=−0.53) and gout (ρ=0.15).
Conclusions Globally, MSK disorders remain a public health burden. The ASR is decreasing for MSK disorders overall, mainly in high-middle SDI regions, but increasing for RA, OA and gout.
- epidemiology
- gout
- low back pain
- osteoarthritis
- rheumatoid arthritis
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The burden of musculoskeletal (MSK) disorders have been growing worldwide, but its incidence pattern and temporal trend overall and by specific causes are hardly reported.
What does this study add?
Globally, the age-standardised incidence rate (ASR) of MSK disorders decreased by an annual average of 0.18%, while the number of incident cases has increased by 58% from 1990 to 2017.
By cause, the global ASR showed a decreasing trend for low back pain (LBP), remained stable for neck pain (NP), and increased for rheumatoid arthritis (RA), osteoarthritis and gout.
Women had higher increase in estimated annual percentage change (EAPC) than men for RA and gout.
The absolute EAPC was strikingly high in high or high-middle sociodemographic index (SDI) regions for MSK disorders, LBP and gout, and in low SDI regions for NP.
EAPC from 1990 to 2017 was significantly associated with baseline ASR for LBP, RA and gout, also with human development index in 2017 for LBP and gout.
How might this impact on clinical practice or future developments?
The results help to illustrate the trend of the global disease burden of specific MSK disorders, which can serve as a baseline for relevant policies, programme design and follow-up studies for reducing the burden of MSK disorders.
Introduction
The burden of musculoskeletal (MSK) disorders is extremely high globally.1 MSK disorders rank the fifth cause of disability-adjusted life years (DALYs) and the highest in terms of years lived with disability (YLDs), accounting for 5.6% of the total DALYs and 15.9% of the total YLDs, respectively in 2017.1 2 Along with the rise in life expectancy and population growth, a bigger increase in the burden of MSK disorders is expected.3 Importantly, in addition to pain, functional disability and work incapacity, MSK disorders often led to psychological problems, increased risk of all-cause mortality and developing chronic diseases.4 5 However, compared with other causes such as cardiovascular diseases and cancers, the MSK disorders were placed as lower importance because of low case fatality and its irreversibility.6 7
Since the Global Burden of Disease (GBD) study in 2010, all MSK disorders have been estimated and classified into six categories, including rheumatoid arthritis (RA), osteoarthritis (OA), low back pain (LBP), neck pain (NP), gout and a group of other MSK disorders.8–14 The burden of MSK disorders was measured on incidence, prevalence, mortality and non-fatal health loss such as DALYs, YLDs and years of life lost (YLLs) in GBD study. DALY is the standard metric for quantifying the burden and varies by the specific causes. According to estimates from GBD study 2017, the largest contribution to global DALYs caused by MSK disorders was LBP (46.8% in 2017), followed by NP (20.6%), OA (6.9%), RA (2.5%) and gout (0.9%). Other MSK disorders, accounting for 22.2% of DALYs in 2017 globally, are not included in this analysis due to unavailability of any specific incidence data from GBD study.
Since 2010, the GBD study has not provided data on MSK disorders and specific causes, except a GBD study 2013 where the prevalence, mortality and health loss measurements of MSK disorders were presented for the Eastern Mediterranean region.15 A recent study, using data from the WHO Global Health Estimates Database, reported DALYs, YLDs and YLLs but not incidence of MSK disorders globally from 2000 to 2015.6 Moreover, no study ever quantified the annual trend in incidence of MSK disorders and specific causes over a specified time period. This study, for the first time, analysed the incidence of MSK disorders caused by five major causes as well as temporal trend at global, regional and national levels, using data from the GBD study 2017. Their association with countries’ human development index (HDI) and baseline age-standardised incidence rate (ASR) was also analysed.
Materials and methods
Overview
The GBD study provides comprehensive epidemiological estimates on incidence, mortality, prevalence and YLDs of diseases and injuries across each specific group of country and territory, sex, age and year. The detailed methods for gathering, processing and producing those data have been described extensively in the GBD 2017 studies.1 2 16 17 In summary, the GBD study combines all available sources of information, such as published literature, surveillance data, survey data, hospital and clinical data. The risk of bias of each data source was assessed and corrected for standardised statistical estimation and model performance assessment by cross-validation analysis, using the Bayesian meta-regression tool DisMod-MR V.2.1. In addition, the GBD study conducts annual updates to incorporate new data sources and develops new methods to adjust representativeness bias for each data element. With regard to specific MSK disorders, details on flow chart, definitions, input data and modelling strategy are available in the online supplementary appendix 1 of the GBD study 2017 (https://www.thelancet.com/cms/10.1016/S0140-6736(18)32279-7/attachment/6db5ab28-cdf3-4009-b10f-b87f9bbdf8a9/mmc1.pdf).
Supplemental material
Data collection
We downloaded data from the Global Health Data Exchange query tool (http://ghdx.healthdata.org/gbd-2017), including incident numbers, incidence rate and ASR of MSK disorders from 1990 to 2017, by sex, age, location and cause.18 Data were available from a total of 195 countries and territories, and those were categorised into five regions on the basis of sociodemographic index (SDI) and 21 GBD regions according to geographical contiguity. The full list of countries and territories, and regions is shown in online supplementary table S6 and table 1. Cause specifically, we obtained incidence information from five major MSK disorders, namely RA, OA, LBP, NP and gout. HDI data in 1990 and 2017 are available for 189 countries and territories in the Human Development Report 2019 (http://hdr.undp.org/en/composite/trends). The available HDI data can be matched with incident cases among 184 countries and territories, except American Samoa, Bermuda, Greenland, Guam, North Korea, Northern Mariana Islands, Puerto Rico, Somalia Syria, Taiwan and Virgin Islands.
The incident cases and ASR of MSK disorders in 1990 and 2017
Statistical analysis
The ASR and estimated annual percentage change (EAPC) were used to estimate the trend of MSK disorders.19 To compare the incidence rates of MSK disorders across different populations, direct standardisation of incidence was used to adjust for potential confounding of age structure. Let Tk be the distribution of the chosen reference standard population in the k age groups, and Ik be the age-specific incidence rate, then a weighted average of incidence rate was computed with weights from the age distribution.

To summarise and quantitatively evaluate the trend of ASR over a specified period, EAPC and its 95% CIs were calculated by fitting a regression line to the natural logarithm of the ASR.19 20 Briefly:


where y=ln (ASR), and x=calendar year.
An EAPC estimation above 0 means an increasing ASR, while being below 0 indicates a decreasing ASR. If 95% CIs of the EAPC include 0, there is no change in ASR over time. A hierarchy cluster analysis was performed to classify 195 countries and territories by the EAPC and its 95% CI. The correlation analysis was then conducted between EAPC and ASR in 1990, between EAPC and HDI in 2017 and between ASR and HDI for overall and by cause. The global incidence of overall, RA, OA, LBP, NP and gout by country for both sexes combined were depicted with maps, including the ASR in 2017, the percentage change in incident cases and the EAPC in ASR in 1990–2017. Pearson correlation analysis was used to estimate the ρ indices and p values for the association of EAPC with HDI and baseline ASR. The break point was estimated by the change of ρ indices in the smoothed curve. Data were analysed using R programme (V.3.5.3, R core team). A p value of <0.05 was considered statistically significant
Results
Incident cases of MSK disorders
Globally, in 2017, the incident cases of MSK disorders increased by 58% from 211.80 million in 1990 to 334.74 million in 2017. The most prominent incident cases were in China, India and USA, and the corresponding change percentages were 42.78%, 77.98% and 42.61%, with country-specific details in online supplementary table S6 and figure 1B. It increased particularly in the 35–64 year age group, with the peak shifted from age 35–39 years in 1990 to age 45–49 years in 2017. Females (180.77 million in 2017) had relatively higher incident cases than males (153.97 million in 2017, figure 2; table 1). Incident cases increased across all regions in 1990–2017, with the greater increase observed in the lower SDI regions (table 1; figure 3A). In GBD regions, the greatest increase in incident cases was in Western Sub-Saharan Africa (SSA, 138.19%), followed by Central SSA and Eastern SSA (table 1; figure 3B).

The global incidence of MSK disorders by countries and territories for both sexes combined. (A) The ASR of MSK disorders in 2017. (B) The percentage change in incident cases of MSK disorders between 1990 and 2017. (C) The EAPC in ASR of MSK disorders from 1990 to 2017. ASR, age-standardised incidence rate; EAPC, estimated annual percentage change; MSK, musculoskeletal.

Global MSK disorders incident cases by 5 causes and 23 GBD age groups. (A) Global MSK disorders incident cases by age for both sexes combined in 1990 and 2017. For each group, the left column shows case data in 1990 and the right column shows data in 2017. (B) Sex difference in global MSK disorders incident cases by age in 2017. GBD, Global Burden of Disease; LBP, low back pain; MSK, musculoskeletal; NP, neck pain; OA, osteoarthritis; RA, rheumatoid arthritis.

Global MSK disorders incident cases by five causes and regions for both sexes combined. (A) The MSK disorders incident cases by five causes and SDI regions, from 1990 to 2017. (B) The MSK disorders incident cases by five causes and by GBD regions, in 1990 and 2017. For each group, the left column shows case data in 1990 and the right column shows data in 2017. Certain regions are magnified to the top-right of the panel. LBP, low back pain; MSK, musculoskeletal; NP, neck pain; OA, osteoarthritis; RA, rheumatoid arthritis; SDI, sociodemographic Index.
The ASR of MSK disorders
The global ASR of MSK disorders was 4172.67 per 100 000 in 2017. It varies 2.57-fold across countries, with the highest rate in New Zealand (7355.47 per 100 000 in 2017) and the lowest rate in China (2864.49 per 100 000 in 2017, table 1, online supplementary table S6; figure 1A). However, it decreased by an average of 0.18% (95% CI −0.21% to −0.15%) during 1990–2017, with negative EAPC (95% CI) in China (−0.29, –0.39 to −0.19), India (−0.29, –0.41 to −0.17) and USA (−0.05, –0.07 to −0.13, table 1, online supplementary table S6; figure 1C). The EAPC (95% CI) for males and females was −0.17 (−0.20 to −0.13) and −0.19 (−0.22 to −0.16), respectively (table 1). For SDI regions, the decreasing trend in ASR was mainly in high-middle SDI regions (EAPC=−0.25; 95% CI −0.31 to −0.19), and was slightly in low and high SDI regions, but not in the low-middle and middle SDI regions during this period (table 1; figure 4A). For GBD regions, the ASR showed a stable or minor change in most regions over time, with the most significant increase observed in Andean Latin America (0.21, 0.19–0.23) and Western SSA (0.21, 0.15–0.27), and the most significant decrease in East Asia (−0.28, −0.38 to −0.18) and South Asia (−0.20, –0.28 to −0.12, table 1; figure 4A). Furthermore, through a hierarchy cluster analysis, the trend in ASR of MSK disorders in 195 countries and territories was divided into five categories. The detailed results are shown in the supplementary files (online supplementary figure S1).

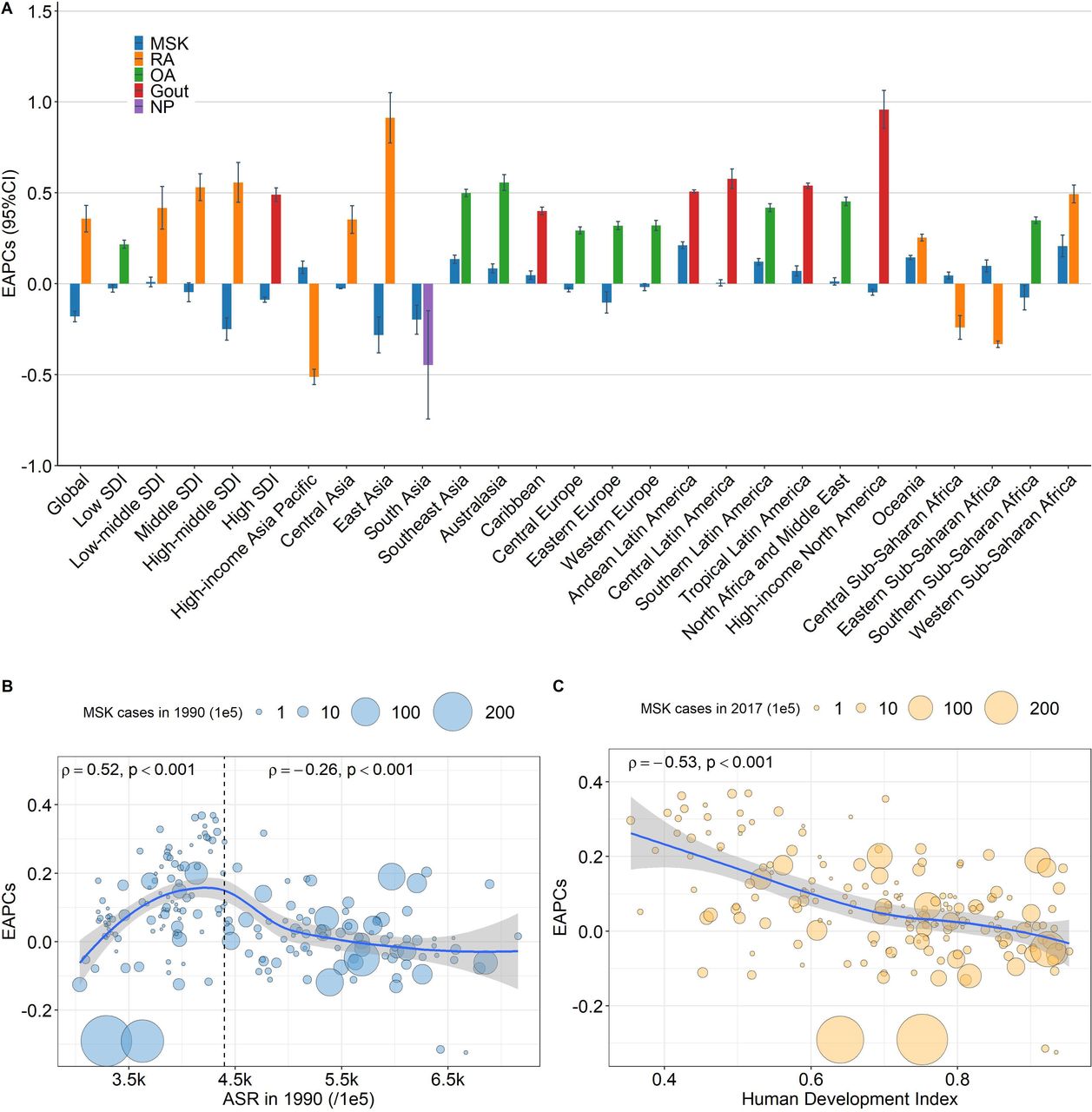
The EAPCs in ASR of MSK disorders from 1990 to 2017, at global, regional and national level for both sexes combined. (A) The EAPC in ASR of MSK disorders from 1990 to 2017, by causes and by region, for both sexes combined. Those EAPCs in each of the regions are presented as the overall and the absolute maximum caused by specific cause. The correlation between EAPC and ASR in 1990 (B), and between EAPC and HDI in 2017 (C) for MSK disorders. The incident cases from countries was represented by the circles and its size. The available HDI data can be matched with incident cases among 184 countries. ASR, age-standardised incidence rate; EAPC, estimated annual percentage change; HDI, human development index; LBP, low back pain; MSK, musculoskeletal; NP, neck pain; OA, osteoarthritis; RA, rheumatoid arthritis; SDI, sociodemographic index.
Incidence of MSK disorders by cause
LBP was the leading cause at the global and regional level, followed by NP, OA, gout and RA, accordingly for 73.4%, 19.5%, 4.5%, 2.2% and 0.4% of total incident cases in 2017, respectively (figure 5). During 1990–2017, incident cases for each cause increased, by between 52% for LBP and 102% for OA. However, ASR presented a different temporal trend, with the EAPCs (95% CI) for LBP, NP, RA, OA and gout of −0.24 (−0.29 to −0.20), −0.09 (−0.13 to −0.05), 0.36 (0.28 to 0.43), 0.32 (0.28 to 0.36) and 0.22 (0.21 to 0.23), respectively. The highest EAPC among five causes differed across regions, RA at the global level, in low-middle, middle and high-middle SDI regions, and seven GBD regions; OA in low SDI regions and eight GBD regions; gout in high SDI regions and five GBD regions; and NP in South Asia (figure 4A and online supplementary figure S17). The detailed information of incident cases, ASR and EAPC for each cause by age, sex, region and country and territory are described in online supplementary files.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Contribution of specific causes to MSK disorders incident cases, by regions for both sexes combined in 1990 and 2017. LBP, low back pain; MSK, musculoskeletal; NP, neck pain; OA, osteoarthritis; RA, rheumatoid arthritis.
Factors associated with incidence
A significant positive correlation (ρ=0.52, p<0.001) was observed between EAPC and baseline ASR (in 1990) for MSK disorders, when baseline ASR was below the break point of 4400 per 100 000. Such correlation turned negative for baseline ASR above 4400 per 100 000 (ρ=0.26, p<0.001, figure 4B). A significant negative correlation (ρ=−0.53, p<0.001) was found between EAPC and HDI (in 2017) for MSK disorders (figure 4C). The ASR was positively associated with HDI in the corresponding year (ρ=0.62, p<0.001 in 1990; ρ=0.53, p<0.001 in 2017) for MSK disorders (online supplementary figure S23). The cause-specific correlations are presented in online supplementary figures S18–S22, S24–S28.
Discussion
For the first time, we analysed the global trend of incidence for MSK disorders, overall and by the most five common causes at the global, regional and national level. From 1990 to 2017, the ASR of MSK disorders decreased by an annual average 0.18%, while the number of incident cases has increased by 58%. This pattern appears a major public health concern as the ASR has not been improved substantially. The magnitude of incident cases increased probably due to population growth and ageing. As the global population increased by 42% from 5.28 billion in 1990 to 7.51 billion in 2017, with the absolute annual change of the population of 82.93 million, and the proportion of the population aged 60 years or over increased from 9.16% in 1990 to 13.47% in 2015 from WHO.21
To our best knowledge, this is the first study to examine the associations of ASR and EAPC with HDI of countries. The ASR was positively associated with HDI in the same year, particularly for LBP, OA and RA. EAPC during 1990–2017 was associated with both baseline ASR and HDI in 2017 for MSK disorders, except for OA and NP.
Few studies have investigated the temporal trend in incidence of MSK disorders comprehensively. Findings cannot therefore be directly compared with those from previous studies. However, both the substantial increases in the number of incident cases and the temporal trend in ASR of MSK disorders in our study are consistent with the rising all-age counts and temporal trend in age-standardised rates of prevalence, DALYs and YLDs of MSK disorders in the past three decades.1 2 The GBD 2017 studies also indicated that the global number of all-age YLDs attributed to MSK disorders was increasing, while the percentage change in age-standardised YLDs was decreasing in 1990–2017.
The pattern of the temporal trends in ASR varied by cause. LBP dominated the trend of MSK disorders, with the ASR decreasing by 24% annually, which compares the increasing trend of ASR for RA, OA and gout, a relatively stable trend in ASR for NP. In line with the GBD study 2017, between 2007 and 2017, the global number of all-age YLDs attributed five causes also increased, while age-standardised YLDs rates decreased for LBP, remained stable for NP and increased for RA, OA and gout, respectively.1 2 A recent study reported a global increase of 8.2% in ASR for RA between 1990 and 2017, despite a simple estimate between two timepoints (1990 and 2017).22 Moreover, the contribution level of incident cases was consistent with the burden rank of each cause of MSK disorders on YLDs and DALYs.1 2 23 Those heterogeneous patterns are probably determined by the change in prevalence of different major risk factors over time. For example, with the rise of HDI worldwide, the major risk factors of LBP, such as social factors and occupational risks, have been modified during 1990–2017, especially in high HDI countries, which may attribute to the decreased trend in ASR. However, those major risk factors were not modified in low HDI countries, presenting an increased ASR, which might have a negative association between EAPC and HDI for LBP. Meanwhile, autoimmune conditions for RA cannot be easily modified, and obesity and dietary factors for OA and gout have shown an increase in both developed and developing countries.24–26
The pattern of the temporal trends in ASR varied across the world. For overall MSK disorders and LBP, the trends in ASR remained stable or slightly increased in low and low-middle SDI regions, although other SDI regions had a decreasing trend. The burden of MSK disorders increased by 60% in developing countries from 1990 to 2010.23 In low SDI regions, a downturn trend in ASR was observed for NP, while in high SDI regions, ASR of gout was on rise. Previous studies also reported between-country variances in prevalence and mortality, and their temporal changes of MSK disorders.1 25 The association between EAPC and HDI varied by cause. Not all the patterns of associations were simplistic and linear. There are variations of change in major risk factors by cause and substantial variations of different health system performance in the different countries or regions, even within the same level of HDI.24–27 The prevention and treatment appeared to be more robust in these countries with not only high ASR, but also high EAPC.
Our findings show sex differences in global incident cases and ASR for MSK disorders by cause, with slightly higher in women than men at all ages for MSK disorders, LBP, NP and OA. It is promising that the gap between sexes is narrowing, as the decreasing trend of ASR is steeper among females for MSK disorders and LBP, and the increasing trend of ASR is smaller among females for OA. Consistent with findings from the literature, sex differences were obvious in incident cases and ASR for RA and gout.28 29 The increasing trend of ASR is more apparent among women than men for RA and gout. Consequently, females experience higher prevalence and YLD rates from RA, and so do males from gout.9 13 22 Of several explanations suggested for this sex disparity, biological and hormonal factors may play an important role in aetiology across women’s life course, including oestrogen and progesterone, and events such as pregnancy, postpartum period, breastfeeding and menopause.30
Several limitations should be noted for this study. In nature, this study is a secondary data analysis from the GBD study. As with issues existing for many diseases from the GBD study, the accuracy of the results for MSK disorders largely depends on the quality and quantity of input data to the models. There are no comparable studies, so the findings in this study cannot be externally validated. The incidence of many other MSK disorders is not included in the current study due to lack of data. This may be warranted in the future GBD estimates. Last but not least, the effect of the different health systems in the different countries or regions was not evaluated, as substantial variations in health gains exist even between countries within the same HDI.2 27 Despite these limitations, this study is nevertheless the first one to comprehensively assess the incidence and trends of MSK disorders at global, regional and national level. The results can serve as a baseline for relevant policies, programme design and follow-up studies.
MSK disorders share common risk factors with other chronic, non-communicable diseases, such as inadequate physical activity, obesity, smoking, alcohol drinking, unhealthy diet or poor nutrition, and genetic factors.26 Prevention programmes focused on modifiable risk factors should be as an important approach to controlling MSK disorders. Evidence-based strategies to reduce four major risk factors in the community include, maintaining an ideal weight, being physically active, having a balanced diet, avoid smoking and restricting alcohol drinking.24 31–33 Moreover, exercise therapy offers significant benefit for adults with MSK pain and is recommend for patients with NP and LBP in clinical practice guidelines.34 In addition, special preventive measures for MSK disorders should include the environment improvement and avoidance of repetitive activities.24 26
Conclusions
MSK disorders remain a major public health concern worldwide, despite of an overall decreasing trend in ASR. The global ASR shows an increasing trend for RA, OA and gout and remains stable for NP from 1990 to 2017. The findings in this study should inform the trend analysis of the global disease burden of specific MSK disorders and for the development of appropriate policies focusing on those modifiable risk factors.
Acknowledgments
We would like to thank Institute for Health Metrics and Evaluation and its cooperative organisations for making the GBD study data public.
References
Footnotes
JZ and LS are joint senior authors.
Handling editor Josef S Smolen
JZ and LS contributed equally.
Contributors ZJ, JZ and LS helped in the study conception and design. Acquisition of data and analysis and drafting of the article was performed by ZJ. DW, HZ, JL, XF, JZ and LS helped in revising the article. All authors have finally approved the submitted version to be published.
Funding Bill and Melinda Gates Foundation funded the GBD study, but did not fund this study. This study was supported by the Major International (Regional) Joint Research Project (No. 81720108020), the Jiangsu Province Major Research and Development Programme (No. BE2015602), Jiangsu Province 333 Talent Grant (No. BRA2016001) and the National Key Research and Development Programme of China (No. 2017YFC0909003).
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. We downloaded data from the Global Health Data Exchange (GHDx) query tool (http://ghdx.healthdata.org/gbd-2017).