Article Text

Abstract
Objectives To evaluate the efficacy of rituximab (RTX) in IgG4-related disease (IgG4-RD) in an open-label pilot trial.
Methods We treated 30 IgG4-RD patients with two doses of RTX (1000 mg each). The participants were either treated with RTX alone (n = 26; 87%) or required to discontinue baseline glucocorticoids (GC) within 2 months (n = 4; 13%). Disease activity was measured by the IgG4-RD Responder Index (IgG4-RD RI) and physician's global assessment (PGA). Disease response was defined as the improvement of the IgG4-RD RI by two points. The primary outcome, measured at 6 months, was defined as: (1) decline of the IgG4-RD RI ≥2 points compared with baseline; (2) no disease flares before month 6; and (3) no GC use between months 2 and 6. Complete remission was defined as an IgG4-RD RI score of 0 with no GC use.
Results Disease responses occurred in 97% of participants. The baseline IgG4-RD RI and PGA values, 11±7 and 63±22 mm, respectively, declined to 1±2 and 11±16 mm at 6 months (both p<0.00001). The primary outcome was achieved by 23 participants (77%). Fourteen (47%) were in complete remission at 6 months, and 12 (40%) remained in complete remission at 12 months. Among the 19 with elevated baseline serum IgG4, IgG4 concentrations declined from a mean of 911 mg/dL (range 138–4780 mg/dL) to 422 mg/dL (range 56–2410 mg/dL) at month 6 (p<0.05). However, only 8 (42%) of the 19 achieved normal values.
Conclusions RTX appears to be an effective treatment for IgG4-RD, even without concomitant GC therapy.
Trial registration number ClinicalTrials.gov identifier: NCT01584388.
- B cells
- Inflammation
- Treatment
Statistics from Altmetric.com
Introduction
IgG4-related disease (RD) is a fibroinflammatory disorder with the potential to affect essentially any organ.1–4 The cardinal histopathologic features of IgG4-RD are a lymphoplasmacytic infiltrate, storiform fibrosis, and obliterative phlebitis, often accompanied by tissue eosinophilia.5 The lymphoplasmacytic infiltrate is composed of polyclonal CD20+ lymphocytes, T-cells, and enriched with IgG4+ plasma cells. Many but not all IgG4-RD patients have elevated serum IgG4 concentrations, but this is not a requirement for diagnosis.6
Treatment paradigms for IgG4-RD have been extrapolated primarily from observational studies of glucocorticoids (GCs) in type 1 (IgG4-related) autoimmune pancreatitis (AIP).7–10 The relapse rate both during and after GC tapers in IgG4-RD is high.7 ,11 ,12 A recent review from Japan concluded that most patients with IgG4-RD require between 5 and 10 mg/day of prednisone for remission maintenance.13 Moreover, because IgG4-RD targets middle-aged to elderly individuals and demonstrates a predilection for causing pancreatic damage, GCs are tolerated poorly in a sizeable subset of patients. Indeed, 27% of patients in a recent prospective evaluation of GCs in IgG4-RD experienced either new-onset diabetes or exacerbations of existing diabetes.12 Conventional disease modifying anti-rheumatic drugs (DMARDs) are not useful in inducing remission on their own, but may have benefit in the maintenance of remission after GC-induced remission.10 Thus, no drug other than GC is known to induce remission in IgG4-RD.
Case series suggest that B cell depletion with rituximab (RTX) might be an effective therapy for treating IgG4-RD.14–16 This prospective, open-label clinical trial aimed to evaluate the tolerability and the efficacy of B cell depletion for remission induction in IgG4-RD.
Methods
Study design
The trial (ClinicalTrials.gov identifier NCT01584388) was performed at the Massachusetts General Hospital (Boston, Massachusetts, USA) and Mayo Clinic (Rochester, Minnesota, USA). All patients signed informed consent approved at the sites’ Institutional Review Boards. Thirty participants were treated with two 1000 mg doses of RTX, administered approximately 15 days apart. RTX was provided by Genentech (South San Francisco, California, USA). The primary outcome was assessed at 6 months. Participants were followed for 1 year after RTX treatment.
Inclusion criteria
All participants had active disease as defined by the IgG4-RD Responder Index (IgG4-RD RI).17 Eligible patients also had either: (1) histopathologic diagnoses of IgG4-RD confirmed by international consensus pathology criteria or international consensus AIP criteria5 ,18 or (2) clinical presentation, laboratory features, and computed tomographic findings compatible with type 1 (IgG4-related) AIP.18 Histopathologic diagnoses were established by the presence of a lymphoplasmacytic infiltrate and storiform fibrosis of an involved organ, accompanied by ≥10 IgG4-bearing plasma cells per high-power field or an IgG4/IgG plasma cell ratio of ≥40%.5 Twenty-nine of the 30 patients had the histopathological confirmation of the IgG4-RD diagnosis according to these criteria. One had a clinical presentation consistent with type 1 (IgG4-related) AIP, a substantial serum IgG4 elevation, and computed tomographic findings strongly consistent with the diagnosis of IgG4-RD.18 In all cases, careful clinicopathological and clinicoradiological correlations were performed.
Glucocorticoid use
All participants received methylprednisolone 100 mg intravenously before each RTX dose to reduce the severity of any infusion reactions, but otherwise were treated with RTX alone whenever possible. Participants could be treated with prednisone at baseline if the clinician believed that concomitant GC use might be required to establish disease control, but were required to discontinue that medication within 2 months. Of the four participants treated with GC at enrolment, only one started prednisone simultaneously with RTX. The other three patients had been receiving GC for 5, 13, and 22 months at the time of their trial entry.
Disease activity and damage measures
The IgG4-RD RI
The IgG4-RD RI is a tool designed to measure IgG4-RD activity and damage.17 The IgG4-RD RI was designed specifically for IgG4-RD, on the model of the Birmingham Vasculitis Activity Score for Wegener's granulomatosis (BVAS/WG).19 ,20 The scoring sheet for the IgG4-RD RI is shown in online supplementary figure S1. The IgG4-RD RI requires the investigator to score disease activity and damage in each organ system. Individual organ scores are summed to achieve the cumulative index. Active IgG4-RD must be distinguished from intercurrent or comorbid medical issues. Damage from IgG4-RD and damage associated with treatment IgG4-RD are both distinguished from active IgG4-RD. The IgG4-RD RI includes a column that allows the investigator to record damage incurred in each organ system from active or previously active IgG4-RD.
Disease activity in each organ system is classified into one of four categories in the IgG4-RD RI. The organ system is scored a ‘4’ if the disease activity has worsened despite treatment; a ‘3’ if new or recurrent disease activity is present in that system; a ‘2’ if the disease activity is persistent (unchanged from the previous visit and still active); a ‘1’ if it is improved but still present; and a ‘0’ if the organ system is normal or if the previous disease activity has resolved. The individual organ system score is doubled when the need to initiate treatment for active IgG4-RD in that particular organ is considered urgent (eg, a ‘3’ for new or recurrent disease activity becomes a ‘6’). Urgent disease is defined as IgG4-RD activity within a critical organ that may lead to organ failure or pose a threat to the patient's life if effective therapy is not begun promptly.
The original IgG4-RD RI index (used in this trial) includes serum IgG4 concentration as well as the individual organ system assessments. In scoring serum IgG4 concentrations, a ‘4’ signifies an increase in the serum concentration despite treatment; a ‘3’ corresponds to new or recurrent serum IgG4 elevations; and so forth. ‘0’ is scored for patients with normal serum IgG4 concentrations. In post hoc analyses, we assessed IgG4-RD-RI scores both with and without the inclusion of serum.
IgG4 concentrations because of growing awareness that the serum IgG4 concentration has shortcomings as a disease biomarker.6 ,21–23
The physician global assessment of disease activity
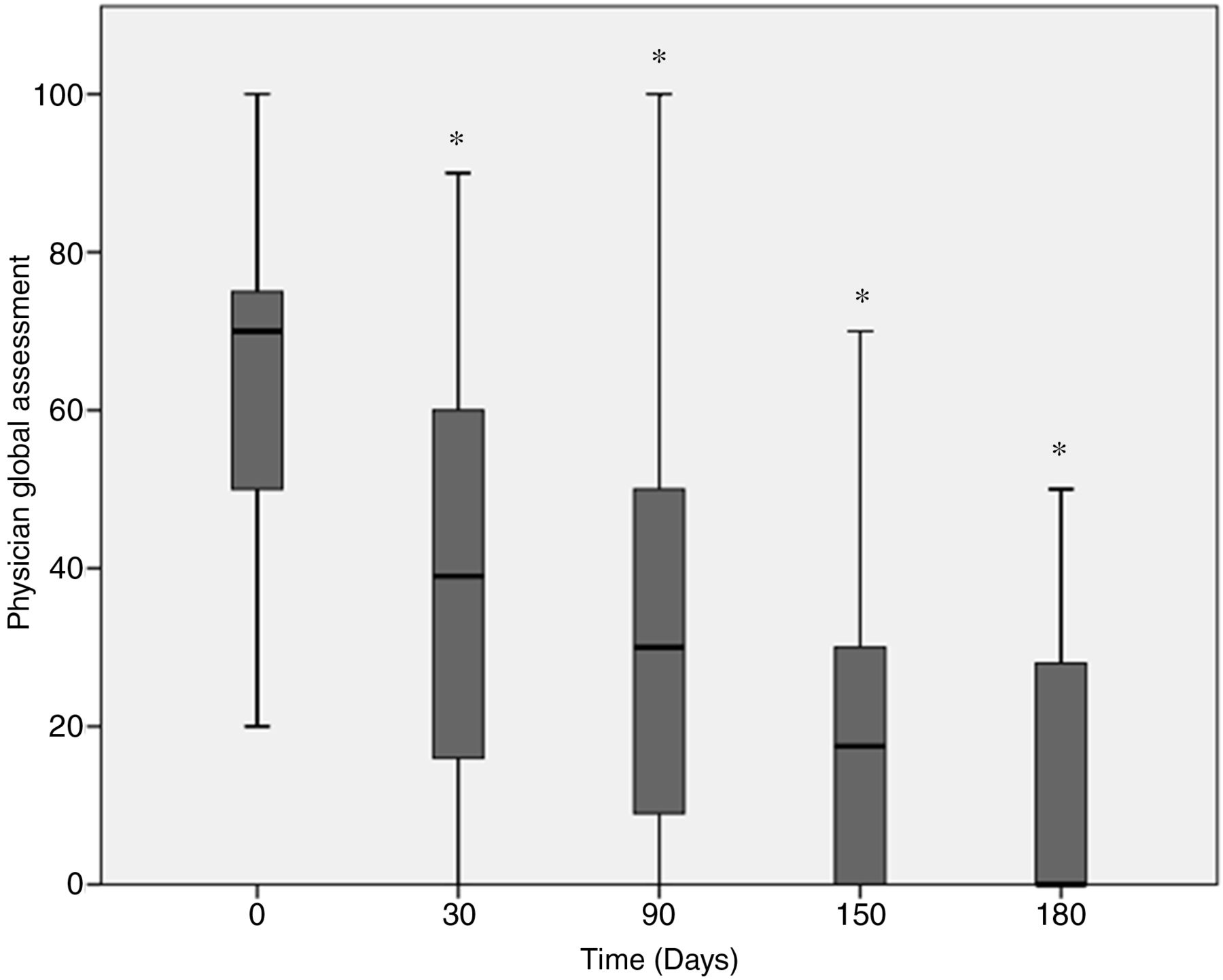
The physician's global assessment (PGA) is a validated visual analogue scale that is scored by placing a vertical mark along a 100 mm horizontal line. The placement of the vertical mark represents the investigator's assessment of the degree of IgG4-RD activity, distinguished from both disease- and treatment-related damage and from comorbid conditions. Zero millimetre indicates no disease activity, that is, remission. A mark of 100 mm indicates the most active disease possible.
Outcome assessments
The primary outcome was defined by three criteria: (1) decline of the IgG4-RD RI ≥2 points compared with baseline; (2) no disease flares before month 6; and (3) no GC use between months 2 and 6. Disease response was defined as an improvement of the IgG4-RD RI ≥2 compared with baseline. Sustained disease response was defined as an improvement of the IgG4-RD RI score ≥2 for 6 consecutive months. Remission was defined as the achievement of an IgG4-RD RI of 0, regardless of GC dose. Complete remission was an IgG4-RD RI of 0 and a prednisone dose of 0. Relapses were defined as increases in the IgG4-RD RI ≥2 and/or the need for the reinstitution of treatment. All adverse events were graded according to the National Cancer Institute's Common Terminology Criteria.24
Clinical assessments
Scheduled trial visits occurred at enrolment, the two RTX infusion visits, and then at months 1, 3, 5, 6, 8, 10, and 12 after the first infusion. Baseline laboratory evaluations included a complete blood count, comprehensive metabolic panel, urinalysis, amylase, lipase, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), C3, C4, serum protein electrophoresis, serum-free light chains, and IgG subclasses. Detailed studies by flow cytometry of peripheral lymphocyte subsets were performed on the MGH patients and will be reported separately. Radiographic data were collected at baseline and at or before month 6 as clinically appropriate.
Statistical analysis
The sample size of 30 participants was determined by enrolment feasibility and the goal of achieving knowledge that was as robust as possible about the utility of B cell depletion in IgG4-RD. The IgG4-RD RI, PGA, and serum IgG4 concentrations were compared with baseline values at subsequent visits using paired t-tests. Contingency data comparing single and multiorgan involvement were analysed by Fisher's exact test.
Results
Patients
Between May 2012 and July 2013, 30 participants were enrolled. Baseline characteristics are presented in table 1. Eighty-seven per cent of the participants enrolled were male and the mean age was 61 years (±11 years). The mean disease duration at the time of enrolment was nearly 6 years (70 months; range 1–540 months).
Baseline characteristics of IgG4-RD subjects (n=30)
Baseline organ involvement
IgG4-RD involved a total of 14 organ sites among the participants and was associated with at least 38 different disease manifestations. As an example, the involvement of the eyes and orbital region (eight participants) included lacrimal gland disease, orbital pseudotumor, orbital myositis, and other (scleritis, amaurosis fugax).
Previous treatment for IgG4-RD
None of the participants were treated with a DMARD at baseline, and only four (13%) were on prednisone. Twenty-two (73%) of the participants enrolled, however, had undergone previous GC courses with subsequent relapse. In addition, many participants had previously received steroid-sparing agents such as mycophenolate mofetil (n=3), azathioprine (n=3), methotrexate (n=1), and RTX (n=6) (see online supplementary table S1), which had failed to prevent relapse and were discontinued before enrolment. No participant had received RTX within 6 months of enrolment, and all had normal B-cell concentrations at enrolment.
Efficacy assessment
Twenty-six participants (87%) were treated initially with RTX alone. Disease responses occurred in 97% at month 6 and were generally observed quickly, often within 2 weeks of the first infusion. One patient whose clinical course was marked by diffuse lymphadenopathy and an extremely high serum IgG4 (1090 mg/dL; normal <121 mg/dL) had recovered normal B cell concentrations by month 3 and did not maintain his response. Twenty-three participants (77%) achieved the primary outcome. Six of the seven participants who did not achieve the primary outcome failed because of prednisone usage between months 2 and 6. The primary and secondary outcomes are shown in table 2.
Primary and secondary outcomes
Disease activity
Both the IgG4-RD RI and the PGA scores declined steeply over time. The IgG4-RD RI decreased between baseline and all subsequent visits (p<0.00001) (figure 1A). The PGA showed a decline (figure 2). The PGA decreased over time between baseline and all subsequent visits (p<0.00001). Between each consecutive visit, the PGA declined significantly at 1, 3, 5, and 6 months (p<0.005). Twenty-three (73%) of the participants achieved a PGA score of 0. The total IgG4-RD RI scores reflected PGA assessments more closely if serum IgG4 concentrations were excluded from the measure (figure 1B).

IgG4-related disease Responder Index (IgG4-RD RI) decreased between baseline and all subsequent visits. (A) Includes serum IgG4 in the RI and (B) excludes serum IgG4 in the RI.

Change in the physician's global assessment (PGA) over time.
Nineteen participants (63%) had organ system involvement classified as urgent at baseline. The organs affected most commonly by urgent disease at baseline were the pancreas (n=6), bile ducts (n=5), kidneys (n=4), lungs (n=4), and orbit (n=3). Over the course of the trial, four participants experienced disease flares with urgent disease manifestations (2 at 3 months, 1 at 10 months, 1 at 12 months). The organs involved in the urgent disease flares were the pancreas and carotid artery (month 3), bile ducts (month 10), and lungs (month 12).
Laboratory values
Nineteen participants (63%) had elevated serum IgG4 concentrations at baseline. Among the 11 (37%) with normal values, only two were on prednisone. Of the 19 with elevated serum IgG4, the mean serum level declined from 911 mg/dL (range 138–4780 mg/dL) at baseline to 422 mg/dL (range 56–2410 mg/dL) at 6 months (p<0.05) (figure 3). However, only 8 of those 19 achieved normal values following treatment. Serum IgG4 concentrations began to decline quickly after treatment and decreased substantially over time in all participants with IgG4 elevations at baseline, but declines in serum IgG4 concentrations trailed overall clinical improvement. The normalisation of serum IgG4 concentrations, if achieved, did not occur in some cases until many months after participants had achieved clinical remissions.

{kind=link}
{kind=link}
{kind=link}
Serum IgG4 concentration over time. Among the 19 patients with elevated serum IgG4 at baseline, the mean concentration declined from 911 mg/dL to 422 mg/dL at 6 months. However, only 8 out of 19 patients had complete normalisation of serum IgG4.
The ESR and CRP showed similar declines between baseline and 6 months, with the ESR decreasing from a mean of 37 mm/h (range 7–123 mm/h) to 19 mm/h (range 1–89 mm/h) (p<0.005) and the CRP declining from 16.6 mg/dL (range 0.5–189.6 mg/dL) to 3.2 mg/dL (range 0.1–13 mg/dL) (p<0.005).
Outcomes at 12 months
Twenty-seven participants (90%) were off GC entirely at 12 months. Only two (7%) were unable to discontinue GC entirely at some point over 12 months of follow-up. Fourteen (47%) and 12 (40%) participants achieved and maintained complete remissions through 6 and 12 months, respectively.
Complete remission with and without serum IgG4
Complete remission was achieved in 18 (60%) of the 30 participants at any time over the 12-month follow-up period (47% at the 6-month time point). When the serum IgG4 concentration was excluded from the IgG4-RD RI, these figures increased to 20 (67%) at any time and 18 (60%) at 6 months.
Multiple versus single organ involvement
The mean initial IgG4-RD RI was lower among participants with limited organ involvement, defined as only one or two active organs, compared with that of participants with multiorgan disease, defined as the involvement of three or more organs. The mean IgG4-RD RI for the subgroup of participants with limited organ involvement was 9±2, compared with 18±8 for those with multiorgan disease (p<0.001). Participants with limited organ involvement had lower baseline serum IgG4 levels (mean 207±195 mg/dL vs 1251±1532 mg/dL; p=0.01). Participants with limited organ involvement were more likely to achieve complete remission within 6 months compared with those with multiorgan involvement (12/16 vs 6/14 subjects including serum IgG4 in the assessment; p=0.10; 14/16 vs 7/14 subjects if serum IgG4 excluded; p<0.05).
Treatment responses within specific organs
No clear pattern of treatment refractoriness according to organ involvement emerge. Persistent disease activity in the lungs (n=3), orbits (n=3), parotids (n=2), sinuses (n=2), pancreas (n=1), lymph nodes (n=1), and kidneys (n=1) was associated with failure to achieve complete remission at month 6. Of those participants with retroperitoneal fibrosis, one out of three had persistent disease at month 6. Three participants did not achieve complete remission only because the serum IgG4 did not normalise. The presence of persistent disease led to primary outcome failure in only one participant. An interim flare and/or or prednisone usage between months 2 and 6 was the most common reason for primary outcome failure (n=6).
Damage
Many participants had incurred substantial damage from IgG4-RD by the time of enrolment (table 3). The pancreas was the organ damaged most often. Pre-existing pancreatic damage was present in 47% of participants, many of whom had pancreatic insufficiency. Other common sites of damage included the biliary tree, salivary glands, and lymph nodes. Seventeen participants (57%) had incurred damage from surgery (eg, partial pancreatectomy, n=3) performed before the diagnosis of IgG4-RD had been established.
Sites of organ damage at baseline and during follow-up
Adverse events
Two subjects were hospitalised for infections during the trial period, one for a Klebsiella urinary tract infection and the other for Legionella pneumophila pneumonia. The Legionella infection was present unrecognised at the time of the baseline infusion. Four additional subjects were hospitalised. The events precipitating these hospitalisations were a cold agglutinin-mediated haemolytic anaemia, amaurosis fugax leading to a carotid endarterectomy, unstable angina, and surgery for an IgG4-related orbital pseudotumor. The cold-agglutinin anaemia, caused by an IgM antibody, had no known relationship to either IgG4-RD or to RTX. The participant with amaurosis fugax, an elderly diabetic male, was suspected of having atherosclerotic disease as the cause of his vascular lesion. The examination of the carotid artery, however, showed an intravascular focus of IgG4-RD. His recurrent amaurosis symptoms resolved completely following carotid endarterectomy. The participant with unstable angina had a long-standing history of coronary artery disease. The worsening of his angina had no apparent relationship to RTX. Eye surgery on a patient with IgG4-related orbital pseudotumor was complicated by blindness in the eye affected by the pseudotumor. Finally, one participant was diagnosed with transitional cell cancer of the bladder. The review of his pretrial studies demonstrated that the malignancy had been present before enrolment.
Discussion
Results of this prospective, single-arm pilot trial of RTX provide strong evidence that B cell depletion is an effective treatment for IgG4-RD. All of the participants enrolled had active disease and many had disease manifestations requiring urgent treatment. The great majority (87%) were treated with RTX alone, and 77% achieved the primary outcome. Ninety-seven per cent of the participants enrolled achieved disease responses that were maintained at 6 months. These favourable results were obtained despite the enrolment of a population enriched with patients at high risk for relapsing or refractory disease due to the presence of multiorgan involvement, prior relapse, and the failure of previous DMARD therapy.
Perhaps the greatest indication of efficacy is the degree to which these patients were managed without GCs. Only eight required prednisone at any point in the trial (four were receiving prednisone at baseline). At 6 and 12 months, only three (10%) participants remained on GCs, one of whom remained on prednisone for his cold agglutinin-mediated anaemia, not IgG4-RD. Thus, the RTX regimen employed in this trial was highly effective at controlling disease without concomitant GCs.
The responses observed in most participants exceeded the improvement required for the primary outcome by a substantial margin. Among the 23 participants who achieved the primary outcome, the mean IgG4-RD RI declined to 1 at 6 months. In addition, 23 (73%) of the participants achieved PGA scores of 0 mm (from a baseline of 63 mm), consistent with complete return to health. Complete remission—an IgG4-RD RI of 0 and no prednisone—is a high bar for success, yet 40% achieved maintained this status at 1 year. The retreatment of patients at some point might have led to even more impressive efficacy outcomes, but this hypothesis will need to be pursued in other studies. In this trial, the RTX retreatment time points were at month 8, 2 at month 10, and one subject at 1 year. This provides an indication of the duration of effect of RTX, which appears to extend beyond the time by which most patients begin to replete their B cell pool. There are few rigorous, prospectively collected data on the outcomes of GC-treated patients with IgG4-RD. Most are derived from retrospective investigations in AIP; as a rule, GCs were not discontinued entirely in most studies. Most patients reported in retrospective case series of GC treatment and in the single prospective trial of prednisolone remained on 5–10 mg/day of prednisone. In a recent international multicenter report, 31% of patients with IgG4-related AIP experienced relapse. Relapse was most common following steroid discontinuation, but 18% of relapses occurred while on maintenance GC.25 Relapse rates are even higher in IgG4-RD patients with multisystem disease and those with intrahepatic biliary involvement.25
Small case series have shown that RTX has promise in treating IgG4-RD.10 ,14–16 ,26 Mechanistic studies suggest that this strategy is effective at least in part because it depletes all measureable peripheral B cells, preventing the repletion of short-lived plasmablasts and plasma cells that generate the large serum concentrations of IgG4 observed in some patients.4 ,14 ,15 ,21 ,27 It is likely that cells of the B cell lineage also have important functions in IgG4-RD beyond IgG4 production, such as antigen presentation to T cells and/or the synthesis of cytokines that sustain T cell memory.4 ,27 The response to RTX among patients with IgG4-RD appears to be variable, with some patients having prolonged periods of remission, others experiencing recurrent disease activity 5–12 months after the initial response to treatment, and a small minority failing to achieve sufficient responses with B cell depletion alone. Potential mechanistic explanations for these differences are now being explored.
The results of this trial provide further indications of the shortcomings of the serum IgG4 concentration as both a diagnostic marker and a correlate of disease activity. More than one-third of participants enrolled (37%) did not have an elevated serum IgG4 at baseline. In addition, among those with elevated serum IgG4 concentrations, the levels declined significantly after treatment but did not normalise despite generally excellent control of disease. Furthermore, in a post hoc analysis, the IgG4-RD RI and PGA correlated better with each other if the serum IgG4 was excluded from the IgG4-RD RI calculation. Other studies have also shown that the serum IgG4 concentration is a poor predictor of relapse after GC therapy,25 does not distinguish reliably between IgG4-RD and cancer,9 ,28 and has other shortcomings as a biomarker of disease activity.6 ,21–23 It therefore seems appropriate to exclude the serum IgG4 concentration from the IgG4-RD RI. In fact, the BVAS/WG, shown to be a robust measure of disease activity in multiple clinical trials of ANCA-associated vasculitis, excludes laboratory parameters such as ANCA titres, ESR, and CRP from the measure.
This trial includes a number of important strengths. The clinical manifestations of the participants enrolled in this trial were broad, a reflection of the protean nature of IgG4-RD. Fourteen organ systems comprising a minimum of 38 different clinical manifestations were identified among the participants. Although the responses across the range of organ involvement were excellent, it is possible that greater experience with IgG4-RD will identify subsets of clinical findings that are likely to respond best to B cell depletion. We anticipate, for example, that patients with multiorgan disease characterised by substantial elevations in serum IgG4 concentrations are most likely to demonstrate clinical responses that are readily evaluable in a clinical trial setting. In contrast, responses may be more difficult to discern among patients whose organ manifestations reflect primarily the stages of advanced fibrosis. Another important strength of this trial is the fact that RTX was used as a sole remittive agent in almost 90% of trial participants. The protocol therefore permitted a reasonable estimate of the effects of B cell depletion alone.
The trial also had several weaknesses. This was an uncontrolled trial and hence the results do not prove definitively that RTX is effective in IgG4-RD. However, the history of resistant or relapsing disease in most participants, the fact that RTX was the only new treatment medication employed in almost all participants, and the objectivity of our assessment tools employed (eg, serum IgG4 concentrations and acute phase reactants) support the suggestion of powerful treatment effects reflected in the IgG4-RD RI and PGA assessments.
In conclusion, the findings from this prospective pilot trial support the observations from small retrospective studies indicating that B cell depletion is an effective and important treatment for IgG4-RD. GC should remain the first treatment approach for most patients at the present time, assuming the absence of major contraindications to GC therapy. However, the incomplete or unsustained responses to GCs observed in many IgG4-RD patients, coupled with the fact that many IgG4-RD patients are middle-aged to elderly and have co-comorbidities contraindicating long-term GCs, indicate that B cell depletion may have a substantial role in a large percentage of IgG4-RD patients. This may be particularly true for patients with multiorgan disease. A randomised clinical trial will be necessary to refine the optimal use and determine the appropriate role of B cell depletion in IgG4-RD.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
- Data supplement 2 - Online table
Footnotes
Handling editor Tore K Kvien
Funding This study was supported by Genentech. JHS has served as a consultant to Genentech in the area of IgG4-related disease.
Competing interests None.
Ethics approval The trial was approved by the Institutional Review Boards of the Massachusetts General Hospital and the Mayo Clinic.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors will entertain reasonable proposals for data-sharing that are submitted in writing to JHS. Requests for the use of any unpublished data pertaining to this trial will be considered upon written request.