Article Text

Abstract
Objectives The aim of this study was to determine whether antibodies to infliximab (IFX) in Remicade-treated patients cross-react with the biosimilar CT-P13.
Methods 250 consecutive patients with rheumatic diseases under Remicade and 77 controls were retrospectively selected for the study. Anti-IFX antibodies at drug through levels were measured in parallel with three different bridging ELISA assays: Promonitor-ANTI-IFX kit, which uses Remicade to detect antibodies, and two more assays that use either Inflectra or Remsima with the same format. Correlation and association between each assay was studied.
Results 50.4% of patients were tested positive with Promonitor-ANTI-IFX. All were antibodies to IFX (ATI)-positive when either Inflectra or Remsima assays were used. In all comparisons positive and negative percentage agreements were 100%, and correlation coefficients were ≥0.995. No differences between rheumatoid arthritis and spondyloarthritis, or between concomitant immunosuppressives, were observed.
Conclusions Anti-IFX antibodies of Remicade-treated patients cross-react with either Inflectra or Remsima. Although additional epitopes may be present in the biosimilar, results suggest that epitopes influencing the immune response to IFX are also present in the biosimilar. Antibody-positive patients treated with Remicade should not be switched to the biosimilar, since antibodies will interact with the new drug and potentially lead to loss of response. This finding supports the utility for therapeutic drug monitoring before a switching strategy is considered.
- Treatment
- Rheumatoid Arthritis
- Anti-TNF
- Spondyloarthritis
Statistics from Altmetric.com
Introduction
The introduction of biosimilars with similar efficacy and safety to the innovator drugs may benefit the treatment of rheumatic diseases through reduced costs. Infliximab (IFX) is an innovator antitumour necrosis factor α (anti-TNFα) marketed under the name of Remicade (RMC). The biosimilar CT-P13, branded as Inflectra (IFT) and Remsima (RMS), was approved in 2013 by the European Medicines Agency for use across all indications of RMC.1–3 However, the first anti-TNFα biosimilar still raises concerns among clinicians. One of the main questions is whether patients treated with RMC can be safely and effectively switched to the biosimilar.
Proving immunogenicity equivalence between the innovator and the biosimilar is essential. The detection of antidrug antibodies (ADA) was similar in CT-P13 and innovator treatment groups in rheumatoid arthritis (RA) and ankylosing spondylitis.4 ,5 A recent work has shown that antibodies to RMC in patients with inflammatory bowel disease (IBD) similarly recognise and cross-react with RMS.6
Patients and methods
Patients and serum samples
All patients (250) had RA and spondyloarthritis (SpA) under standard RMC treatment (3 and 5 mg/kg intravenous infusion for RA and SpA, respectively at 0, 2 and 6 weeks and then every 8 weeks thereafter) (Janssen Biotech, USA), and had never been exposed to the biosimilar. Patients reported positive to antibodies to IFX (ATI) during routine testing since 2013 were consecutively included (126). Similarly, a balanced population of ATI-negative patients (124) was selected (table 1). Additionally, three IFX-naïve control populations were included for cut-point calculations.7 The study was approved by the ethics committees of La Paz (Madrid, Spain) and Marina Baixa (Alicante, Spain) hospitals. Trough sera were collected, and stored at −80°C until measurement.
Clinical characteristics of the study population
ATI assays
ATI were detected using a bridging ELISA as described previously.8 ,9 Three assay settings were used, one with each drug, to cross-link ATI: assay #1 that uses RMC (Promonitor-ANTI-IFX CE marked kit, Progenika-Grifols, Spain); assay #2 that uses RMS (Orion Pharma, Norway); assay #3 that uses IFT (Hospira, USA). All three assays showed identical analytical performance (LOQ 2 AU/mL). No interference was observed when rheumatoid factor was added to serum up to 172 U/mL, although interference above this level cannot be excluded.
Statistical analysis
Continuous variables were tested for normality by Shapiro–Wilk and Mann–Whitney rank sum tests. Correlation coefficients were determined by Spearman’s correlation test. Positive (PPA) and negative (NPA) percent agreements between tests were determined. A p value <0.05 was considered statistically significant.
Results
Overall 327 individuals participated in the study, 250 were rheumatic patients undergoing RMC treatment and 77 were control individuals (table 1).
Assay cut-point determination
A total of 37 serum samples from IFX-naïve rheumatic patients and 21 sera from healthy donors were analysed with the three assays to determine assay cut-points and allow assay interpretation and comparison.7 There were no statistically significant differences between mean optical density (OD) values obtained in assay #1 (0.095±0.055), #2 (0.121±0.096) and #3 (0.103±0.065) (figure 1A). The cut-point was defined as the mean OD value plus 10 SD. Cut-point value for the three assays was calculated to be 5 AU/mL.
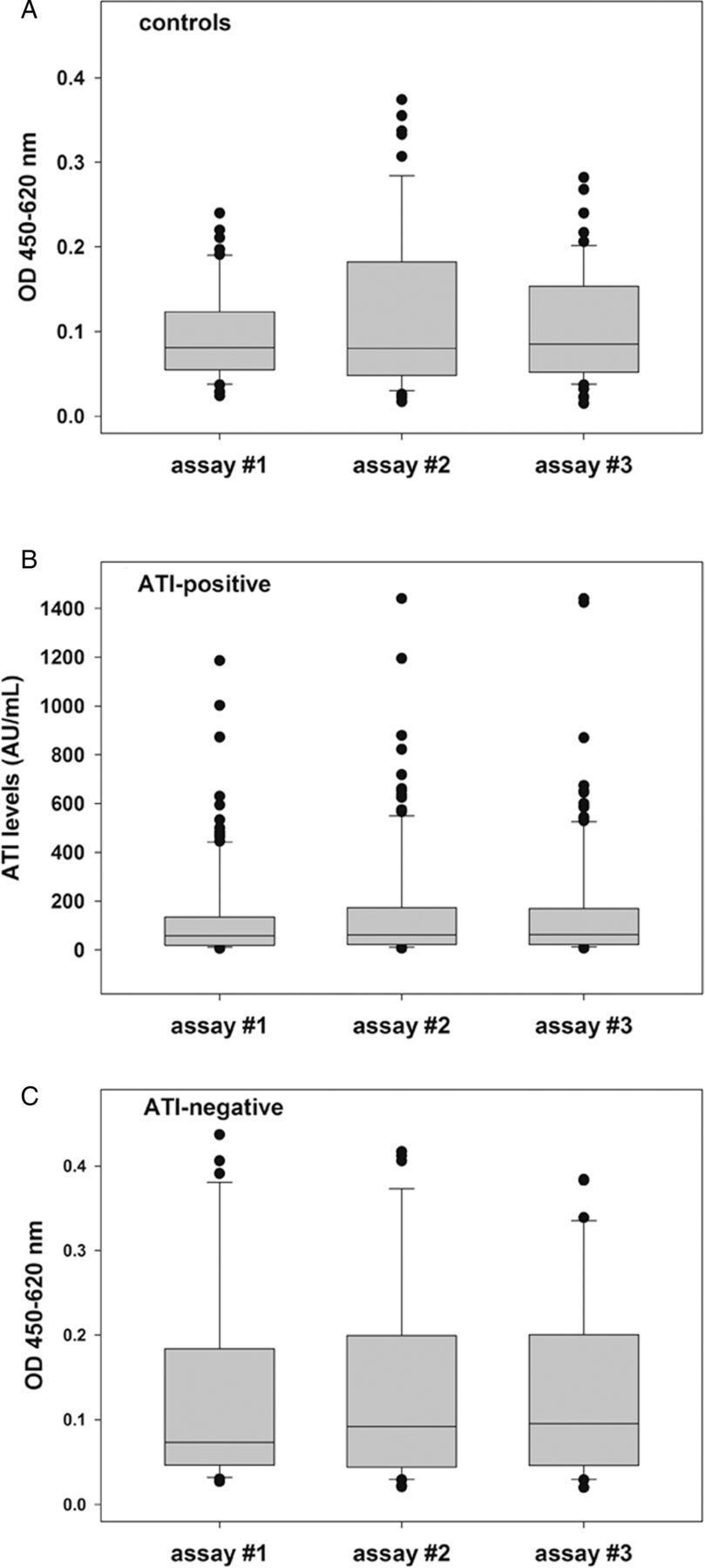
Box plots of (A) signals of Infliximab (IFX)-naïve rheumatic patients and IFX-naïve healthy controls (n=58), (B) antibodies to IFX (ATI)-positive levels (n=126) and (C) signals of ATI-negative samples (n=124), measured with the three assays.
ATI determination towards RMC
A total of 250 patients were tested for ATI using assay #1. Results showed that 126 (50.4%) were positive to ATI and median antibody concentration determined was 57.8 AU/mL (figure 1B). All patients tested positive for ATI had undetectable levels of IFX (p<0.001). Median IFX concentration in ATI-negative patients was 1.7 µg/mL (see online supplementary figure S1).
Supplementary figure 1
IFX concentration distribution in ATI-negative samples
Cross-reactivity between ADA and the biosimilar
Patients were tested to evaluate whether antibodies cross-reacted with IFT and RMS. All patients tested ATI-positive in assay #1 (n=126) were found positive when either RMS or IFT was used to detect the antibodies. The differences between the median ATI concentrations obtained in assay #1 (57.8 AU/mL), #2 (61.5 AU/mL) and #3 (62.1 AU/mL) were not statistically significant (p>0.05, analysis of variance test) (figure 1B). No significant differences in occurrence of antibodies to RMC were observed between patients with RA and patients with SpA (p>0.05). No differences in ATI among patients with concomitant immunosuppressive therapy (methotrexate vs others) was observed, neither between patients with nor without concomitant immunosuppressives.
All patients who tested ATI-negative in assay #1 (n=124) were negative in assay #2 and #3. There were no statistically significant differences between median OD values obtained in assay #1 (0.074), #2 (0.092) and #3 (0.096) (figure 1C) or when compared with the control population (OD median values 0.081, 0.080 and 0.085 for assay #1, #2 and #3, respectively).
Nineteen patients with RA and SpA under active treatment with adalimumab (ADL) and anti-adalimumab antibody (AAA)-positive were tested negative for ATI with the three assays.
Spearman's correlation test was used to study the association between the assays. There was an excellent correlation in ATI levels determined between assays #1 vs #2 (0.991, p<0.001), assays #1 vs #3 (0.993, p<0.001) and assays #2 vs #3 (0.996, p<0.001) (figure 2). PPA and NPA were 100% across all assays (figure 2). Bias between each pair of the methods was assessed by Bland–Altman analysis. No significant difference in bias was found when comparing assay #1 with either assay #2 (33.9±80.1 AU/mL) or #3 (26.8±62.6 AU/mL) indicating that either assay could be used in a clinical setting to detect ATIs (see online supplementary figure S2).

{kind=link}
{kind=link}
Dot plots of Spearman's correlation of antibodies to IFX (ATI) levels and contingency tables between (A) assay #1 and #2, (B) assay #1 and #3 and (C) assay #2 and #3.
Discussion
In the present study, we evaluated the cross-reactivity of ATI in rheumatic patients by using three bridging ELISA assays. Bridging ELISA is a well-validated and clinically useful technique for biological drug monitoring,10–12 although some limitations should be noted like the low drug tolerance and impossibility to detect IgG4. Our results showed that all antibodies developed in patients treated with RMC did cross-react with either IFT or RMS. Moreover, antibody concentrations determined were similar in all cases, and an excellent correlation was found between the assays. It has been described that ATI can persist in the blood years after IFX is discontinued.13 In the case of loss of response many patients can be switched to ADL, which can also induce an immune response. Since the immune response is drug specific (and mostly anti-idiotypic), ATI will not interact with ADL. Here we have extended these observations by analysing an additional control population consisting of AAA-positive patients. Results confirmed that AAA do not cross-react with RMC or CT-P13 in rheumatic patients providing reassurance of safety of switching between ADL and CT-P13.6
Altogether, these results suggest that the epitopes raising the immune response to the innovator drug are responsible for the same degree of reactivity when sera are confronted to the biosimilar molecule, although it must be noted that the biosimilar might present new epitopes due to different glycosylation pattern or impurities, and even conformational epitopes due to potential aggregations. Contrary to Ben-Horin's work we have not observed any increment in the background signal of assays using CT-P13 compared with RMC in the control population. In their work authors hypothesise that those slight but significantly higher signals to RMS in IFX-naïve patients could be due to minute differences in the aggregate content of the drug. One explanation for this discrepancy is that aggregates are formed depending on the reconstitution or handling process instead of being a property inherent to each drug.
Findings imply that ATI-positive patients treated with RMC should not be considered for switching to a biosimilar treatment, since pre-existing ATI will interact with the new drug, enhance clearance and potentially lead to loss of response and infusion-related reactions. Of course, further studies with biosimilar-treated patients are warranted to increase our knowledge about potentially different immunogenic responses.
In addition, RA and SpA are characterised by different clinical manifestations and inflammatory burden, so the magnitude of the immune response can differ between both diseases. However, we did not detect any significant differences in the magnitude of ATI between RA and SpA with any of the assays used, suggesting that the repertoire of the polyclonal response against RMC is the same.
It must be noted that we have not analysed potential differences in the specificity of the antibody titre, that is, different antibodies targeting the Fab or Fc regions of IFX. However, it has been previously described that the majority of ATI are directed to the idiotype of the drug using a TNF competition radioimmunoassay.14 Although in our study we use a bridging ELISA format, we cannot rule out differences in the immunogenicity between the innovator and the biosimilar, and therefore a strong contribution of the Fc region should not be expected.
As described above the vast majority of ADA to anti-TNF blockers elicit a restricted anti-idiotypic antibody response in rheumatic patients resulting in functional neutralisation.15 More than 90% of ATI and more than 97% of AAA, golimumab or certolizumab have been reported as neutralising.14 We have also observed the same phenomenon in all samples where we use assay #1 followed by a confirmatory assay consisting of spiking different concentrations of human TNF to the ATI-positive samples. Since all assays used in this study report similar ATI concentrations (regardless of the use of RMC, RMS or IFT), we conclude that a significant impact of ADA binding activity (either neutralising or non-neutralising) is unlikely.
Results also demonstrate that Promonitor-ANTI-IFX test can be used to monitor ATI in biosimilar-treated patients. This study demonstrates for the first time identical reactivity of ATI towards RMC and biosimilar molecules in patients with rheumatic diseases. Results are in agreement with previous data in patients with IBD in which ATI were shown to be cross-reactive with RMS. This finding supports the utility for therapeutic drug monitoring before a switching strategy is considered.
Acknowledgments
The authors thank Simon Santa Cruz for critical review of the manuscript.
References
Footnotes
Handling editor Tore K Kvien
Contributors All authors have contributed to the study design. DP-S, AM-F, TJ, CP, AB, FL-T and JR have contributed to patient recruitment and sample collection. MBR-A, AM, ARdA, NT, AM and DN have contributed to sample and data analysis, and result interpretation. All authors have contributed to discussion of results.
Competing interests MBR-A, AM, ARdA, NT, AM and DN are full-time employees of Progenika Biopharma S.A.
Patient consent Obtained.
Ethics approval The ethics committees from La Paz University Hospital and Marina Baixa Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.