Article Text

Abstract
Objective Investigate whether the efficacy and safety of intravenous tocilizumab (TCZ) demonstrated at week 52 in patients with early rheumatoid arthritis (RA) are maintained to week 104.
Methods Methotrexate (MTX)-naive patients with early progressive RA were randomly assigned to double-blind 4 mg/kg TCZ+MTX, 8 mg/kg TCZ+MTX, 8 mg/kg TCZ+placebo or placebo+MTX for 104 weeks. Patients not receiving 8 mg/kg TCZ and not achieving Disease Activity Score-28 joints (DAS28-erythrocyte sedimentation rate (ESR)) ≤3.2 at week 52 switched to escape therapy (8 mg/kg TCZ+MTX). Analyses were exploratory.
Results Intent-to-treat and safety populations included 1157 and 1153 patients, respectively. DAS28-ESR remission (<2.6) rates were maintained from weeks 52 to 104 (eg, 8 mg/kg TCZ+MTX, 49.3% to 47.6%). Placebo+MTX and 4 mg/kg TCZ+MTX escape patients' week 104 response rates were 51.4% and 30.5%, respectively. Inhibition of radiographic progression was maintained with 8 mg/kg TCZ (eg, 8 mg/kg TCZ+MTX mean (SD) change from baseline in modified total Sharp score: 0.13 (1.28), week 52; 0.19 (2.08), week 104). The safety profile of TCZ was consistent with that of previous reports.
Conclusions Patients with early RA treated with TCZ monotherapy or TCZ+MTX maintained clinical benefits during their second year of treatment with no new safety signals.
Trial registration number: NCT01007435; Results.
- DMARDs (biologic)
- Early Rheumatoid Arthritis
- Methotrexate
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Early intensive treatment, including addition of a biological agent to conventional synthetic disease-modifying antirheumatic drugs (DMARDs), is recommended for patients with rheumatoid arthritis (RA) and features of poor prognosis.1 ,2 Tocilizumab (TCZ), an interleukin-6 receptor-alpha inhibitor, has demonstrated safety and efficacy in combination with DMARDs in patients with RA and inadequate response to DMARDs3–6 and as monotherapy in patients with RA.7–9 The multicentre, 2-year, double-blind, double-dummy, randomised, parallel-group, phase III FUNCTION trial investigated the efficacy and safety of TCZ in combination with methotrexate (MTX) and as monotherapy in patients with early, active, progressive RA who were MTX-naive.10 The week 52 analysis showed that compared with MTX, TCZ+MTX or TCZ significantly improved rates of remission according to Disease Activity Score based on 28 joint counts and erythrocyte sedimentation rate (DAS28-ESR <2.6). TCZ+MTX also inhibited joint damage progression and improved physical function at 52 weeks compared with MTX.10
This analysis investigated whether previously reported clinical benefits and safety profiles of TCZ were maintained through 104 weeks of double-blind treatment.
Patients and methods
Patient populations and methods of this trial have been described.10 Briefly, MTX-naive patients (≥18 years old) with moderate to severe, active,11 early (≤2 years) RA were randomly assigned (1:1:1:1) to 8 mg/kg TCZ+MTX, 4 mg/kg TCZ+MTX, 8 mg/kg TCZ+placebo (TCZ monotherapy) or placebo+MTX. TCZ+placebo was administered intravenously every four weeks. MTX was administered as oral capsules starting at 7.5 mg/week to a maximum of 20 mg/week at week 8 if they had swollen or tender joints (see online supplementary appendix table S1 for mean MTX doses). Randomisation was stratified by serological status (presence of rheumatoid factor (RF) and/or anticyclic citrullinated peptide (anti-CCP) antibodies) and geographical region.
supplementary data
Inclusion criteria included DAS28-ESR >3.2, ESR ≥28 mm/h or C reactive protein (CRP) ≥1 mg/dL, seropositivity for RF or anti-CCP antibodies and RA-associated erosion in ≥1 joint. Data were collected until the end of the double-blind treatment (week 104) and the 8-week safety follow-up. At week 52, patients receiving 4 mg/kg TCZ+MTX or placebo+MTX who had not achieved low disease activity (LDA; DAS28-ESR ≤3.2) were switched to 8 mg/kg TCZ+MTX (escape therapy) and analysed under their originally assigned treatment groups in a separate postescape subanalysis, re-baselined at the time of escape.
Assessments
Efficacy was assessed in the intent-to-treat (ITT) population (randomly assigned patients who received ≥1 dose of TCZ/placebo) by evaluating DAS28-ESR remission (<2.6) and LDA; American College of Rheumatology (ACR)20/50/70 responses; Clinical Disease Activity Index (CDAI) remission (<2.8); ACR/European League Against Rheumatism (EULAR) Boolean remission (tender joint count (68) ≤1, swollen joint count (66) ≤1, Patient Global Assessment of Disease Activity visual analogue scale (VAS, cm) ≤1 and CRP ≤1 mg/dL) and index remission (Simplified Disease Activity Index (SDAI) ≤3.3); radiographic measures (van der Heijde–modified total Sharp score (vdH mTSS), erosion score and joint space narrowing score). Baseline and week 52 radiographs were reread by the joint assessor along with the week 104 radiographs; a baseline radiograph and at least one postbaseline time point had to be available for a patient to be included in the analysis. The study used two assessors, but a third assessor adjudicated in cases where scores did not match. All X-rays were blinded to order and treatment group. Serum TCZ levels and neutralising anti-TCZ antibodies were measured regularly through week 104, including withdrawal (see online supplementary appendix).
Safety was assessed in the safety population (all patients who received ≥1 TCZ+placebo infusion and had ≥1 postdose safety assessment). Adverse events (AEs) and serious AEs (SAEs) were reported. All analyses were exploratory; no statistical analyses were performed to compare treatment arms at week 104.
Results
Patients
Of 1162 randomly assigned patients, 1157 were included in the ITT population and 1153 in the safety population; 809 (69.6%) completed week 104 (see online supplementary appendix figure S1). At week 52, 33% (95/290) of patients receiving 4 mg/kg TCZ+MTX and 49% (142/289) receiving placebo+MTX switched to escape therapy with 8 mg/kg TCZ+MTX. Demographics and disease characteristics at baseline were similar across treatment arms in the ITT population10 and in escape patients (see online supplementary appendix table S2).
Efficacy
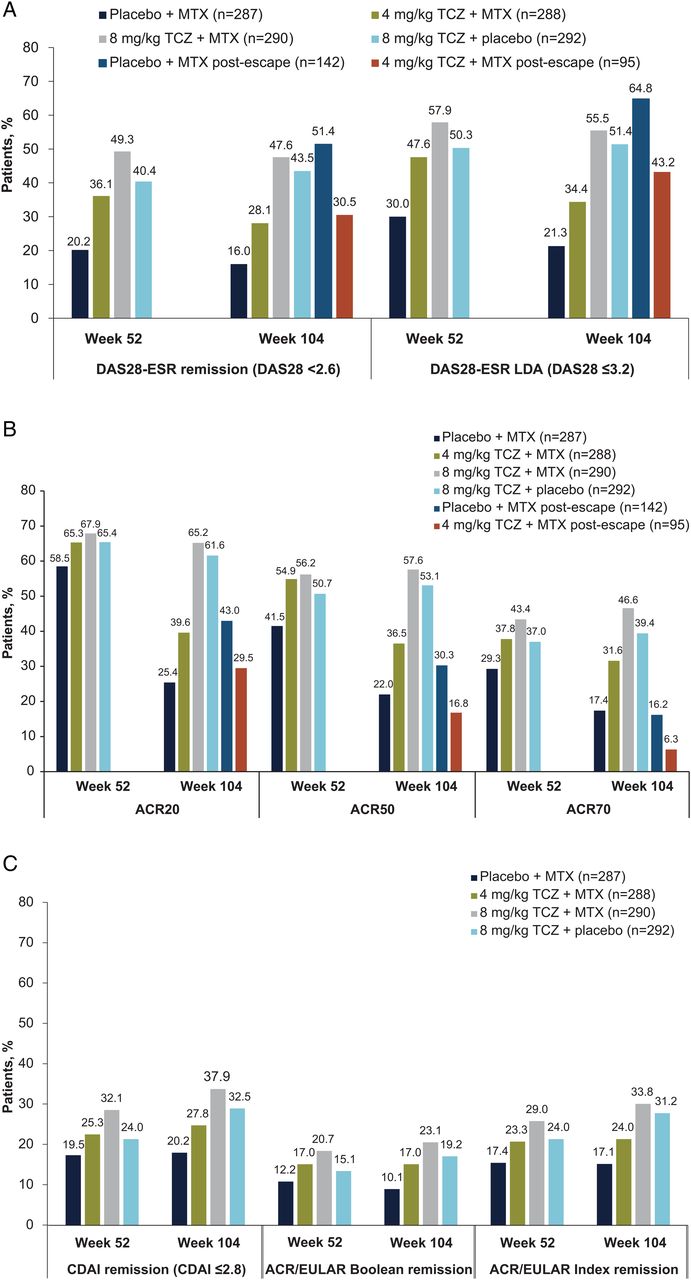
DAS28-ESR remission rates were maintained from weeks 52 through 104 (figure 1A). DAS28-ESR remission was achieved by 49.3% (143/290) of patients in the 8 mg/kg TCZ+MTX group at week 52 and by 47.6% (138/290) at week 104, and DAS28-ESR LDA was achieved by 57.9% (168/290) and 55.5% (161/290), respectively (figure 1A). Proportions of patients who lost DAS28-ESR LDA (DAS28-ESR >3.2 at two consecutive visits) after week 52 were 4.2% (7/168) in the 8 mg/kg TCZ+MTX group and 4.8% (7/147) in the 8 mg/kg TCZ monotherapy group. Proportions of patients achieving ACR20, ACR50 and ACR70 responses were similar at weeks 52 and 104 in the 8 mg/kg TCZ monotherapy and 8 mg/kg TCZ+MTX groups (figure 1B). After 52 weeks of escape therapy, 30.5% (29/95) and 51.4% (73/142) of patients who originally received 4 mg/kg TCZ+MTX and placebo+MTX, respectively, achieved DAS28-ESR remission (figure 1A). ACR20, ACR50 and ACR70 response rates after 52 weeks of escape therapy were 43.0%, 30.3% and 16.2%, respectively, in the placebo+MTX escape group and 29.5%, 16.8% and 6.3%, respectively, in the 4 mg/kg TCZ+MTX escape group (figure 1B). Similar proportions of patients in each initial treatment arm achieved remission according to CDAI and ACR/EULAR Boolean and Index criteria at weeks 52 and 104 (figure 1C).
{kind=link}
Proportions of patients achieving (A) Disease Activity Score based on 28 joint counts and erythrocyte sedimentation rate (DAS28-ESR) remission or low disease activity (LDA), (B) ACR20/50/70 responses at weeks 52 and 104 or (C) Clinical Disease Activity Index (CDAI) remission, American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) Boolean remission or ACR/EULAR Index remission (intent-to-treat (ITT) population). For DAS28 and ACR, last observation carried forward (LOCF) was used for missing tender and swollen joint counts. No imputation was used for missing ESR, Patient Global Assessment of Disease Activity visual analogue scale, Health Assessment Questionnaire–Disability Index score or C reactive protein (CRP). ESR was used if CRP was missing for assessment of ACR response. For CDAI, data collected after withdrawal or initiation of escape therapy were set to missing, and LOCF was used for missing data. Patients who received escape therapy or withdrew prematurely or for whom a DAS28 score, ACR response or EULAR response could not be calculated were considered non-responders. Postescape data at week 104 were based on the postescape baseline and represented 52 weeks of 8 mg/kg tocilizumab (TCZ)+ methotrexate (MTX) escape therapy. SDAI, Simplified Disease Activity Index.
Inhibition of radiographic progression was maintained between weeks 52 and 104 for both 8 mg/kg TCZ groups and was numerically greater in the 8 mg/kg TCZ+MTX group. The mean (SD) change from baseline in vdH mTSS was 0.13 (1.28) at week 52 and 0.19 (2.08) at week 104 for the 8 mg/kg TCZ+MTX group (table 1). The annualised progression rate (APR) for vdH mTSS was numerically lower for the TCZ groups than the placebo+MTX group in the first and second years and between baseline and week 104. The vdH mTSS APR decreased in patients who switched to escape therapy (see online supplementary appendix table S3).
Radiographic endpoints (intent-to-treat population)
Post hoc analysis of efficacy at week 104 according to achievement of DAS28-ESR LDA at week 52 suggested that in the TCZ groups some week 52 non-responders achieved responses at week 104; for example, 14–17% of week 52 LDA non-responders achieved remission at week 104 (see online supplementary appendix table S4).
Pharmacokinetics
Mean predose serum TCZ concentrations over time were similar for both 8 mg/kg TCZ groups (see online supplementary appendix figure S2).
Safety
Eighty-three SAEs were reported in the 8 mg/kg TCZ+MTX group compared with 67, 58 and 31 for the 8 mg/kg TCZ+placebo, 4 mg/kg TCZ+MTX and placebo+MTX groups, respectively (table 2). Rates (95% CI) of SAEs per 100 patient-years (PY) were 11.6 (9.2 to 14.3), 13.3 (10.3 to 16.9), 14.7 (11.2 to 19.0) and 9.1 (6.2 to 13.0), respectively. Most AEs were mild or moderate in intensity (96–97% across the four treatment groups). Infections were the most frequently reported AEs/SAEs in all treatment arms, with AE rates (95% CI) per 100 PY ranging from 89.4 (82.6–96.6) for 8 mg/kg TCZ+MTX to 113.3 (103.0–124.3) for 4 mg/kg TCZ+MTX.
Safety at week 104 (safety population)
Fourteen deaths occurred during the study: nine in the first year10 and five in the second year (none on escape therapy). Causes of second-year deaths included duodenal ulcer haemorrhage in a patient receiving 4 mg/kg TCZ+MTX, interstitial lung disease and endometrial cancer in patients receiving 8 mg/kg TCZ+MTX and congestive heart failure and metastatic cancer in patients receiving 8 mg/kg TCZ+placebo (see online supplementary appendix table S5). Switching to escape therapy did not impact the incidence or rate of AEs (see online supplementary appendix table S6).
Immunogenicity
Nine patients tested positive for neutralising anti-TCZ antibodies (8 mg/kg TCZ+MTX, n=2; 8 mg/kg TCZ+placebo, n=2; 4 mg/kg TCZ+MTX, n=5), though none withdrew from treatment because of insufficient therapeutic responses.
Discussion
FUNCTION is the first study of TCZ initiated in patients with early RA. Year 2 results show that the efficacy of TCZ10 was maintained for extended treatment periods; patients with early RA who received 8 mg/kg TCZ+MTX or 8 mg/kg TCZ monotherapy exhibited sustained improvement in disease activity and maintained inhibition of joint damage during their second year of treatment. In both 8 mg/kg TCZ groups, week 52 improvements were maintained through week 104 for DAS28-ESR remission and LDA, ACR 20/50/70 responses and radiographic progression. The best responses were consistently observed in the 8 mg/kg TCZ+MTX group, particularly for radiographic endpoints. Maintenance of response with 8 mg/kg TCZ monotherapy suggests that early TCZ therapy is a viable option for patients intolerant of MTX. Some patients in the TCZ groups who did not achieve DAS28-ESR LDA by week 52 achieved remission by week 104 in a post hoc analysis, suggesting that longer treatment may be required to observe efficacy in some patients.
In escape patients who received 4 mg/kg TCZ+MTX or placebo+MTX in the first year and 8 mg/kg TCZ+MTX in the second year, further efficacy improvements were generally observed from escape through week 104 for DAS28-ESR, ACR and radiographic endpoints. Although comparable DAS28-ESR remission rates were observed between escape patients who received 8 mg/kg TCZ+MTX in the second year and patients who received 8 mg/kg TCZ+MTX throughout, ACR response rates were lower and the overall degree of joint damage was greater in escape patients, highlighting the importance of early initiation of therapy.
Improvements in the placebo+MTX escape group were comparable to those of patients receiving 8 mg/kg TCZ throughout. Serum TCZ concentrations were maintained at similar levels between the 8 mg/kg TCZ+placebo and 8 mg/kg TCZ+MTX groups, indicating that, in contrast to adalimumab,12 MTX does not appear to have an additive effect on serum drug levels. Only nine patients tested positive for neutralising anti-TCZ antibodies, none of whom withdrew because of insufficient therapeutic response or loss of efficacy, consistent with previous reports.13
Because of the complexity of multiple comparisons, all week 104 analyses were exploratory, which is a limitation of this study. Post-week 52 data for the 4 mg/kg TCZ+MTX and placebo+MTX groups should be interpreted with caution given the large number of patients switching to escape therapy. This meant the data were enriched for patients who achieved DAS28 LDA at week 52 for endpoints at which escape patients were set to missing and possibly underestimated for endpoints at which they were considered non-responders.
The most common AEs/SAEs in all groups were infections. Although there was no clear difference in the rate of infections between the TCZ and placebo+MTX groups, the rate of serious infections was numerically higher with TCZ (95% CIs overlapping). Rates of infection and serious infection did not appear to increase over time. Safety was consistent with the known TCZ safety profile. The low incidence of gastrointestinal perforations may reflect less exposure to non-steroidal anti-inflammatory drugs and corticosteroids. No new safety signals were identified in this MTX-naive patient population with early RA.
Acknowledgments
The first draft of the manuscript was prepared by the authors, with professional writing and editorial assistance provided by Jennifer Adlington, PhD, Sara Duggan, PhD, and Meryl Mandle, who provided writing services on behalf of F. Hoffmann-La Roche.
References
Footnotes
Handling editor Tore K Kvien
Contributors GRB and WFR contributed to the conception and design of the study. GRB, WFR, RFvV, JK, AR-R and RB contributed to data acquisition. GRB, WFR, RFvV, JK, AR-R, RB, AK and SD analysed and interpreted the data. GRB, WFR, JK, AK and SD drafted the manuscript. All authors revised the manuscript critically for important intellectual content. All authors contributed to, reviewed and approved the final manuscript. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This study was funded by Roche. Funding for manuscript preparation was provided by F. Hoffmann-La Roche Ltd.
Competing interests GRB has received honoraria from Roche for lectures and consulting. WFR reports grants and personal fees from Roche outside the submitted work. RFvV reports grants from Roche during the conduct of the study; grants from AbbVie, Amgen, BMS, GSK, Pfizer, Roche, UCB; and personal fees from AbbVie, Biotest, BMS, Celgene, Crescendo, GSK, Janssen, Lilly, Merck, Novartis, Pfizer, Roche, UCB, and Vertex outside the submitted work. JK reports grants and personal fees from AbbVie, Eli Lilly and Company, Genentech, Pfizer, Roche Laboratories and UCB; and personal fees from Amgen, Boehringer Ingelheim GmbH, Bristol-Myers Squibb Company, Crescendo Bioscience, Epirus Biopharmaceuticals, GlaxoSmithKline, Hospira, Janssen Biotech, Merck Sharp & Dohme, Novartis Pharmaceuticals, Regeneron Pharmaceuticals, Samsung Bioepis and Sandoz outside the submitted work. AR-R reports personal fees from Roche and Chugai during the conduct of the study and personal fees from Pfizer, Lilly, BMS, AbbVie, MSD, UCB, Janssen, Sanofi and Boehringer outside the submitted work. RB reports grants from Roche, Merck Sharp & Dohme and AbbVie outside the submitted work. AK is an employee of Genentech. SD is an employee of Roche Products.
Patient consent Obtained.
Ethics approval This trial was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice and was approved by the Institutional Review Board/Independent Ethics Committee governing each site.
Provenance and peer review Not commissioned; externally peer reviewed.