Article Text

Abstract
Objectives Extension of disease beyond the atrioventricular (AV) node is associated with increased mortality in cardiac neonatal lupus (NL). Treatment of isolated heart block with fluorinated steroids to prevent disease progression has been considered but published data are limited and discordant regarding efficacy. This study evaluated whether fluorinated steroids given to manage isolated advanced block prevented development of disease beyond the AV node and conferred a survival benefit.
Methods In this retrospective study of cases enrolled in the Research Registry for NL, inclusion was restricted to anti-SSA/Ro-exposed cases presenting with isolated advanced heart block in utero who either received fluorinated steroids within 1 week of detection (N=71) or no treatment (N=85). Outcomes evaluated were: development of endocardial fibroelastosis, dilated cardiomyopathy and/or hydrops fetalis; mortality and pacemaker implantation.
Results In Cox proportional hazards regression analyses, fluorinated steroids did not significantly prevent development of disease beyond the AV node (adjusted HR=0.90; 95% CI 0.43 to 1.85; p=0.77), reduce mortality (HR=1.63; 95% CI 0.43 to 6.14; p=0.47) or forestall/prevent pacemaker implantation (HR=0.87; 95% CI 0.57 to 1.33; p=0.53). No risk factors for development of disease beyond the AV node were identified.
Conclusions These data do not provide evidence to support the use of fluorinated steroids to prevent disease progression or death in cases presenting with isolated heart block.
- Outcomes research
- Corticosteroids
- Autoantibodies
- Cardiovascular Disease
Statistics from Altmetric.com
Introduction
The signature lesion of anti-SSA/Ro-associated cardiac neonatal lupus (cardiac-NL) is advanced (second or third degree) congenital heart block (CHB). Histologically, CHB is represented by fibrosis, calcification and infiltration of macrophages and giant cells in the atrioventricular (AV) node.1 Injury can extend beyond the AV node and include endocardial fibroelastosis (EFE) and dilated cardiomyopathy (DCM).2 ,3 Cardiac-NL, often identified in utero between 18 and 24 weeks of gestation,4 is associated with significant mortality (17.5%) and morbidity (70% require pacing).5 ,6 The case fatality rate approaches 50% when extranodal disease is present.5 ,6
Reduction of an inflammatory response with fluorinated steroids (FS), given their bioavailability in the fetus,7 is considered a logical approach to prevent or treat cardiac-NL. FS may reverse first and second degree heart block, with the rationale that incomplete block reflects ongoing inflammation preceding AV nodal fibrotic replacement and calcification seen in complete block.5 ,6 ,8–10 Published data are limited and discordant regarding the efficacy of FS in reducing mortality in cardiac-NL.6 ,11 ,12 Thus, insufficient evidence, amplified by maternal and fetal toxicity associated with FS use,9 ,13 ,14 leaves physicians with a therapeutic dilemma regarding whether to initiate treatment in cases with isolated advanced block to prevent progression of disease beyond the AV node and, by extension, mortality.
To date, no published studies have systematically evaluated only those fetuses with detectable injury restricted to the conduction system, to address whether prompt initiation of FS prevents development of extranodal disease. Accordingly, this study leveraged data available from a large registry of NL15 to address the efficacy of FS with regard to progression, mortality and need for pacemaker implantation.
Methods
Study population
Cardiac-NL cases were identified from the Research Registry for Neonatal Lupus (RRNL), established in 1994.15 Evaluation of de-identified information was approved by the NYU School of Medicine IRB. Enrolment of a family in the RRNL requires verification of maternal anti-SSA/Ro antibodies by a CLIA-approved laboratory or the research laboratory of JPB, and documentation that at least one child has NL. The affected children were born between 1972 and 2013.
Inclusion/exclusion criteria
As of 31 January 2015, 394 cases of cardiac-NL were enrolled in the RRNL, with 156 children meeting the following inclusion criteria for the primary analysis: (a) advanced (second or third degree) heart block in utero documented by echocardiogram and (b) no evidence of extranodal disease (defined as EFE, DCM and/or hydrops) at the time of advanced block detection. These cases will herein be referred to as isolated block. Exclusion criteria are itemised in figure 1 and in the online supplementary text.

Flow diagram of assessment, inclusion, exclusion and analysis of study subjects. FS, fluorinated steroids; NL, neonatal lupus; RRNL, Research Registry for Neonatal Lupus.
Study design, outcome measures and data collection
This was a retrospective study. Extranodal disease was defined as one or more of the following noted on any fetal or postnatal echocardiograms: (1) diagnosis of EFE, (2) DCM and (3) hydrops fetalis as previously defined.5 Dates of death of affected children and data on pacemaker implantation and time of initial placement were recorded. The cumulative dose of FS to which the fetus was exposed in utero was calculated. Maternal, fetal and echocardiographic factors analysed (including medications) are listed in table 1.
Clinical and demographic characteristics
Statistical methods/analysis
Survival distributions were estimated by the Kaplan–Meier method. For mortality, weeks since conception was used as the timescale to include deaths that occurred in utero (N=7) as well as after a live birth. Unadjusted and adjusted HRs for death, extranodal disease and pacemaker implantation associated with FS were estimated from Cox proportional hazards regression models. Covariates that were statistically significant and/or were deemed a priori to be clinically important were included in the regression model. For analysis of extranodal disease and pacemaker implantation, death was considered a competing risk.16 In analysing pacemaker implantation, weeks since birth was the timescale, and only live births were included. Five fetuses, four of which died, were not exposed to FS at detection of advanced block and subsequently developed disease beyond the AV node, at which time they were given FS. These five cases were included only in the extranodal disease analysis and were considered as unexposed to FS (for a survival analysis that includes these five cases, see online supplementary text). All analyses were performed in SAS (V.9.4). Two-sided p<0.05 were considered statistically significant.
Results
Patient demographics, maternal autoantibody status and medication use
Table 1 presents patient characteristics stratified by exposure to FS within a week of detection compared with no exposure. There were no differences between treatment groups with regard to most variables except that fetuses exposed to FS were significantly more likely to be born more recently.
The initial steroid dose was equivalent to ≥4 mg/day dexamethasone in 97% of cases (range: 2–8 mg/day), with 82% receiving the equivalent of 4 mg dexamethasone. The average daily dose was 2.8±1.8 mg. Steroids were initiated an average of 1.8 days after detection of block. The average cumulative dose of FS to which fetuses were exposed was the equivalent of 274±177 mg of dexamethasone. Overall, there was no significant difference between treatment groups in use of other medications, with the exception that hydroxychloroquine use (although limited) was significantly higher in mothers treated with FS (p=0.006).
Evaluation of FS use for prevention of extranodal disease
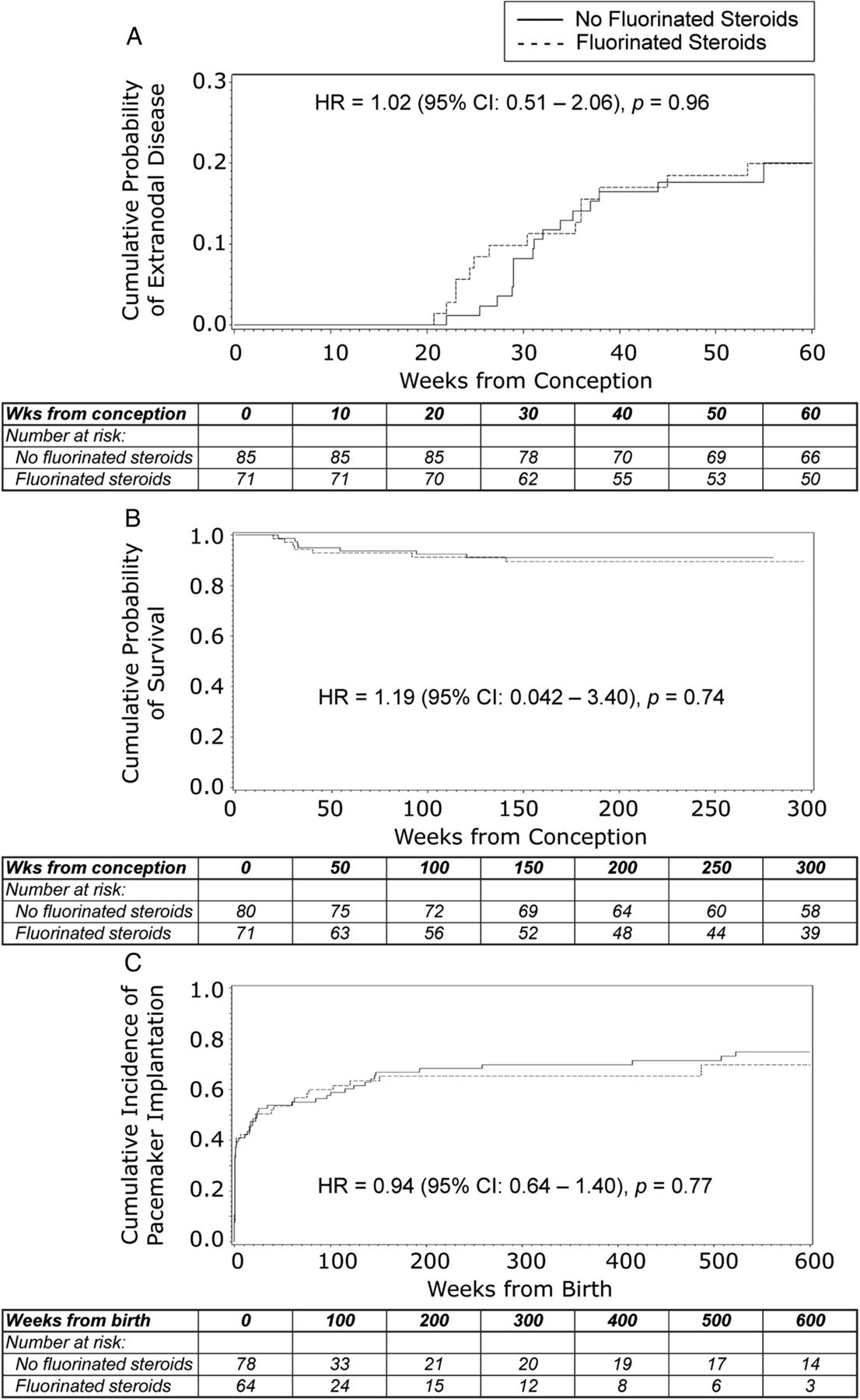
FS did not reduce the risk of development of extranodal disease when given within 1 week of detection of advanced block (figure 2A). Overall, 14 (19.7%) of 71 fetuses exposed to FS developed extranodal disease, compared with 17 (20.0%) of 85 unexposed, yielding an unadjusted HR of 1.02 (95% CI 0.51 to 2.06; p=0.96).
{kind=link}
{kind=link}
Kaplan–Meier curves reflecting the probability of: (A) Developing disease beyond the atrioventricular (AV) node in cases that presented with isolated advanced block. Solid line=no fluorinated steroid treatment (N=85); dashed line=fluorinated steroid treatment (N=71). The X axis represents weeks from conception. (B) Survival for cases presenting with isolated advanced block. Solid line=no fluorinated steroid treatment (N=80); dashed line=fluorinated steroid treatment (N=71). The X axis represents weeks from conception. Of note, the five cases who received fluorinated steroids at the time of diagnosis of extranodal disease were excluded from this analysis. (C) Pacemaker implantation. Solid line=no fluorinated steroid treatment (N=78); dashed line=fluorinated steroid treatment (N=64). The X axis represents weeks from birth. Of note, the five cases who received fluorinated steroids at the time of diagnosis of extranodal disease were excluded from this analysis. Additional four cases that died in utero and five cases in which pacing data were either unavailable (N=2) or the exact timing of pacemaker implantation was unknown (N=3) were also removed.
A multivariable Cox analysis, adjusted for potential confounders, yielded an adjusted HR=0.90 (95% CI 0.43 to 1.85; p=0.77) for development of extranodal disease associated with FS treatment at diagnosis of isolated block. No identifiable risk factors were noted (see online supplementary table S1).
Evaluation of FS use for prevention of mortality
FS did not improve overall survival when given at detection of isolated block (figure 2B). Overall, 7 (9.9%) of 71 FS-exposed fetuses died, compared with 7 (8.8%) of 80 unexposed: HR=1.19 (95% CI 0.42 to 3.40; p=0.74). (As noted in Methods, five cases that did not receive FS until diagnosis of extranodal disease were excluded from this analysis; for an analysis including these five cases as ‘unexposed’, see online supplementary text.) In cases exposed to FS, the average time between steroid initiation and death was 31.7 weeks. There were seven in utero deaths: three in the exposed and four in the unexposed group. In fetuses exposed to FS, cumulative dose did not influence mortality (mean 227.3±190.8 mg in those who died vs 278.4±176.2 mg in survivors; p=0.50).
The adjusted HR for mortality associated with FS treatment at diagnosis of isolated block was 1.63 (95% CI 0.43 to 6.14; p=0.47). Development of disease beyond the AV node was strongly associated with mortality (HR=10.85; 95% CI 3.48 to 33.84; p<0.0001) (see online supplementary table S1).
Evaluation of FS use for prevention of pacemaker implantation
FS given at diagnosis of isolated block did not prevent the need for pacemaker implantation (figure 2C). Overall, 42 (66%) of 64 live births exposed to FS were paced compared with 60 (75%) of 78 unexposed, yielding an unadjusted HR=0.94 (95% CI 0.64 to 1.40; p=0.77). The HR adjusted for potential confounders for pacemaker implantation associated with FS treatment at diagnosis of isolated block was 0.87 (95% CI 0.57 to 1.33; p=0.53) (see online supplementary table S1 for additional results).
Discussion
Despite acceptance that complete block is irreversible, prevention of more extensive injury has been considered because extranodal disease is a marker of poor outcome.5 ,6 To our knowledge, this is the first study to evaluate whether early institution of maternal FS for fetuses with isolated advanced heart block prevents progression of injury, death or requirement for pacemaker implantation. These data do not provide evidence that prompt FS use significantly alters fetal/neonatal morbidity or mortality. Variables that differed between treated and untreated groups included year of birth, which did not associate with extranodal disease, and hydroxychloroquine use, which was so infrequent that it precluded meaningful analysis. Multivariable analyses revealed no identifiable maternal or fetal risk factor for progression of disease beyond the AV node. Extranodal disease was significantly associated with mortality, consistent with previous reports.5 ,6 ,17 ,18
The average FS dose used in this study was lower than in the single reported study that demonstrated a benefit from treatment.11 Maternal steroid dosing is challenging since the desired effect is in the fetus. It has been reported that between 50% and 98% of FS cross the placenta.19 Using a conservative estimate of transplacental passage, fetuses were exposed to at least 1.4 mg of dexamethasone, greater than the standard mg/kg equivalent of prednisone used to treat children with myocarditis.20
Earlier studies have evaluated use of maternal FS with discordant results (for more details, see online supplementary text).6 ,8 ,10–12 However, in these studies, prevention of extranodal disease was not the stated intent.
The need for robust data regarding efficacy of FS in prevention of disease progression is further compounded by the risk of toxicity.9 Maternal and fetal side effects of FS were not systematically collected in our study. Additional study limitations are presented in the online supplementary text.
In summary, the use of FS at detection of isolated block did not prevent development of extranodal disease, improve survival or prevent pacemaker implantation.
Acknowledgments
The authors would like to acknowledge Ann Rupel and Amanda Zink for assistance in preparing the manuscript, and the families who have enrolled in the Research Registry for Neonatal Lupus whose information made this study possible.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online table
Footnotes
Handling editor Tore K Kvien
Contributors PMI, AS, MYK and JPB have full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All the authors were involved in preparing this manuscript. PMI, AS, MYK and JPB were responsible for the overall study design, data analysis and interpretation of data, and wrote the initial draft of the manuscript. All the authors contributed to the critical revision of the manuscript.
Funding This work was supported by American Heart Association Founders Affiliate Clinical Research Program Award #11CRP795008 and the S.L.E. Lupus Foundation MD Scientist Fellowship Grant to AS; and by National Institute of Arthritis and Musculoskeletal and Skin Disease (NIAMS) contract N01-AR-4-2220-11-0-1 and grant 5R37AR042455, Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) grants R01 HD079951-01A1 and R03 HD069986, and a Lupus Foundation of America LFA Lifeline Program grant to JPB.
Competing interests None declared.
Ethics approval This study was approved by the Institutional Review Board of New York University School of Medicine (IRB Protocol Title: Research Registry for Neonatal Lupus (RRNL), IRB Protocol Number: 7820).
Provenance and peer review Not commissioned; externally peer reviewed.