Article Text

Abstract
Objectives: To obtain evidence for dose response and to extend evidence of safety and efficacy for B lymphocyte depletion in rheumatoid arthritis.
Methods: Twenty two patients with rheumatoid arthritis received a total of 29 treatments with five different combinations of rituximab (RTX), cyclophosphamide (CP), and/or high dose prednisolone (PR) on an open basis as follows; cohort I: RTX 1400 mg/m2, CP 750×2+PR; cohort II: RTX 300–700 mg/m2, −CP±PR); cohort III: RTX 600–700 mg/m2, CP 750×2+PR; cohort IV: RTX 1200 mg/m2, CP 750×2−PR; cohort V: RTX 500 mg/m2, CP 750×2+PR. American College of Rheumatology (ACR) criteria of improvement at six months were chosen as the primary outcome measure. Disease activity scores and total duration of improvement and of B cytopenia were also recorded.
Results: No major adverse events attributable to treatment were seen. ACR grades of improvement at six months were as follows: cohort I: ACR70×3, ACR50×2; cohort II: ACR20×1, ACR0×3; cohort III: ACR70×6, ACR50×2, ACR20×2; cohort IV: ACR70×2, ACR50×2, ACR20×1, ACR0×1; cohort V: ACR0×4.
Conclusions: B lymphocyte depletion in rheumatoid arthritis has so far proved to be safe and associated with major improvement with protocols including RTX 600 mg/m2 or more and CP, but not with more limited protocols. These observations provide an initial basis for the design of formal trials of B cell depletion and other B cell directed treatments, including a phase II controlled trial now in progress.
- rituximab
- anti-CD20
- rheumatoid arthritis
- autoimmunity
- ACR, American College of Rheumatology
- DMARDs, disease modifying antirheumatic drugs
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- TNFα, tumour necrosis factor α
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- DMARDs, disease modifying antirheumatic drugs
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- TNFα, tumour necrosis factor α
For much of the past two decades, rheumatoid arthritis (RA) has been considered chiefly as a T cell mediated disease,1 based on the association with HLA-DR allotype,2 the dominance of T cells (chiefly Th1) over B cells in RA synovium,3 and an assumed dependence of proinflammatory macrophage cytokine production on T cell activation. In the past few years, however, there has been increasing interest in the role of B cells. A number of B cell directed treatments are now under review, of which B cell depletion with rituximab was the first to be applied in the clinic.4
The observations quoted above are consistent with important roles for B cells.5 Antibody production is dependent on antigen presentation by HLA-DR.6 T cells almost always outnumber B cells in inflammation. Th1 cells can support antibody production and may well do so in RA synovium, where plasma cells are prominent. The resolution of synovitis after tumour necrosis factor α (TNFα) blockade7 suggests that the leucocyte populations present may simply reflect trafficking due to TNFα-induced expression of adhesion molecules on synovial vasculature. Finally, the lack of consistent autoreactive T cell responses to IgG or, indeed, other autoantigens in RA and the possibility of T cell independent signals for macrophage TNFα production casts doubt on many assumptions about T cell involvement.
B cells and their products may have several roles in RA. A potent stimulus for TNFα production by macrophages is the cross linking of IgG Fc receptors (FcγR).8 The oligomeric IgG rheumatoid factor (RF) complexes circulating in subjects with RA9 can probably cross the endothelium, access tissue macrophages, and generate TNFα.5,10 Involvement of FcγR in TNFα production in RA is supported by the fact that the only FcγR which can apparently generate TNFα in response to very small complexes, FcγRIIIa,11 is only expressed at high level in tissues showing macrophage activation in RA: synovial intima, serosae, alveoli, bone marrow, lymphoid tissue, sclera, salivary gland, dermis at pressure points, and Kuppfer cells.12 An immune complex based mechanism would explain why macrophage activation precedes T cell infiltration.13
B cells also contribute to immune responses through antigen presentation to T cells. Although it is often assumed that in autoimmunity autoantigens are presented to T cells, RF B cells are unusual in that they can pick up foreign antigens complexed with IgG and present them to T cells, resulting in both T cell activation and T cell help for the RF B cell.14 This interaction would explain the dependence of the disease on HLA-DR, without requiring loss of T cell tolerance.
Persistent B cell survival should require not only T cell help but also a supply of cognate antigen in the form of immune complexes containing C3d.15 IgG RF B cells are again unusual in that they secrete their own antigen in self complexing form—that is, their own survival signal. This led us to propose that the origin of persistent RF production and clinical disease in RA may be the chance generation of B cell clones which can perpetuate their existence, and that of other RF committed B cells, through IgG RF production.5 If so, removal of these cells might be expected to induce prolonged remission.
Rituximab is a chimeric monoclonal antibody that binds to the B cell surface antigen CD20.16 Expression of CD20 is restricted to the B lymphocyte lineage, initially appearing at the late pre-B cell stage of development and being lost during terminal differentiation into plasma cells. Promising results were obtained with a B lymphocyte depletion protocol based on rituximab in an initial study of five subjects described in detail elsewhere.4 We describe here our current experience with follow up of these and a further 17 subjects treated with reduced dosages of one or more of the drugs involved. Kinetic studies are also now under way to elucidate the true therapeutic mechanism.
PATIENTS AND METHODS
Subjects
Twenty two patients, satisfying the American College of Rheumatology (ACR) diagnostic criteria for RA,17 were treated for active erosive disease not adequately controlled by standard disease modifying antirheumatic drugs (DMARDs). Two patients were male and 20 female, mean age 58 years (range 33–81), mean disease duration 18 years (range 5–40). Treatment with methotrexate, sulfasalazine, and intramuscular gold had failed in all patients owing to inefficacy, toxicity, or contraindication. The number of DMARDs which had previously failed ranged from two to six (mean four). Table 1 summarises the patient characteristics.
Details of patients at entry to the study
The following patients had salient features that might have influenced outcome. Patient 11 had advanced secondary renal amyloidosis and had been receiving monthly cyclophosphamide after treatment with oral chlorambucil had failed. Patient 16 was functional grade IV with multiple osteoporotic fractures, but still had inflammatory symptoms. Patient 8 was RF negative and antinuclear antibody positive, but with erosive disease and no features of lupus. Patient 20 was seronegative and had psoriasis but a symmetrical rheumatoid pattern of disease and no nail dystrophy.
Treatment protocol
Twenty two patients received a total of 29 treatments (seven re-treatments), approved by the local hospital ethics committee. All patients gave informed consent. After encouraging progress in the first five cases, further patients were treated with protocols involving a reduction in one or more components of the original protocol. Patients were treated primarily according to individual clinical need with a protocol judged reasonably likely to provide an optimum cost-benefit profile at that time. Minor modifications of protocol were dictated by logistic or toxicity considerations, but treatments were matched as far as possible within five sequential cohorts (table 2). DMARDs (excluding steroids) were discontinued from day 0. All patients used non-steroidal anti-inflammatory drugs or analgesics as needed. Patients were re-treated either following relapse after improvement or if a reduced dose protocol failed to produce significant improvement.
Doses of drugs used in B lymphocyte depletion
Cohort I comprised the first five patients whose characteristics and one year follow up have been described in detail elsewhere.2 These patients received the following (table 2): rituximab, as four intravenous infusions on days 2, 8, 15, and 22, of 300, 600, 600, and 600 mg (200, 375, 375, 375 mg/m2) respectively (patient 5 omitted dose 4 because of an episode of fever and pleuritic pain); cyclophosphamide as intravenous infusions on days 4 and 17 of 750 mg each and oral prednisolone 60 mg on days 1–22, reducing in the three older subjects (perceived to be at higher risk of toxicity) to 30 mg on days 11–22 and then withdrawn over three weeks in subjects not previously taking steroids and, in the other cases, to 5 mg daily over six weeks.
Cohort II comprised four patients (2, re-treated from cohort I; 6; 7; 8) who received either one or two 300 mg/m2 doses of rituximab 14 days apart without cyclophosphamide (table 2). Patients 7 and 8 received oral prednisolone cover (60 mg by mouth daily for five consecutive days starting the day before the rituximab infusion).
Cohort III comprised 10 patients who received two 300–350 mg/m2 doses of rituximab and, in most cases, two doses of 750 mg of cyclophosphamide, under oral prednisolone cover (table 2). Patients received 60 mg for five days twice unless individual tolerance to steroids dictated otherwise. Patient 2 received three doses of 750 mg of cyclophosphamide. Patients 7 and 10 received two doses of 500 mg of cyclophosphamide in view of their smaller body surface area. This cohort included re-treatment of patients 2, 4, 6, and 7 from previous cohorts, and of patients 10 and 12.
Cohort IV comprised six patients treated with a protocol as in cohort I but without oral prednisolone cover (except patient 18 who had 30 mg for four days twice for anti-emesis) and compression of rituximab treatment into two infusions (table 2).
Cohort V comprised four patients who received 500 mg/m2 rituximab, with two 750 mg doses of cyclophosphamide under variable prednisolone cover (table 2).
Assessment
Patients were assessed at recruitment, before treatment, monthly for the first six months after treatment or re-treatment, every two months until one year, and every two to three months afterwards. Clinical assessment included duration of early morning stiffness in minutes, patient's assessment of pain on a 100 mm visual analogue scale, number of swollen joints (out of 28 joints), number of tender joints (out of 28 joints), and doctor's and patient's global assessment of disease activity on a 100 mm visual analogue scale. Laboratory measurements included erythrocyte sedimentation rate, serum C reactive protein concentration, full blood count, renal and liver function tests, serum immunoglobulin levels, RF by latex fixation (positive or negative), titre of rheumatoid arthritis particle agglutination test, and antinuclear antibody titre by immunofluorescence. Circulating B lymphocytes (CD19+ by flow cytometry) and total lymphocytes were measured before treatment, monthly after treatment in the first six months, and then every two months until normal. Response at six months was defined as a score of ACR20, 50, or 70, representing a 20%, 50%, or 70% minimum percentage improvement in five of eight measures, including swollen and tender joint counts, as defined by the ACR.18 Outcome was also assessed by the modified disease activity score (DAS28, calculated as 0.56×28T+0.28×28S+0.70× lnESR+0.014×GH) at six months (T, tender joint count; S, swollen joint count; GH, patient's global health assessment).19 Relapse was defined as a deterioration to less than ACR20 having achieved at least this level.
RESULTS
Clinical response
Table 3 summarises the baseline measures of disease activity. Mean follow up was 16 months (range 6–36).
Baseline characteristics of disease activity
The one year follow up for cohort I has been described previously.2 At six months, three of the five patients achieved ACR70 (table 2), which can be considered optimal in longstanding disease. The other two showed major improvement at ACR50. Three cases achieved and maintained ACR70 for at least 18 months without further treatment. The other two also achieved ACR70, but required repeat treatments. Patient 5 had rheumatoid nodules and these regressed with treatment.
Patients in cohort II were treated with a smaller dose of rituximab without cyclophosphamide and results were disappointing; only one patient achieved ACR20 at six months. Cyclophosphamide was retained in further protocols.
Cohort III showed broadly comparable responses at six months to those in cohort I (table 2), although subject 6 remained relatively refractory. Patient 7 achieved only ACR20 at six months but improved further to ACR50 at 10 months. Five patients achieved ACR70 at six months with patient 10 repeating this score on re-treatment. Patient 12 improved to ACR50 with first treatment and after re-treatment. Patient 9 had a rheumatoid nodule that decreased in size but did not regress completely.
In cohort IV two patients achieved ACR70 and two others ACR50 at six months. Patient 15 had highly refractory disease, with severe Sjögren's syndrome. At three months she achieved ACR20 but owing to persistently active disease methotrexate was reintroduced at four months. At six months she continued to achieve only ACR20. Subject 16 only achieved ACR20 but was functional grade IV. When this was taken into account, cohort IV showed responses close to those of cohorts I and III.
In cohort V clinical benefit was short lived, all cases having relapsed by six months.
Mean duration of response to a single treatment in cohorts I, III, and IV was 14.4 months (range 6–33.5).
Figure 1 shows the mean DAS28 results for each of the cohorts.

Mean modified disease activity score (DAS28) for each cohort. Bars indicate minimum and maximum values.
Laboratory results
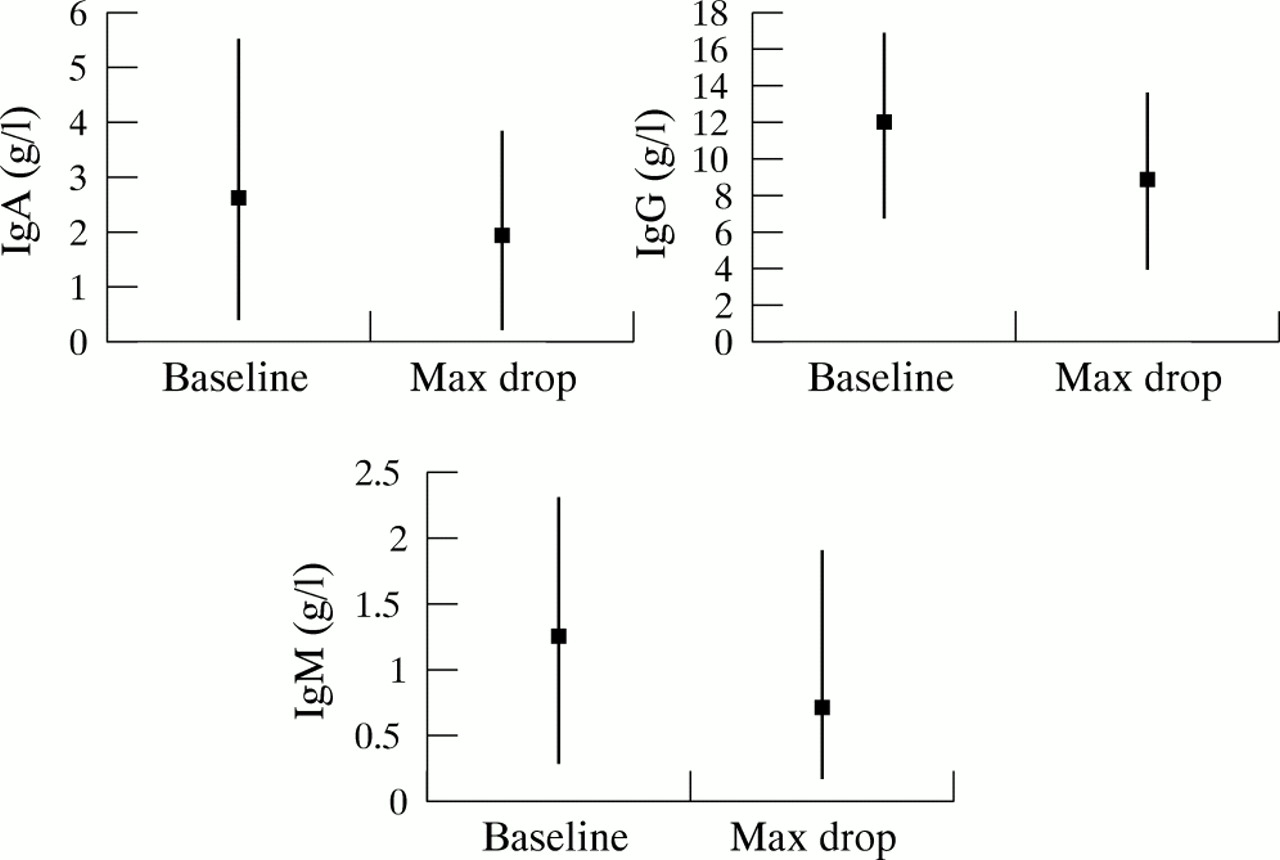
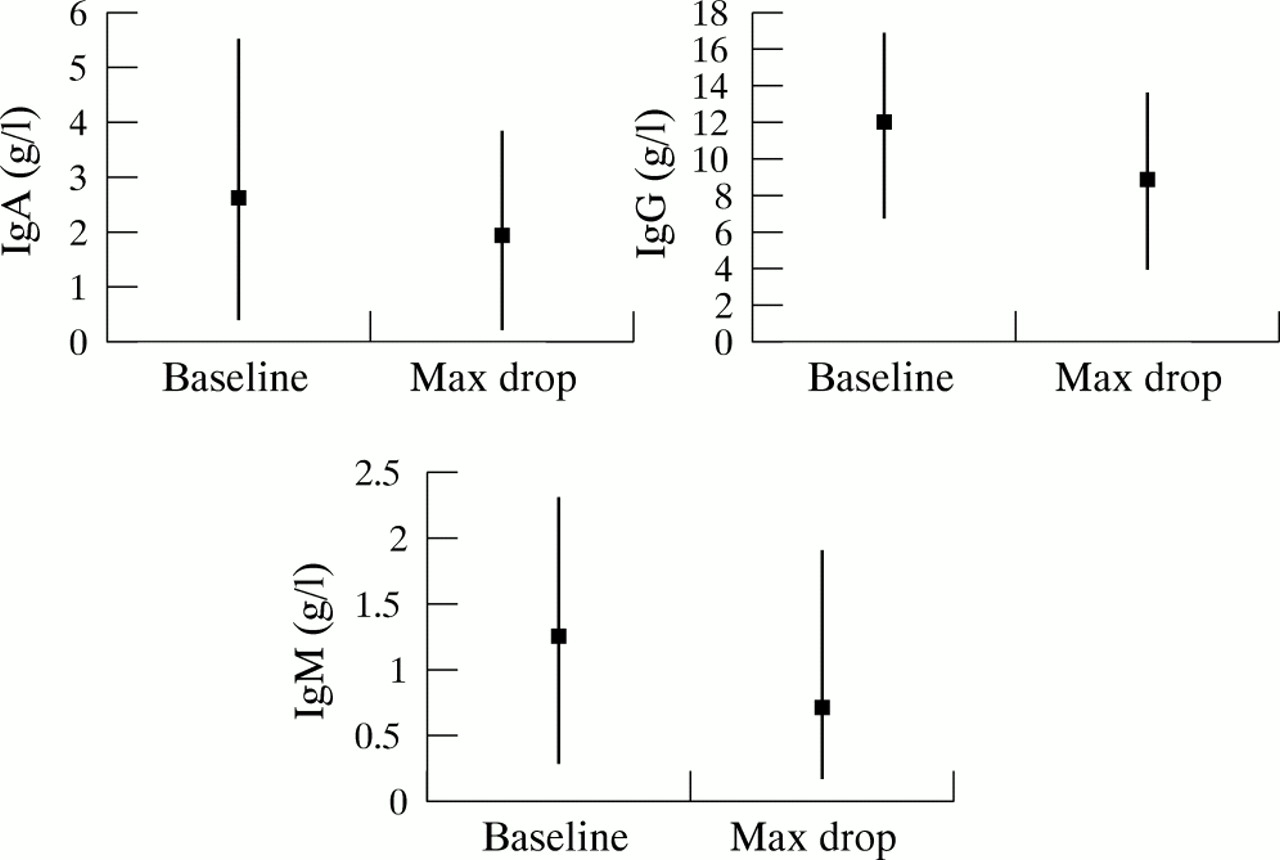
Several patients had normochromic normocytic anaemia. Haemoglobin levels followed the pattern of clinical response, normalising when disease was significantly controlled. In patient 11, with secondary amyloidosis with chronic renal insufficiency, serum amyloid A protein levels normalised and remained so at 20 months' follow up. Peripheral blood B lymphocyte counts fell to undetectable levels in all cases (except in patient 2 in cohort II when re-treated with only one dose of rituximab (300 mg/m2BSA)) and remained below normal for at least six months. The mean period of B lymphocyte depletion in cohorts I to V was 11 months, 5.5 months, 8.8 months, 10.2 months, and 7.4 months, respectively. Total lymphocyte counts showed no consistent trend. Serum total immunoglobulin levels decreased moderately. IgA dropped by a mean of 0.7 g/l (range 0–3), IgG dropped by a mean of 3.1 g/l (range 0–8.2), and IgM dropped a mean of 0.5 g/l (range 0.1–1.5) (see fig 2). In only three patients did IgG levels drop below the lower limit of normal, whereas in eight patients IgM levels fell below normal.
{kind=link}
{kind=link}
Mean total serum immunoglobulin levels. Bars indicate minimum and maximum levels.
Adverse events
No major adverse events attributable to the treatment occurred. Only two mild cases of infusion related toxicity were seen: patient 21 had fever (38.5°C) after the first rituximab infusion that responded to paracetamol; patient 17 had mild tachycardia (pulse rate 108) during her first rituximab infusion that resolved when the infusion rate was decreased. Patient 4 had phlebitis secondary to cyclophosphamide extravasation. Seven patients complained of mild to moderate nausea and occasional vomiting lasting one to two days after cyclophosphamide infusion.
During the study there were four cases of lower respiratory infection (patients 1, 5, 16, 17) and one case of acute bacterial maxillary sinusitis (patient 13) that responded to antibiotic treatment. Patient 2 had three episodes of mild transient thrombocytopenia (platelet counts over 100×109/l), with associated minor bruising only on the first episode. Patient 9 had a mild asymptomatic thrombocytopenia (platelet count 123×109/l). Patient 2 had self limiting acne rosacea at two months. Patient 7 had a self limiting erythematous rash over her nose at six months.
DISCUSSION
Clinical interpretation
The initial protocol used for B cell depletion in RA was based both on experience in lymphoma16,20 and anecdotal experience of immunoablation in RA. Primate studies suggested that rituximab did not ablate all B cells in solid tissues21 and in lymphoma, rituximab alone did not produce long term remission. Better results were being reported with rituximab combined with CHOP (cyclophosphamide, adriamycin, vincristine, and prednisolone).22 Use of adriamycin and vincristine was difficult to justify in RA, so a protocol was designed using the other elements of the anti-CD20/ CHOP regimen at doses consistent with minimal toxicity.
After good medium term results in the first five subjects, a decision was made to explore reduced levels of treatment to assist in the design of formal trials (including a controlled trial in progress) and to confirm low levels of adverse events. Patients were recruited purely on the grounds of clinical need and were, inevitably, heterogeneous. Protocol modification was designed to provide what stood a reasonable chance of being the best cost-benefit profile at the time and within cohorts some flexibility was maintained where it appeared relevant to individual requirements.
The pattern of outcomes can only be seen as a preliminary guide to further study. Nevertheless, certain general observations emerge. A low level of adverse events was confirmed. Only two mild cases of infusion related toxicity were seen, in contrast with patients with lymphoma, in whom mild to moderate reactions to the first rituximab infusion are common.16,20,22 Infections were not a significant problem.
The occurrence of major responses with higher doses of rituximab in combination with cyclophosphamide was confirmed. Moreover, there was a clear implication that the outcome was less successful when either cyclophosphamide was omitted or the dose of rituximab was lowered below 600 mg/m2. The absence of responses sustained at six months with 500 mg/m2 rituximab supports the idea that cyclophosphamide and steroid in the doses used are unlikely to be responsible for the results obtained initially.
The poor response of those who did not receive cyclophosphamide is probably clinically significant, but it is certainly possible that the patients in this cohort were atypical or the doses of rituximab suboptimal. Nevertheless, patients 2 and 7 achieved significant clinical responses when they were re-treated with the same dose of rituximab and cyclophosphamide. The possibility that useful remission in mild to moderate cases can be achieved with rituximab alone, perhaps at a higher dose, or in combination with an agent such as methotrexate, is by no means excluded.
High dose prednisolone is a common element of B lympholytic protocols and there is a suggestion that reduction in prednisolone might have reduced the efficacy or length of B lymphopenia. Prednisolone certainly appeared to decrease the incidence of nausea after cyclophosphamide and may be worthwhile for that reason.
So far RF seronegative cases have not responded, but both received low dose rituximab with (patient 20) or without cyclophosphamide (patient 8).
Immunological interpretation
Interpreting the results on a broad front, it seems reasonable to conclude that whatever the mechanism of RA, clinical disease is highly dependent on B cells and/or their products. Moreover, temporary removal of B cells seems to induce a remission which in some cases persists for several months after B cell repopulation (table 2).
The outcomes observed remain consistent with the original idea that self perpetuating IgG RF committed B cells and their products are the driving force behind the disease.4 However, current experience suggests that with the protocols used so far, all patients are likely to relapse within three years. This was expected to occur either if B cell depletion was incomplete or if pathogenic IgG RF complexes were still being generated by long lived plasma cells at the time of B cell repopulation.
At present, difficulties in assaying pathogenic complex-forming IgG RF mean that crucial pieces of evidence about their role are difficult to obtain. IgM RF titres are a poor surrogate for IgG RF, and even more so for pathogenic subsets. Studies of RF isotype and immune complex kinetics are now under way.
Improvement after B cell depletion might also reflect the role of antigen presenting B cells in T cell activation. However, several factors point in the opposite direction. Improvement after B cell depletion often progressed over several months, despite depletion being more or less immediate. In most RA synovia, B cells make up a tiny minority of antigen presenting cells and it seems unlikely that T cells should require antigen to be presented by B cells alone. B cells are rarely present in nodules, which also regressed. There was no clinical evidence of loss of T cell function in other ways, suggesting that antigen presentation was not generally blocked. Nevertheless, T cell function during B cell depletion is another important avenue to explore.
B lymphocyte depletion in this group of patients has proved to be an effective and safe treatment for RA. Major improvement occurred in most cases and in some persisted well after B lymphocyte repopulation. Work now needs to be done to establish the precise mechanism of action of B cell depletion in RA and how its potential may be increased (optimal rituximab dosage and dosing regimens, combination treatment with cyclophosphamide, steroids or other drugs). Armed with this information, the original aim of long term remission may yet be fulfilled. A phase II clinical trial is in progress.