Article Text

Abstract
Background Previous studies have suggested a potential risk of cervical cancer in patients with systemic inflammatory diseases (SID) such as inflammatory bowel disease (IBD) and systemic lupus erythematosus (SLE).
Objectives To assess the risk of high-grade cervical dysplasia, a surrogate endpoint for cervical cancer and cervical cancer, in women with SID, including IBD, psoriasis, rheumatoid arthritis (RA) or SLE, compared with the risk in women without SID.
Methods Using US insurance data (2001–2012), we conducted a cohort study of 133 333 women with SID, based on two or more diagnoses and one or more dispensed prescription for disease-specific treatment, and 533 332 women without SID. High-grade cervical dysplasia and cervical cancer was defined by a validated algorithm with a positive predictive value of ≥81%.
Results Over the mean follow-up of 2.1 years, the crude incidence rate of high-grade cervical dysplasia and cervical cancer per 100 000 person-years was the highest at 141.1 in SLE and the lowest at 82.2 in psoriasis among women with SID, and 73.4 in women without SID. The multivariable HR adjusted for potential confounders was 1.07 (95% CI 0.79 to 1.45) in IBD, 0.96 (95% CI 0.73 to 1.27) in psoriasis, 1.49 (95% CI 1.11 to 2.00) in RA and 1.53 (95% CI 1.07 to 2.19) in SLE. Multivariable HRs were increased, but not statistically significant, in IBD, RA and SLE with baseline use of systemic immunosuppressive drugs or steroids.
Conclusions The risk of high-grade cervical dysplasia and cervical cancer was 1.5 times higher in women with RA and SLE than in those without SID. The risk may be increased in IBD with use of systemic immunosuppressive drugs or steroids.
- Autoimmune Diseases
- Rheumatoid Arthritis
- Systemic Lupus Erythematosus
- Epidemiology
Statistics from Altmetric.com
Introduction
Human papillomavirus (HPV) infection is the most common sexually transmitted disease in the USA.1 Although most low-grade cervical intraepithelial neoplasia (CIN) lesions regress spontaneously, the majority of high-grade cervical dysplasia, CIN 2 or 3 do not.1 Persistent HPV infection, the major risk factor for cervical cancer, is related to other factors, such as older age, HPV genotype, coexisting infections, immunosuppression and inflammation.1 ,2
Some studies have suggested an increased risk of cervical dysplasia and HPV infection in immunocompromised patients including those with systemic inflammatory disease (SID), such as inflammatory bowel disease (IBD), rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE).3–8 Although the progression of HPV infection to cervical cancer in immunocompromised women is not yet fully understood, viral reactivation from a latent state in immunocompromised patients has been noted.9 ,10 Impaired innate and cellular immune responses in patients with SID, particularly those taking immunosuppressive drugs, may decrease clearance of HPV infection or regression of CIN and may result in persistent HPV infection and an increased risk of high-grade cervical dysplasia and cervical cancer.11 ,12
The US Preventive Services Task Force recommends screening for cervical cancer in women aged 21–65 years with Papanicolaou (Pap) smear every 3 years or, for women aged 30–65 years who want to lengthen the screening interval, screening with a combination of Pap smear and HPV testing every 5 years.13 With such a routine Pap test, cervical cancer is rare, with an estimated annual incidence rate (IR) of 7.9/100 000 people in the USA, as most women are diagnosed with cervical dysplasia and treated before they develop invasive cervical cancer.14 High-grade cervical dysplasia, including CIN 2, CIN 3 and carcinoma in situ, has been used as a surrogate endpoint in cervical cancer prevention trials in order to decrease sample size and follow-up duration.15 ,16
The objectives of this study were (1) to assess the risk of high-grade cervical dysplasia and cervical cancer in women with SID, including IBD, psoriasis, RA and SLE, compared with the risk for those without SID and (2) to examine the risk of high-grade cervical dysplasia and cervical cancer specific to each SID compared with the risk for those without SID.
Methods
Data source
We conducted a cohort study using the claims data from two commercial US health plans, the Wellpoint (2001–2008) and the United Healthcare (2003–2012), which primarily insure working adults and their family members. These databases provide a large, population-based cohort and contain longitudinal claims information, including medical diagnoses, procedures, hospitalisations, doctor visits and pharmacy dispensing on subscribers with medical and pharmacy coverage across the USA. The quality of data on inpatient diagnoses, procedures, healthcare use and drug dispensing as well as some outpatient diagnoses is known to be high.17 Both databases have been successfully used in a number of high-quality published studies.18–22 Because the study databases were deidentified, patient informed consent was not required. The study protocol was approved by the institutional review board of Brigham and Women's Hospital.
Study cohort
Among female patients aged ≥18 years, we selected women with SID, including RA, SLE, psoriasis and IBD based on a combination of two or more International Classification of Diseases, ninth revision (ICD-9) codes on two separate visits that were ≥7 days apart. The start of the follow-up period (ie, index date) was defined as the date of the first disease-specific drug dispensing (see online supplementary table S1) after ≥12 months of continuous health plan eligibility; thus, all people in the ‘SID cohort’ were required to have had two diagnoses of RA, SLE, psoriasis (including psoriatic arthritis) or IBD and one or more filled prescription for disease-specific treatment at the start of follow-up. Nursing home residents, women with hysterectomy organ transplantation, HIV infection and malignancy in the 12-month period before the index date were excluded. In addition, women with diagnosis of more than one SID were excluded; the SID subcohorts, RA, SLE, psoriasis and IBD, were thus mutually exclusive.
For comparison with the SID cohort, we identified the non-SID cohort among female patients aged ≥18 years who did not have a RA, SLE, psoriasis or IBD diagnosis during the study period. To compare the risk of high-grade cervical dysplasia and cervical cancer in women with SID with people with another chronic medical condition requiring regular visits to a doctor, we identified patients who had two or more ICD-9 codes for hypertension on two separate visits ≥7 days apart described herein as the ‘non-SID cohort’. The index date for the non-SID cohort was defined as the date of the first dispensation of an antihypertensive drug after ≥12 months of continuous health plan eligibility. Requirement of the same number of visits and the use of prescription as in the SID cohort was chosen to minimise surveillance bias. The aforementioned exclusion criteria were then applied to the non-SID cohort. Patients in the non-SID cohort were then matched with patients with SID for age and index date (±30 days) with a 4:1 ratio.
Patients were then followed up until the first of any of the following censoring events: development of the outcome, disenrolment, end of the study database (ie, 2008 for the Wellpoint and 2012 for the United databases) or death.
Outcome definition
The primary outcome of interest was high-grade cervical dysplasia or cervical cancer. To identify the primary outcome, we developed a claims-based algorithm that combined two ICD-9 and current procedural terminology codes for relevant gynaecological procedures or treatment within 30 days after the diagnosis date (see online supplementary table S2) using the billing data in an electronic medical records database.23 The positive predictive value of the algorithm was 91% in the electronic medical records database and 81% in an independent insurance claims database using cytological or pathological diagnosis of CIN 2 or worse as the ‘gold standard’.23 In addition, we assessed the number of visits to gynaecology doctors and number of gynaecological procedures during the follow-up.
Covariates
A number of predefined variables potentially associated with risk of HPV infection or cervical cancer were assessed using data from the 12-month baseline period before the index date. These variables included age, risk factors for HPV infection, comorbidities, medication such as systemic immunosuppressive drugs and steroids and healthcare use factors (see table 1). Systemic immunosuppressive drugs included azathioprine, cyclophosphamide, ciclosporin, hydroxyurea, leflunomide, methotrexate, 6-mercaptopurine, mycophenolate, pimecrolimus, tacrolimus, abatacept, adalimumab, alefacept, anakinra, certolizumab pegol, etanercept, golimumab, infliximab, rituximab, tocilizumab and ustekinumab. In addition, women who were likely to be sexually active were identified based on a previously validated claims-based algorithm.24 To quantify patients’ comorbidities at baseline, we also calculated a comorbidity score that combined 20 medical conditions included in both the Charlson Index and the Elixhauser system based on ICD-9.25
Baseline characteristics of the study cohort in 12 months before the index date
Statistical analyses
We compared the baseline characteristics of the SID and non-SID cohorts as well as the SID subcohorts. IRs of high-grade cervical dysplasia and cervical cancer with 95% CI were calculated for each cohort and SID subcohort. Unadjusted and multivariable Cox proportional hazard models adjusting for various potential confounders listed in table 1 were used to compare the risk of high-grade cervical dysplasia and cervical cancer in the SID cohort with that in the non-SID cohort.26 In separate unadjusted and multivariable Cox models, the risk of high-grade cervical dysplasia and cervical cancer in each SID subcohort was assessed compared with the non-SID cohort. The likelihood ratio test was performed to examine heterogeneity between the SID subcohorts. Kaplan–Meier curves were plotted for the cumulative incidence of high-grade cervical dysplasia and cervical cancer in the SID subcohorts and non-SID cohort.
Multivariable Cox regression models stratified by receipt of baseline Pap smear or HPV testing and prior abnormal Pap smears were performed for comparison of the SID and non-SID cohorts. We estimated the proportion of women who had one or more visit to a gynaecologist or one gynaecological testing done during the follow-up period in each cohort to deal with surveillance bias, as high-grade cervical dysplasia or early cervical cancer would probably be asymptomatic and thus diagnosed mainly with a screening test. Among a subgroup of women with one or more visit to a gynaecologist or one gynaecological testing (ie, Pap smear, colposcopy or HPV-DNA test) done during the follow-up period, the risk of high-grade cervical dysplasia and cervical cancer was compared between the SID and non-SID cohorts. Furthermore, we conducted another subgroup analysis in patients with SID with and without systemic immunosuppressive drugs or steroids at baseline compared with patients without SID. All these subgroup analyses were repeated for the comparison between the SID subcohorts and the non-SID cohort.
We determined the potential impact of unmeasured confounders on the association between SID and high-grade cervical dysplasia and cervical cancer in a sensitivity analysis.27 Proportional hazard assumptions for the SID cohort and each disease-specific subcohort were not violated, assessed by the Kolmogorov supremum test.28 All analyses were done using SAS V.9.2 statistical software (SAS Institute Inc, Cary, North Carolina, USA).
Results
Study cohort
The study included 133 333 patients with SID, including 25 176 patients with IBD, 34 665 with psoriasis, 58 979 with RA, 14 513 with SLE and 533 332 patients without SID. The mean (SD) follow-up time was 2.1 (1.8) years for both patients with SID and without SID. Table 1 shows baseline characteristics of the age- and index date-matched cohorts and SID subcohorts. Little differences across most HPV-infection associated factors and preventive medical services existed between the cohorts. The mean (SD) number of total doctor visits was 9.6 (7.0) in the SID cohort and 6.7 (5.2) in the non-SID cohort. However, the mean (SD) number of visits to a gynaecologist was similar—0.8 (1.9) in the SID cohort and 0.8 (2.3) in the non-SID cohort. Women who were identified as being sexually active or were using prescription drugs including systemic immunosuppressive drugs and steroids and comorbidities except diabetes were more common in the SID than the non-SID cohort. The proportion of patients with a sigmoidoscopy or colonoscopy at baseline was higher in the SID cohort owing to the IBD subcohort.
Risk of high-grade cervical dysplasia and cervical cancer
The IR of high-grade cervical dysplasia and cervical cancer was 94.2 per 100 000 person-years in the SID and 73.4 per 100 000 person-years in the non-SID cohort (table 2). Table 3 summarises the results from various multivariable Cox regression analyses comparing the SID cohort with the non-SID cohort. The HR adjusted for age, HPV infection-associated factors, comorbidities and the number of prescription drugs was 1.23 (95% CI 1.04 to 1.46) in the SID cohort. In the fully adjusted model, the HR in the SID cohort became 1.16 (95% CI 0.97 to 1.39). The likelihood ratio test of the global null hypothesis showed no significant heterogeneity between the SID subcohorts (χ2=6.04, df=3, p=0.11).
Incidence rates (IRs) per 100 000 person-years and IR ratios of high-grade cervical dysplasia and cervical cancer*
HRs (95% CIs) for high-grade cervical dysplasia and cervical cancer
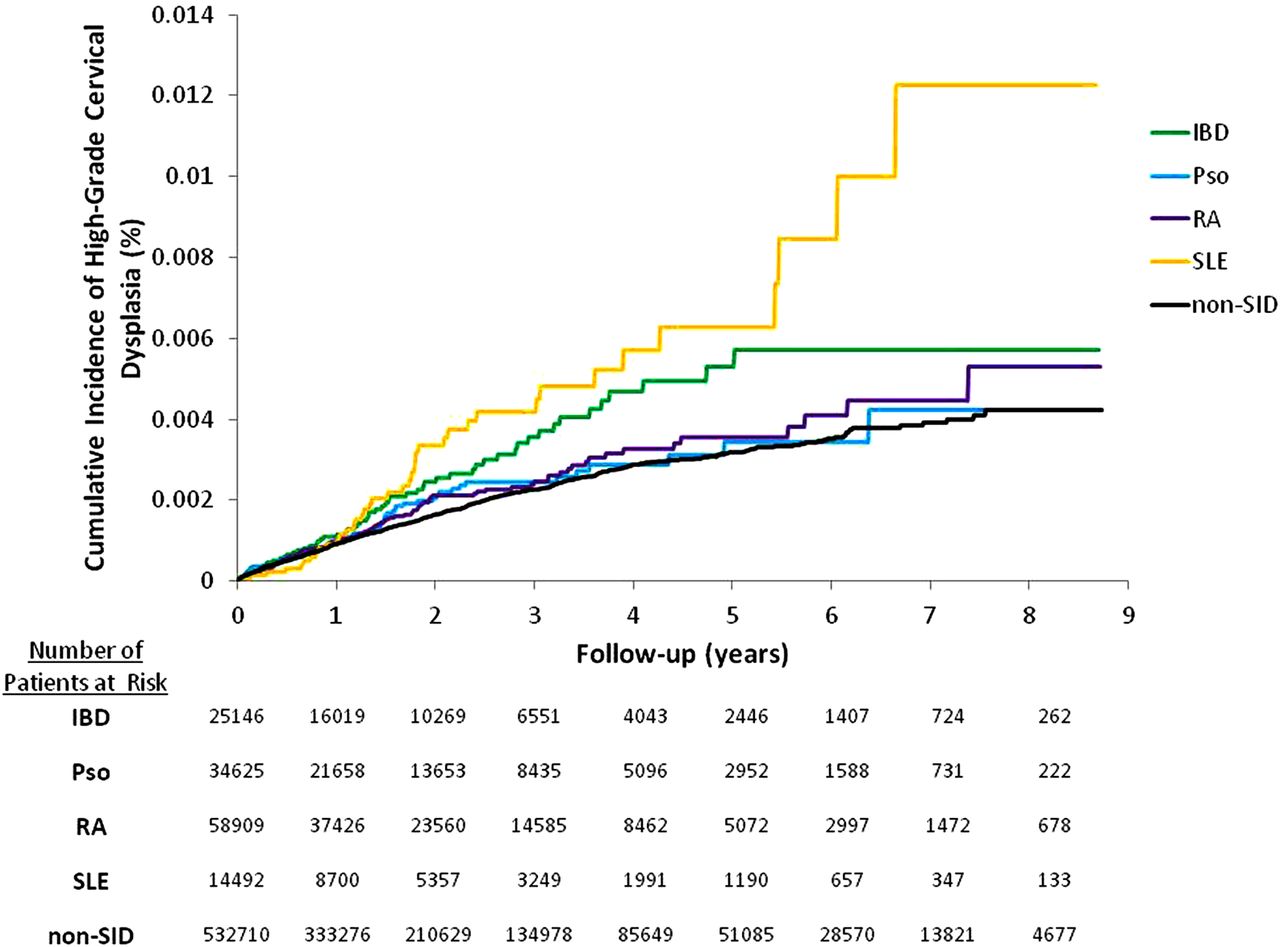
Among the four SID subcohorts, the IR of high-grade cervical dysplasia and cervical cancer was the highest in women with SLE and the lowest in women with psoriasis (table 2). Kaplan–Meier curves comparing the cumulative incidence of high-grade cervical dysplasia and cervical cancer in the SID subcohorts and non-SID cohort showed an increased risk in the IBD, RA and SLE subcohorts (figure 1). Unadjusted HRs for high-grade cervical dysplasia and cervical cancer were raised across all four subcohorts, with the highest HR of 1.90 in SLE and the lowest HR of 1.11 in psoriasis (table 3). With full adjustment, the HR was not increased in the IBD (1.07, 95% CI 0.79 to 1.45) and psoriasis (0.96, 95% CI 0.73 to 1.27) subcohorts. For the SLE subcohort, the HR was attenuated but remained raised at 1.53 (95% CI 1.07 to 2.19) in the fully adjusted model. In the RA subcohort, further adjustment for potential confounders moved the HR away from the null with a fully adjusted HR of 1.49 (95% CI 1.11 to 2.00).

{kind=link}
Kaplan–Meier curves for the cumulative incidence of high-grade cervical dysplasia and cervical cancer. IBD, inflammatory bowel disease; Pso, psoriasis; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; SID, systemic inflammatory disease.
Stratified and subgroup analyses
In women with one or more baseline Pap smear or HPV-DNA testing done, the fully adjusted HR was 1.73 (95% CI 1.18 to 2.59) in RA and 1.60 (95% CI 0.98 to 2.59) in SLE compared with women without SID (table 4). Among the women without prior history of abnormal Pap smear, the fully adjusted HR was 1.13 (95% CI 0.78 to 1.63) for IBD, 0.87 (95% CI 0.62 to 1.23) for psoriasis, 1.31 (95% CI 0.92 to 1.87) for RA and 1.71 (95% CI 1.14 to 2.56) for SLE compared with women without SID.
Stratified and subgroup analyses: fully adjusted* HRs for high-grade cervical dysplasia and cervical cancer in patients with SID compared with those without SID
Among the women with baseline use of systemic immunosuppressive drugs, the fully adjusted HR was increased, but not statistically significant, in IBD (1.72, 95% CI 0.66 to 4.45), RA (1.40, 95% CI 0.65 to 3.03) and SLE (1.52, 95% CI 0.64 to 3.61) compared with women without SID. Similarly, the fully adjusted HR was increased, albeit not statistically significant, in women with IBD, RA and SLE who used systemic steroids at baseline compared with women without SID.
During the mean 2.1 years of follow-up, 53% of women with SID and 50% of women without SID had one or more visit to a gynaecologist or one or more gynaecological testing done. Among the SID subcohorts, 59% of women with IBD, 55% with psoriasis, 49% with RA and 54% with SLE had one or more visits to a gynaecologist or one or more gynaecological tests. The mean (SD) number of visits to a gynaecologist during the follow-up was 3.1 (4.8) in the SID cohort and 3.0 (4.8) in the non-SID cohort. The mean (SD) number of gynaecological tests was also similar between the cohorts, 2.1 (2.1) in the SID and 2.1 (2.0) in the non-SID. Among those women with one or more visit to a gynaecologist or one gynaecological testing, the HRs were consistently raised in RA (1.53, 95% CI 1.13 to 2.06) and SLE (1.52, 95% CI 1.06 to 2.18).
Sensitivity analysis
Online supplementary figure S1 illustrates the potential impact of residual confounding on our results assessed by the rule-out approach.28 Unless very strong risk factors of cervical cancer that are imbalanced between the two groups are unmeasured and uncontrolled in our fully adjusted models, the increased HR associated with RA and SLE cannot be explained by residual confounding.
Discussion
This study found that the incidence of high-grade cervical dysplasia and cervical cancer was very low. It is still important to note that the diagnosis of high-grade cervical dysplasia and cervical cancer is associated with substantial psychosocial burden and high healthcare use for diagnostic and therapeutic procedures.29 ,30 Women with RA and SLE appeared to have a 1.5 times greater risk of high-grade cervical dysplasia and cervical cancer than women without SID after adjusting for many potential confounders. No significantly increased risks were noted in women with psoriasis or IBD. These findings might be related to the difference in the severity of systemic inflammation or in the use of systemic immunosuppressive drugs or steroids across the four subcohorts as most patients with RA and SLE, but only 20% of patients with psoriasis and 13% of those with IBD, were receiving systemic immunosuppressive drugs at baseline. Although a few studies reported an increased risk of abnormal Pap smears in patients with IBD,3 ,4 others found no increased risk of CIN or cervical cancer in this disease.31–33 Our study also found that, among women with baseline use of systemic immunosuppressive drugs or steroids, IBD, RA and SLE may be associated with an increased risk of cervical cancer.
In our multivariable analyses, the HRs were attenuated in IBD, psoriasis and SLE, while the HRs for RA increased with more adjustment. Age appeared to be a major confounder of the association between RA and high-grade cervical dysplasia and cervical cancer; adjusting only for age moved the HR from 1.13 to 1.40. Among all the subcohorts, the mean age of patients was highest in RA. As high-grade cervical dysplasia and cervical cancer is more common in younger women, the absolute risk might not be high in women with RA, but the adjusted risk relative to women without SID was increased.
Several strengths of this study are worth noting. First, we examined a large cohort of patients with SID, including those with IBD, psoriasis, RA and SLE, and a cohort without SID in a population that is representative of the US commercially insured population. Studying relatively uncommon exposures and outcomes is methodologically challenging. With the large size of our study cohort, we were able to observe a total of 1077 women with high-grade cervical dysplasia and cervical cancer. Second, we provided the overall and disease-specific relative risk of high-grade cervical dysplasia and cervical cancer in women with SID, adjusted for age, known HPV infection-associated factors, comorbidities, medication and healthcare use, including preventive medical services. Third, to minimise surveillance bias, we selected the non-SID cohorts as a group of patients with hypertension, a chronic medical condition requiring regular medical care. Women both with and without SID had overall similar general healthcare use and preventive medical services at baseline and during the follow-up. Fourth, we mainly relied on diagnosis and procedure codes for exposure and outcome ascertainment, which can potentially lead to exposure and outcome misclassification. To maximise the specificity, we used a combination of diagnosis codes and a dispensed prescription for a disease-specific treatment to select women with SID and identified high-grade cervical dysplasia and cervical cancer with a previously validated claims-based algorithm combining two diagnoses and a procedure.23 ,34–37
There are limitations to this study. First, this cohort study might still be subject to residual confounding by race, ethnicity, socioeconomic status, behavioral characteristics and gynaecological history of the patients. As sexual activity is a known risk factor for HPV infection and cervical dysplasia, we used a previously validated claims-based algorithm to identify women who were more likely to be sexually active.24 We found that women with SID were more likely to be sexually active than those without SID. The validity of this algorithm in the SID population may require further testing since previous studies have shown a higher proportion of sexual dysfunction in women with SID.38–41 However, as illustrated in the sensitivity analysis (see online supplementary figure S1), the positive association between RA or SLE and high-grade cervical dysplasia or cervical cancer is unlikely to be fully explained by an unmeasured or incompletely measured confounder. Second, this study cannot ascertain whether the increased risk noted in RA and SLE is due to the disease itself or to the treatment. Future studies, however, should examine this question. Third, this study was not designed to determine the comparative safety of different immunosuppressive drugs on the risk of high-grade cervical dysplasia or cervical cancer. Fourth, our results may not be generalisable to women with lower socioeconomic status, as the study databases primarily include working adults and their family members. Fifth, it is possible that the 12-month baseline period was not long enough to capture all the information on potential confounders.
To date, there are no specific guidelines examining HPV vaccination or cervical dysplasia management in the SID population. Two different HPV vaccines are available—a bivalent vaccine for types 16 and 18 and a quadrivalent vaccine for types 6, 11, 16 and 18. Although the efficacy of the HPV vaccine in the SID population has not been studied and some other HPV genotypes are not covered by the current HPV vaccines, young women with SID, particularly those with RA or SLE, should be considered as a target population for the HPV vaccine, given its high efficacy for preventing high-grade cervical dysplasia and cervical cancer in the general population15 ,42 and the safety data in patients with SLE.43 ,44
In conclusion, the risk of high-grade cervical dysplasia and cervical cancer was increased in patients with RA and SLE with and without use of systemic immunosuppressive drugs or steroids at baseline. The risk may also be increased among women with IBD who have had baseline use of systemic immunosuppressive drugs or steroids. Future research should examine whether a different implementation strategy for HPV vaccination or cervical dysplasia management is needed in patients with RA or SLE.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Contributors SCK had full access to all the data in the study and takes responsibility for its integrity and the accuracy of the data analysis. She is the guarantor for the study.
Funding This study is funded by the National Institutes of Health (NIH) grant K23 AR059677. SCK is supported by the NIH grant K23 AR059677. SH-D is supported by the AHRQ grant R01HS018533. EWK is supported by NIH AR052403, AR047782 and AR049880. SS is principal investigator of the Harvard-Brigham Drug Safety and Risk Management Research Center funded by FDA. His work is partially funded by grants/contracts from PCORI, FDA and NHLBI. DHS is supported by the NIH grants K24 AR055989, P60 AR047782 and R01 AR056215.
Competing interests SCK receives research support from Pfizer and tuition support for the Pharmacoepidemiology Program at the Harvard School of Public Health partially funded by the Pharmaceutical Research and Manufacturers of America (PhRMA) foundation. RJG receives research support from AstraZeneca and Novartis. Hernandez-Diaz has consulted for GSK Biologics and Novartis for unrelated projects. SS is consultant to WHISCON, LLC and to Aetion, Inc. of which he also owns shares. He is principal investigator of investigator-initiated grants to the Brigham and Women's Hospital from Novartis and Boehringer-Ingelheim unrelated to the topic of this study. DHS receives research support from Amgen, Lilly, Pfizer and CORRONA and serves in unpaid roles on studies sponsored by Pfizer, Novartis, Lilly and Bristol Myers Squibb.
Ethics approval Brigham and Women's Hospital institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.