Article Text

Abstract
Objective: To determine the frequency and clinical impact of anticardiolipin antibodies (aCL) in patients with rheumatoid arthritis treated with infliximab and etanercept.
Methods: 121 patients from the Stockholm tumour necrosis factor α (TNFα) follow up registry (STURE) treated with infliximab or etanercept were studied.
Results: At baseline 9/65 (14%) infliximab and 10/56 (18%) etanercept treated patients had positive aCL. After 3 months the frequencies of aCL positivity were 29% (p<0.05 compared with baseline) and 27%, respectively, and after 6 months 28% and 25%. Increases were seen for both IgG and IgM aCL. Increasing age, a higher number of prior DMARDs, and higher DAS28 were predictors for the development of aCL. In the infliximab treated patients, 26/30 (87%) aCL(−) but only 7/14 (50%) aCL(+) patients met the ACR20 criteria (p<0.05), and the frequency of treatment limiting infusion reactions in the aCL(+) patients was higher than expected (17%). aCL positivity in the etanercept treated patients did not show such a clinical correlate. Four patients had thromboembolic events, of whom two were aCL(+) and two aCL(−).
Conclusion: Frequencies of both IgM and IgG aCL positivity increase in patients treated with these TNFα antagonists for 3 months or longer. Increasing age, a greater number of prior DMARDs and a greater disease activity at baseline are predictors for the development of aCL. The development of aCL during treatment with infliximab, but not etanercept, is associated with worse clinical results and more frequent serious infusion reactions. aCL are an important class of autoantibodies associated with TNFα blocking therapy.
- aCL, anticardiolipin antibodies
- ACR, American College of Rheumatology
- ANA, antinuclear antibodies
- DAS28, disease activity score
- DMARDs, disease modifying antirheumatic drugs
- ELISA, enzyme linked immunosorbent assay
- RA, rheumatoid arthritis
- STURE, Stockholm TNFα follow up registry
- TNFα, tumour necrosis factor α
- tumour necrosis factor α blockers
- rheumatoid arthritis
- anticardiolipin antibodies
Statistics from Altmetric.com
- aCL, anticardiolipin antibodies
- ACR, American College of Rheumatology
- ANA, antinuclear antibodies
- DAS28, disease activity score
- DMARDs, disease modifying antirheumatic drugs
- ELISA, enzyme linked immunosorbent assay
- RA, rheumatoid arthritis
- STURE, Stockholm TNFα follow up registry
- TNFα, tumour necrosis factor α
Tumour necrosis factor α (TNFα) blocking agents are now widely used in the treatment of aggressive rheumatoid arthritis (RA) and have proved to be effective and relatively safe.1–,10
Earlier studies have shown the induction of autoantibodies during treatment with TNFα blocking agents.11 Thus, antinuclear antibodies (ANA) have been described in 53–68% and anti-double stranded DNA (anti-dsDNA) antibodies in 5–10% of patients with RA treated with the TNFα blocking agent infliximab (Remicade).1–3,5,11 In patients treated with etanercept (Enbrel) the same autoantibodies are seen in 11% and 5–13%, respectively.7,8 Only limited data have been published about the induction of anticardiolipin antibodies (aCL) during TNFα blocking treatment. Thus, Elliott et al found aCL in one of 20 patients with RA treated with anti-TNFα (cA2) in an open trial lasting 8 weeks.4 Rankin et al measured the serological effects of repeated doses of the humanised anti-TNFα antibody CDP 571 in patients with RA and found that some patients develop positive aCL (IgG).12 Ferraccioli et al showed variations in aCL titres over time in etanercept treated patients with concomitant bacterial infection, where lowering of titres was seen after treatment with antibiotics.13 In the normal population (healthy blood donors) aCL are found in 2–6%, and in an aging population in up to 12%.14,15 In patients with RA aCL have been found at even higher frequencies.16,17 aCL, in general, are associated with thromboembolic disease, but their clinical significance in RA is uncertain and their presence has been considered to be a non-specific marker of activation of the immune system.18
In this study we assessed the frequency of aCL in patients with RA treated with infliximab or etanercept, and their relation to clinical outcomes.
PATIENTS AND METHODS
Patients
We retrospectively studied 121 patients from the Stockholm TNFα follow up registry (STURE), who were at least 18 years of age and fulfilled the1987 criteria for RA of the American College of Rheumatology (ACR).19 Treatment of these patients conventionally had failed and they then received treatment with the TNFα blocking agents infliximab (n = 65) or etanercept (n = 56). Over 90% of the patients receiving infliximab and 50% of those receiving etanercept were also treated with methotrexate 7.5–15 mg/week. Infliximab was given according to standard protocol guidelines: 3 mg/kg at 0, 2, and 6 weeks and every 8th week thereafter. Etanercept (25 mg) was given subcutaneously twice weekly.
Blood samples and laboratory analyses
Analyses for aCL, ANA, rheumatoid factor, and IgG anti-DNA were performed at baseline and after 3, 6, and 12 months of treatment. aCL was measured with an in-house enzyme linked immunosorbent assay (ELISA), calibrated against the Harris standard for IgG and IgM aCL, respectively. A rabbit antihuman IgG, γ chain-specific conjugate, conjugated to horseradish peroxidase (Dako p 0214) was used. Results were given in IU/ml and the cut off point was determined at 14 IU/ml in a healthy blood donor population. Low, medium, and high levels were defined as 14–20, 21–80, and >80 IU/ml respectively. ANA were assayed using HEp-2 cells as substrate (Immunoconcepts) and FITC antihuman IgG conjugate (Binding Site). IgG anti-DNA antibodies were measured with an ELISA (Pharmacia Diagnostics). Rheumatoid factor was measured by nephelometry (Beckman).
Clinical outcomes
The following clinical outcomes were measured at baseline and after 3, 6, and 12 months: swollen joint count, tender joint count, visual analogue scale for global assessment and pain by the patient, a five point Likert scale for physician’s global assessment, Health Assessment Questionnaire—Disability Index,20 and laboratory data (acute phase reactant values of C reactive protein, erythrocyte sedimentation rate, and haemoglobin concentrations).
The ACR, response criteria (ACR20)21 and the EULAR response criteria based on disease activity score-28 (DAS28)22 were determined at baseline and after 3, 6, and 12 months of treatment.
Adverse effects
We analysed the frequency of treatment limiting infusion reactions and of thromboembolic events.
Statistical analysis
Statistical analysis was performed using Statview 5.0.1 software (SAS Corp, Cary, NC). Results of the analysis are reported as mean values and standard deviations (SD) and comparisons were performed using χ2 test and Student’s t test.
RESULTS
Characteristics of the patients
Ninety eight women and 23 men were studied. The mean age was 52 years (range 21–81), the mean disease duration was 14 years (range 1–43), 90% were seropositive, and the median number of prior disease modifying antirheumatic drugs (DMARDs) was five.
Frequency of aCL increases during treatment with TNFα blockers
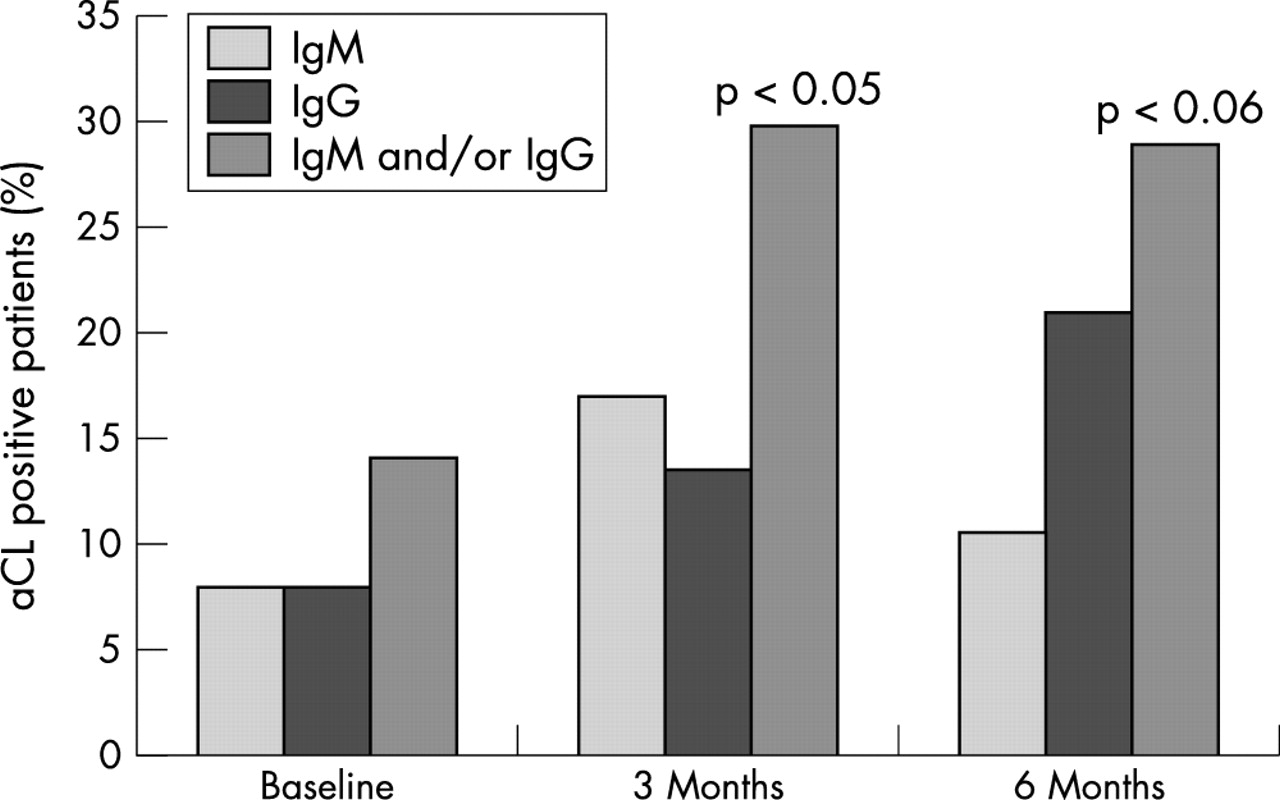
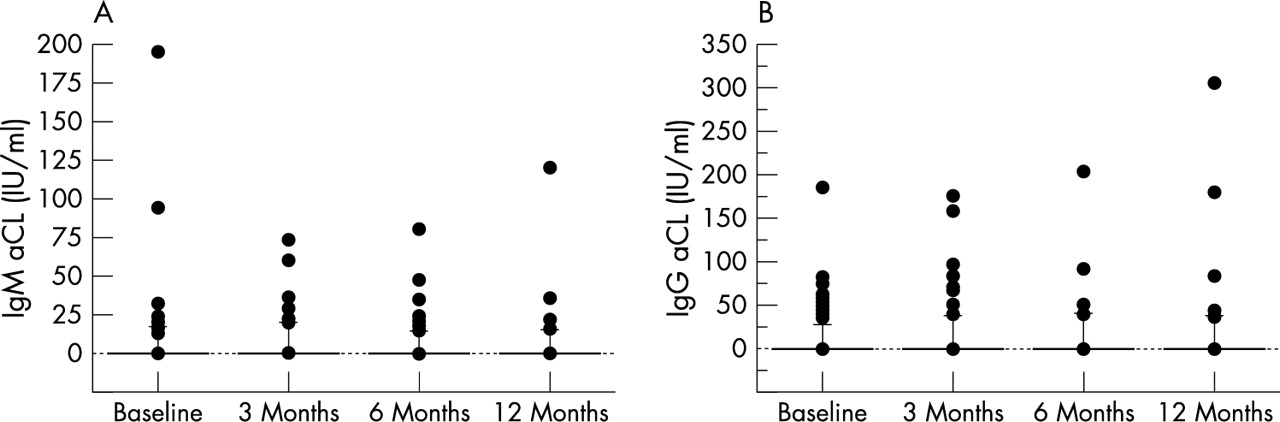
At baseline 9/65 (14%) infliximab and 10/56 (18%) etanercept treated patients had positive IgM and/or IgG aCL, at low to medium levels. After 3 months the frequencies of aCL positivity were 29% (p<0.05 compared with baseline) and 27%, respectively, and after 6 months 28% and 25%, respectively. Increases were seen for both IgG and IgM aCL (figs 1 and 2⇓⇓). Increasing age, a greater number of prior DMARDs, and a greater disease activity at baseline by DAS28 were positive predictors for development of aCL after 3 months of treatment. No correlation was seen between ANA positivity and the development of aCL (table 1⇓). The mean aCL IgM and IgG titres showed a small, non-significant increase over time (fig 3⇓).
Predictors of aCL positivity at baseline and of seroconversion

Percentage of aCL(+)patients at baseline and after 3 and 6 months of treatment with infliximab. Percentage positive for IgG aCL: p<0.05 for linear trend.

Percentage of aCL(+)patients at baseline and after 3, 6, and 12 months of treatment with etanercept.

(A) IgM aCL titres (IU/ml) in all patients at baseline and after 3, 6, and 12 months of treatment. (B) IgG aCL titres (IU/ml) in all patients at baseline and after 3, 6, and 12 months of treatment.
aCL are associated with worse clinical results
ACR responses and DAS values were studied in 44 infliximab treated patients. Twenty six of 30 (87%) aCL(−) patients were ACR20 responders while only 7/14 (50%) aCL(+) patients met the ACR20 criteria (p<0.05) (fig 4⇓). Assessment of the DAS28 response after 3 months showed that the aCL(−) patients had a mean (SD) DAS28 of 3.6 (0.15) compared with the aCL(+) patients who had a mean DAS28 of 4.3 (0.24) (p<0.05). However, baseline DAS28 values were also higher in the aCL(+) patients and there were no significant differences between the changes in DAS28 in the two groups (not shown).
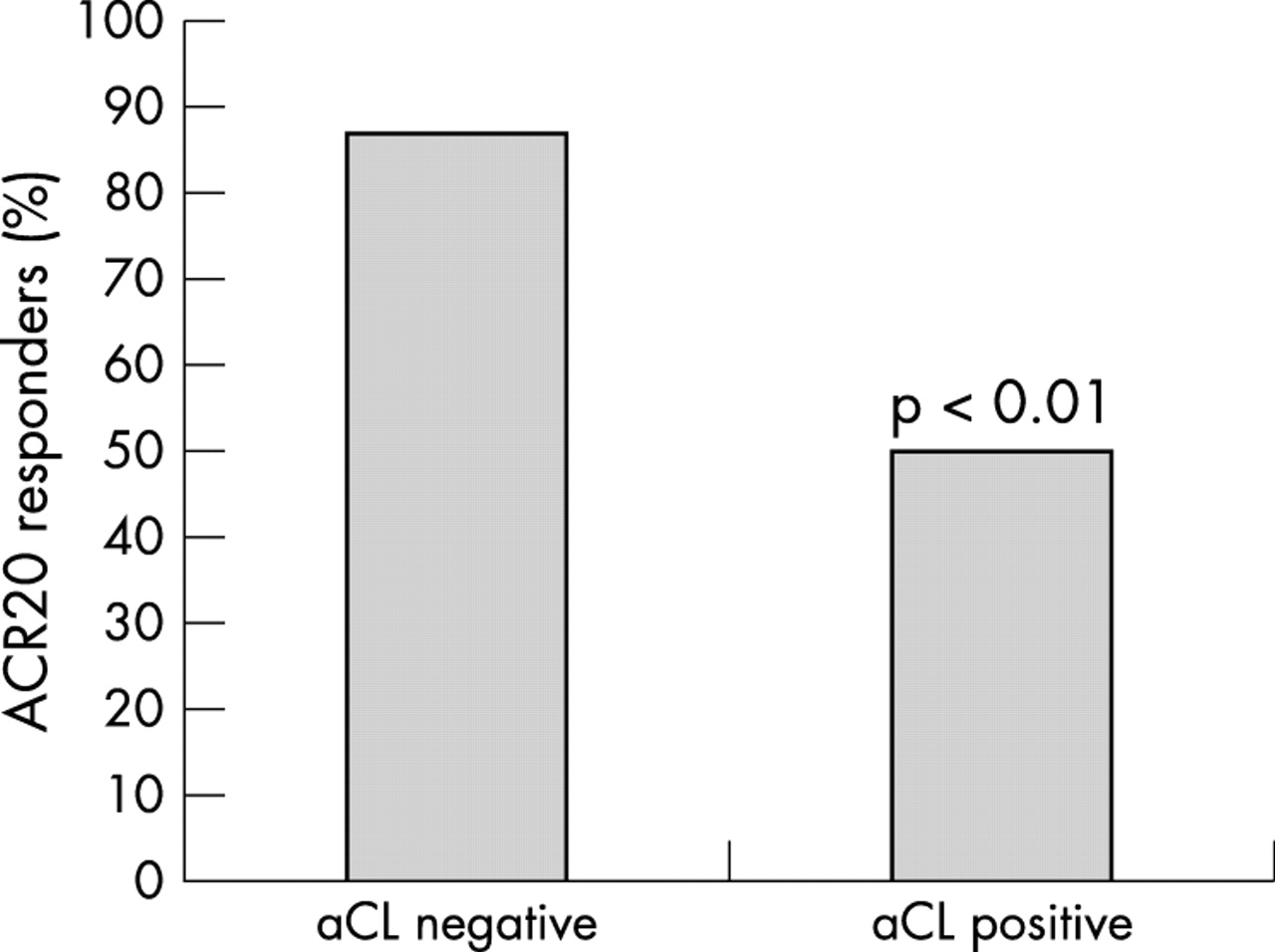
Percentage of ACR20 responders to treatment with infliximab in aCL(−) and aCL(+) patients. Comparison is by χ2 test.
In etanercept treated patients, clinical responses were similar between aCL(+) and aCL(−) patients (data not shown).
aCL are associated with more frequent adverse outcomes
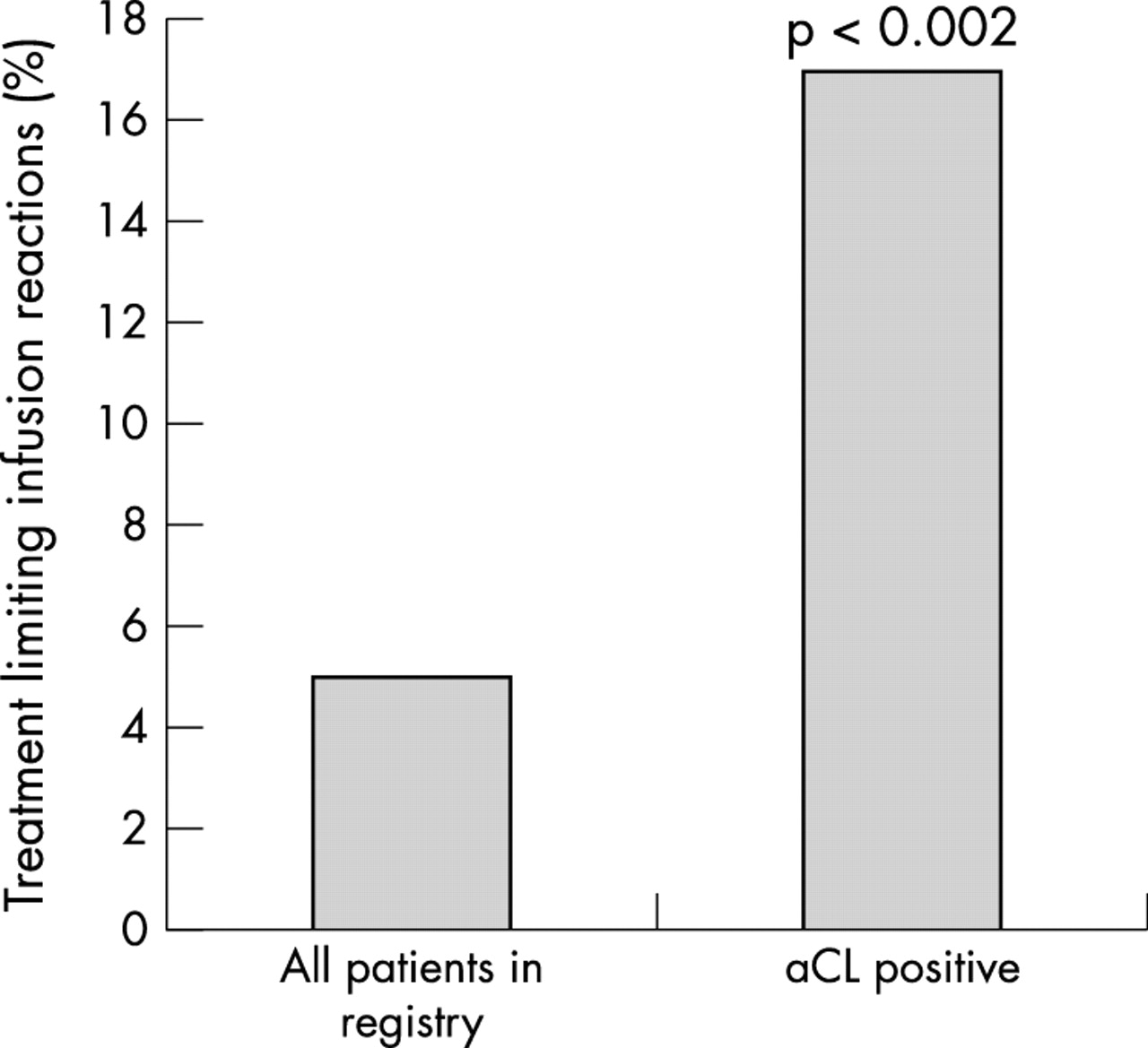
The frequency of treatment limiting infusion reactions in the aCL(+) patients was 17% compared with 5% in the entire TNFα registry (p<0.05) (fig 5⇓). The adverse effects were fevers, chills, urticaria, chest pain, dyspnoea, sickness, flushing with headache, tachycardia, hypotension, and anaphylactic reactions. Four patients had thromboembolic events (three receiving infliximab, one receiving etanercept). Two of these patients were aCL(+) and two aCL(−). Of the aCL(+) patients, one had a pulmonary embolus and the other a stroke. Thus, frequencies for thromboembolic events are 7% and 2.6% in the aCL(+) and aCL(−) patients, respectively, which is not statistically significant (relative risk 2.7, 95% confidence interval 0.8 to 4.6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of treatment limiting infusion reactions in aCL(+) patients compared with all patients in the registry (infliximab treatment only). Comparison is by χ2 test.
DISCUSSION
In our patients we found a statistically significant increase in the frequency of IgM and/or IgG aCL positivity among patients treated with infliximab for 3 months or longer. Similar results were seen for etanercept, suggesting that this may be a class effect of the TNFα blocking agents. Previous studies on treatment with TNFα blocking agents and development of autoantibodies have mainly focused on ANA and anti-DNA. Thus, we believe that this is the first systematic description of increased aCL frequency in patients treated with TNFα antagonists.
A possible criticism of the study could be that patients treated with TNFα blocking agents might have reduced or discontinued glucocorticoid treatment and this might in itself allow the development of autoantibodies. Supporting this, a small but statistically significant decrease in mean glucocorticoid dosage was seen in these patients (not shown). However, the absolute change in dosage was small. Moreover, Lockshin et al showed that glucocorticoid treatment even at high doses did not change the presence of aCL nor did it lower the titres.23
One possible explanation for the induction of aCL positivity in patients treated with TNFα blocking agents is that the down regulation of TNFα induces up regulation of interleukin 10, which in turn activates autoreactive B cells24 and thus induces autoantibody production. Alternatively, lower levels of TNFα might lead to a generalised increase in Th2 activity, which even through other cytokine pathways might leads to B cell activation24 and autoantibody formation. Ferraccioli et al have shown a relationship between clinically overt infections and aCL formation.13 Thus, a third explanation might be that TNFα blockade allows a subtle increase in bacterial stimuli from the environment, leading to increased aCL formation.
Increasing age, greater number of prior DMARDs, and more severe disease activity were predictors for the development of aCL in this study, but obviously, these factors are not independent.
We found that the development of aCL positivity during treatment with infliximab had prognostic significance because it was associated with worse clinical results and more frequent serious infusion reactions. However, it is unclear how the association between aCL positivity and clinical outcome is mediated. One could speculate that the precise immunopathologies of RA are different from patient to patient, and that in some patients autoreactive B lymphocytes might have a more causal role. Such patients might therefore be less likely to respond to TNFα blockade and also more likely to produce aCL. Indirect evidence for the existence of such a patient group with more B cell dependent disease has come from clinical studies with the B cell ablative monoclonal antibody rituximab.25,26
In this study we found only a few patients with anti-dsDNA antibodies. However, it should be noted that we only measured IgG anti-dsDNA and not the IgM isotype, which in earlier studies was shown to be preferentially induced by TNFα blocking treatment.1–3,6–8,11 Among our patients only one developed IgG anti-dsDNA antibodies (both by an ELISA and by the Crithidia luciliae test) during treatment with infliximab. This patient developed a lupus-like syndrome with pleuropericarditis.
Our study may have some practical clinical implications. Although aCL in general are associated with an increased risk for thromboembolism, the small number of events in these patients did not allow us unequivocally to identify an increased risk. Continued long term follow up of patients treated with biological agents, such as is continuing through the Swedish ARTIS and STURE registries, is therefore of critical importance.
An important clinical question is whether all patients treated with the TNFα blocking agents should be screened for aCL. In this study, aCL positivity predicts less benefit from treatment with infliximab and a higher risk for a treatment limiting infusion reaction. Therefore, knowledge of aCL serology might, in principle, lead to a change in the risk/benefit assessment and might affect the decision about which antirheumatic treatment to choose. This may become a more germane consideration if a significantly greater number of therapeutic choices become available, which may well be the case in a number of years.
Another question is what should be done if a patient develops aCL during treatment with TNFα blocking agents. We believe that such patients should be treated as all subjects with fortuitously detected aCL, and that the aCL titres should be followed up periodically if found to be positive. However, this does not necessarily mean that aCL(+) patients need to stop the TNFα blocking treatment.
In future studies, it might be interesting to look more closely at the general immunoglobulin production and even the production of antibodies against infliximab and etanercept in our patient group. It would also be interesting to see if the aCL(+) patients would respond better to B cell ablative therapy. We are also following up our patient cohort for a longer period of time to see if more patients develop these autoantibodies, the longer the treatment continues.
In summary, aCL are induced in patients with RA treated with the TNFα blocking agents infliximab and etanercept. A statistically significant increase in frequency is seen for IgM and IgG aCL already after 3 months of treatment with infliximab. Etanercept treated patients show the same pattern, suggesting a class effect of the TNFα blocking agents. aCL positivity in patients treated with infliximab predicts worse clinical outcomes and more frequent treatment limiting infusion reactions. aCL are an important class of autoantibodies associated with TNFα blocking therapy.
Acknowledgments
The Swedish TNFα follow up registry is owned by the Swedish Rheumatological Society (SRF), and supported by grants from Wyeth Lederle and Schering-Plough. This study was supported by the Swedish Rheumatism Association.