Article Text

Abstract
Objective To compare the prevalence of left ventricular (LV) diastolic dysfunction in subjects with and without rheumatoid arthritis (RA), among those with no history of heart failure (HF), and to determine risk factors for diastolic dysfunction in RA.
Methods A cross-sectional, community-based study comparing cohorts of adults with and without RA and without a history of HF was carried out. Standard two-dimensional/Doppler echocardiography was performed in all participants. Diastolic dysfunction was defined as impaired relaxation (with or without increased filling pressures) or advanced reduction in compliance or reversible or fixed restrictive filling.
Results The study included 244 subjects with RA and 1448 non-RA subjects. Mean age was 60.5 years in the RA cohort (71% female) and 64.9 years (50% female) in the non-RA cohort. The vast majority (>98%) of both cohorts had preserved ejection fraction (EF≥50%). Diastolic dysfunction was more common in subjects with RA at 31% compared with 26% (age and sex adjusted) in non-RA subjects (OR=1.6; 95% CI 1.2 to 2.4). Patients with RA had significantly lower LV mass, higher pulmonary arterial pressure and higher left atrial volume index than non-RA subjects. RA duration and interleukin 6 (IL-6) level were independently associated with diastolic dysfunction in RA even after adjustment for cardiovascular risk factors.
Conclusion Subjects with RA have a higher prevalence of diastolic dysfunction than those without RA. RA duration and IL-6 are independently associated with diastolic dysfunction, suggesting the impact of chronic autoimmune inflammation on myocardial function in RA. Clinical implications of these findings require further investigation.
Statistics from Altmetric.com
Introduction
We have previously shown that patients with rheumatoid arthritis (RA) have about a twofold increased risk of heart failure (HF) and mortality, which is not explained by traditional cardiovascular (CV) risk factors and/or clinical ischaemic heart disease (IHD).1,–,3 We have also recently shown that subjects with RA with HF have fewer typical signs and symptoms of HF and are more likely to have a preserved ejection fraction (EF ≥50%) than non-RA subjects with HF.4 The reasons for this are poorly understood, but these observations suggest there may be inherent differences in ventricular function, particularly diastolic, in people with RA compared with people without RA. The important questions are whether these differences in ventricular function may be evident in patients with RA even before symptoms of HF develop clinically and whether there are RA-specific determinants for these changes.
Isolated diastolic dysfunction occurs frequently without clinically recognised HF,5 and may be one mechanism for the excess development of HF in patients with RA. In previous population-based studies, isolated diastolic dysfunction was common and was associated with a marked increase in all-cause mortality in the general population, underlining the importance of this disease entity.5 6 Previous studies have shown that patients with RA without clinically evident CV disease have a higher prevalence of left ventricular (LV) diastolic dysfunction than controls without RA.7,–,16 However, these studies recruited highly selected patients from hospitals or academic centres rather than from community populations, and most included fewer than 60 consecutive patients with RA. Thus, information from population-based studies is lacking and the mechanisms underlying the development of diastolic dysfunction in RA remain unclear.
The purpose of this study was to compare the prevalence of LV diastolic dysfunction in subjects with RA, without a history of HF, with non-RA subjects without HF in a community-based population and to determine risk factors associated with diastolic dysfunction in RA.
Subjects and methods
Study subjects and design
Using the resources of the Rochester Epidemiology Project,17 a population-based medical records linkage system that allows access to complete medical records from all community medical providers, we conducted a population-based study of residents of Olmsted County, Minnesota aged ≥18 years who first fulfilled 1987 American College of Rheumatology classification criteria for RA between 1 January 1980 and 31 December 2005.18 From this RA incidence cohort,19 we identified eligible subjects with RA, alive and living in Olmsted County without a history of HF (based on Framingham criteria20). We recruited 244 (61%) of the 397 eligible subjects with RA.
We performed a cross-sectional study comparing these subjects with RA with subjects drawn from the same underlying community without either RA or a history of HF. The latter subjects, referred to as the non-RA cohort, were part of a population-based study examining the burden of ventricular dysfunction in the community.5 This previous study recruited patients from a random sample of Olmsted County residents aged ≥45 years in 1997. Study participants returned for a second study visit in the years 2001–4. These data were used for comparison with our patients with RA. All subjects had undergone echocardiography according to previously defined protocols. The institutional review boards of the Mayo Clinic and Olmsted Medical Center approved this study.
Data collection
Data collection for subjects in both the RA and non-RA cohorts was identical except that subjects with RA were asked additional questions pertaining to their RA disease. Subjects in both cohorts completed a questionnaire, provided a blood sample and underwent echocardiography. The questionnaire included identical questions pertaining to HF symptoms, CV risk factors and drug usage. Demographic characteristics were recorded. Presence of the following traditional CV risk factors was ascertained: smoking (current or former); diabetes mellitus (based on a doctor's diagnosis and/or documented use of insulin and/or oral hypoglycaemic agents); hyperlipidaemia (based on clinically obtained elevated fasting lipid values of total cholesterol ≥240 mg/dl, low-density cholesterol ≥160 mg/dl, triglycerides ≥200 mg/dl or high-density cholesterol <40 mg/dl and/or documented use of lipid-lowering agents); body mass index (BMI, kg/m2) and hypertension (based on a doctor's diagnosis and/or documented use of antihypertensive drugs). Data on history of IHD (presence of angina pectoris, coronary artery disease, myocardial infarction (including silent events)) and coronary revascularisation procedures (ie, coronary artery bypass graft, percutaneous angioplasty, insertion of stents and atherectomy) were also gathered.
For subjects in the RA cohort, rheumatoid factor (RF), anti-cyclic citrullinated peptide (anti-CCP), C-reactive protein (CRP), tumour necrosis factor α (TNFα) and interleukin 6 (IL-6) levels were measured in the provided blood sample. RF testing was performed by nephelometry (latex enhanced assay; Behring Nephelometer II; Dade Behring, Newark, Delaware, USA). Anti-CCP testing was performed by enzyme immunoassay from INOVA Diagnostics (San Diego, California, USA). IL-6 and TNFα tests were performed by enzyme immunoassay from R&D Systems (Minneapolis, Minnesota, USA). CRP testing was performed by immunoturbidimetric assay (Roche CRPLX reagent; Roche Diagnostics, Indianapolis, Indiana, USA). Medical records were reviewed to collect data on RA disease characteristics. The questionnaire was augmented to obtain the Health Assessment Questionnaire (HAQ) disability score and RA drug usage at the time of the echocardiography visit, including systemic cortico-steroids, disease-modifying antirheumatic drugs (DMARDs), biological agents and non-steroidal anti-inflammatory drugs (NSAIDs). Systemic corticosteroid use included either oral or intravenous forms (eg, prednisone, methylprednisolone, hydrocortisone and/or dexamethasone); DMARDs included methotrexate, hydroxychloroquine, sulfasalazine, leflunomide and/or azathioprine; and biological agents included TNFα blockers, anakinra, abatacept and/or rituximab. RA drug usage at the echocardiography visit was verified with patients' pill bottles and by reviewing the most recent medication list in the medical record for discrepancies.
Two-dimensional and Doppler echocardiograms were performed on all subjects in the RA cohort following identical protocols to those used in the non-RA cohort, as previously described.5 All echocardiograms were performed by registered diagnostic cardiac sonographers and interpreted in the Mayo Clinic Echocardiographic Laboratory (by BLK and DDB). The following echocardiographic parameters were measured and/or estimated in each subject: pulmonary arterial pressure, left atrial volume index, LV mass, LV mass index, tricuspid regurgitant jet velocity, pulsed-wave Doppler examination of mitral inflow peak early filling velocity (E) and velocity at atrial contraction (A) (before and during Valsalva manoeuvre) and of pulmonary venous inflow; as well as Doppler tissue imaging of the mitral annulus, E/A ratio, E/E′ ratio and deceleration time.
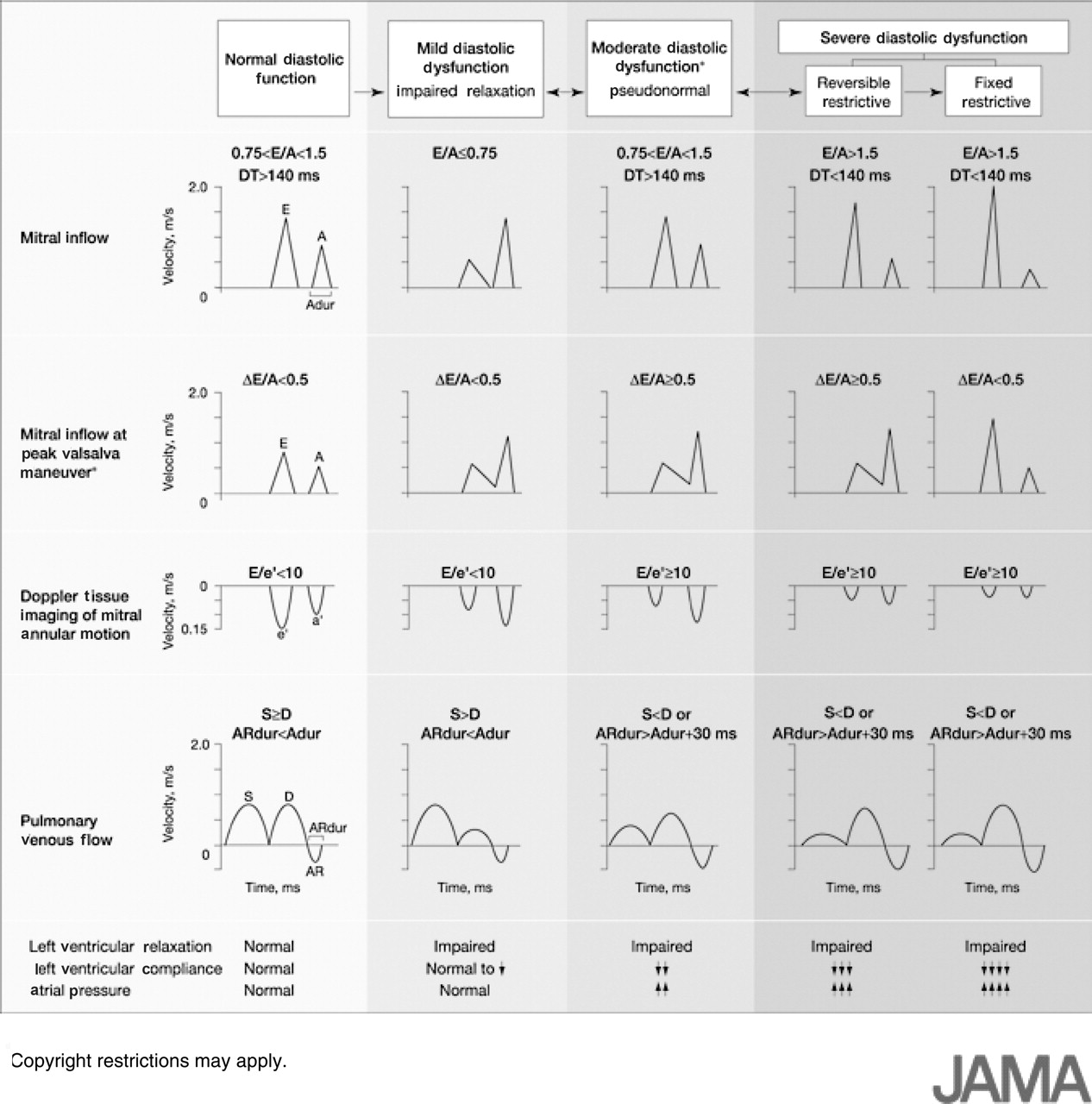
Diastolic dysfunction was categorised as none (normal diastolic function); mild, defined as impaired relaxation without evidence of increased filling pressures; moderate, defined as impaired relaxation associated with moderate elevation of filling pressures or pseudonormal filling; and severe, defined as advanced reduction in compliance or reversible or fixed restrictive filling (figure 1).5 Diastolic function was classified as indeterminate when these criteria could not be fully assessed, such as in cases of dysrhythmias. Subjects were classified into four mutually exclusive categories of normal diastolic function; mild diastolic dysfunction; moderate to severe diastolic dysfunction; or indeterminate diastolic function.
{kind=link}
Doppler criteria for classification of diastolic function. A, velocity at atrial contraction; E, mitral inflow peak early filling velocity. (Adapted with permission from Redfield MM, et al5). Copyright (2003) American Medical Association. All rights reserved.
Statistical methods
Descriptive statistics were used to summarise the demographics, CV risk factors and echocardiographic features for both cohorts, as well as the RA disease characteristics for the RA cohort. Descriptive statistics in the non-RA cohort were adjusted to the age and sex distribution of the RA cohort to allow for visual comparison. This adjustment was performed by weighting the non-RA data according to the proportions of patients with RA in each sex and decade of age. This technique is often used to perform direct standardisation to allow comparison of rates in epidemiology studies. Differences between the two cohorts were tested using linear and logistic regression models adjusted for age and sex. Logistic regression models were also used to examine factors associated with the presence of any diastolic dysfunction. Secondary analyses were performed using matched cohorts. In these analyses, each subject with RA was matched to a non-RA subject of similar age (±1 year), sex and CV risk factors (smoking status, presence of hypertension (defined as systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg), BMI (±2 kg/m2) and presence of diabetes mellitus). Conditional logistic regression was used to examine the association between diastolic dysfunction and RA/non-RA status in the matched cohorts.
Results
The study population included 244 subjects with RA and 1448 subjects without RA. Subjects with clinically diagnosed HF were excluded from both cohorts. Baseline characteristics for both cohorts are reported in table 1. Patients with RA were somewhat younger than non-RA subjects. A higher proportion of subjects with RA were female. The proportion of ever smokers, but not current smokers, was higher in RA than in non-RA subjects. Patients with RA were more likely to have a history of hypertension. Blood pressure at the time of the echocardiographic study in both patients with RA and non-RA subjects was within the normal range, although patients with RA had somewhat higher measures of systolic and diastolic blood pressure than non-RA subjects (table 1). There were no significant differences in diabetes mellitus, hyperlipidaemia, BMI or history of IHD in the two cohorts.
Cardiovascular (CV) risk factors in patients with RA and non-RA subjects
The vast majority (98%) of both cohorts had preserved EF (≥50%), and the proportions with preserved EF in the two cohorts were similar (table 2). However, diastolic dysfunction of any severity was significantly more common in the patients with RA at 31% versus 26% in non-RA subjects (OR=1.6; 95% CI 1.2 to 2.4; p=0.006).
Echocardiographic measurements in patients with RA and non-RA subjects
Age, sex, blood pressure and BMI were significantly associated with diastolic dysfunction overall, and a history of IHD approached statistical significance (p=0.06) (data not shown). There were no significant interactions between these variables and RA/non-RA status. After adjustment for age, sex, blood pressure, BMI and history of IHD, patients with RA were still more likely to have diastolic dysfunction than non-RA subjects (OR=1.4; 95% CI 0.9 to 2.0). However, adjusting for these risk factors somewhat attenuated the risk of diastolic dysfunction in RA and the association was not statistically significant. This association remained unchanged when blood pressure was removed from the list of adjustors.
A secondary analysis was performed to deal with the concern of higher prevalence of some traditional CV risk factors in RA versus non-RA subjects, in which RA and non-RA subjects were matched for age, sex, smoking status, BMI, presence of hypertension and presence of diabetes mellitus. Diastolic dysfunction was still more common in subjects with RA than in non-RA subjects (OR=1.6; 95% CI 0.9 to 2.7). However, this association did not reach statistical significance.
Our finding of increased prevalence of diastolic dysfunction in subjects with RA was further supported by other echo findings (table 2). Patients with RA had a higher pulmonary arterial pressure and higher left atrial volume index than non-RA subjects (table 2). The proportion of subjects with a high left atrium volume index (>28 ml/m2) was also significantly higher in the patients with RA than in the non-RA cohort. The tricuspid regurgitant jet velocity and E/A ratio were both significantly higher in the RA than non-RA subjects, consistent with increased filling pressures seen in diastolic dysfunction (table 2). The mean LV mass index was lower in subjects with RA than in non-RA subjects (p=0.001).
We further investigated the impact of RA characteristics on myocardial function. Disease characteristics of subjects with RA are summarised in table 3. Median disease duration was 8.2 years, with 71% seropositive for RF and 45% seropositive for CCP. About one half of subjects with RA had erosive disease on radiography. At the time of the echocardiography visit 54% of subjects with RA used methotrexate, 27% used hydroxychloroquine and 10% of patients used other DMARDs. About one-third of patients with RA were treated with corticosteroids, 63% used NSAIDs and 16% were receiving treatment with biological agents.
Disease characteristics of patients with RA and association with diastolic dysfunction
RA duration and IL-6 level were significantly associated with diastolic dysfunction (OR=3.2; 95% CI 1.8 to 5.4 and OR=1.2 per 2.8 pg/ml; 95% CI 1.02 to 1.4, respectively), even after adjustment for CV risk factors (table 3). There was no apparent association between TNFα level and LV diastolic dysfunction (OR=1.0 per 2.2 pg/ml; 95% CI 0.98 to 1.01). Methotrexate use was significantly associated with diastolic dysfunction (OR=2.1; 95% CI 1.01 to 4.2). Use of other DMARDs was associated with 1.9-fold increased risk of LV diastolic dysfunction; however, this association did not reach statistical significance (OR=1.9; 95% CI 0.6 to 5.6). After adjustment for CV risk factors, patients treated with methotrexate and other DMARDs were still more likely to have diastolic dysfunction (OR=1.8; 95% CI 0.9 to 3.8 and OR=2.0; 95% CI 0.6 to 6.5, respectively), although these associations did not reach statistical significance (table 3).
To examine the possibility of confounding by indication in methotrexate users, we performed additional analyses adjusting for RA characteristics (RF positivity, CRP and IL-6). After this additional adjustment, the association between methotrexate and diastolic dysfunction was somewhat attenuated and was no longer statistically significant (OR=1.7; 95% CI 0.7 to 3.8; p=0.21). Furthermore, there was no association between duration of methotrexate use and diastolic dysfunction. We did not find statistically significant associations of diastolic dysfunction with other RA characteristics (namely, RF and CCP positivity, CRP level, erosive changes and HAQ score) or with drugs (including biological agents, corticosteroids and NSAIDs) (table 3).
Discussion
Herein, we report the first large, population-based echocardiographic investigation of myocardial function among subjects with RA compared with non-RA subjects without a history of HF from the same community. We have shown that patients with RA have a higher prevalence of diastolic dysfunction (31%) than non-RA subjects (26%) based on currently accepted diagnostic criteria. Diastolic dysfunction was more common in RA than in the non-RA subjects even after adjustment for, or matching for, CV risk factors, although the associations were marginally significant. We have also found that diastolic dysfunction in RA is associated with RA duration and IL-6 level, even after adjustment for CV risk factors. Notably, the vast majority of subjects had preserved EF. The presence of diastolic dysfunction with preserved EF, or isolated diastolic dysfunction, has been previously associated with a marked increase in mortality in the general population.5 6 Hence, the increased prevalence of isolated diastolic dysfunction in RA may have implications on excess mortality in patients with RA.
Other echocardiographic findings supportive of the increased prevalence of diastolic dysfunction in subjects with RA included higher pulmonary arterial pressure and left atrial volume index in the RA cohort compared with the non-RA cohort. Pulmonary arterial hypertension has been reported to be more prevalent among patients with RA than among controls.21 22 While this finding resonates with the higher prevalence of any diastolic dysfunction in RA compared with non-RA subjects, we cannot exclude the possibility that higher pulmonary arterial pressures were due to pulmonary abnormalities such as interstitial lung disease in the RA cohort. However, a larger left atrial volume index would not be expected from interstitial lung disease alone.
Previous studies have reported an association between RA and features of impaired diastolic ventricular function, as reviewed by Giles et al.23 Using Doppler determination of transmitral flow velocity, alterations of the E/A ratio have been demonstrated for patients with RA compared with controls in several studies.14 16 17 –,27 Left atrial size and left atrial volume have been noted to be increased among patients with RA. Increased LV diameter, increased LV mass and LV hypertrophy16 have been reported and were independently associated with RA.28 However, similar to our findings, some other authors found a lower LV mass index in patients with RA than in non-RA subjects, as measured by cardiac MRI.29 Despite the differences in the direction of changes of LV mass in different studies these findings are not necessarily contradictory. There is a possibility of sequential changes in LV mass in RA from myocardial hypertrophy to myocardial wasting (ie, myocardial remodelling). It is notable that subjects with RA in the study reporting high LV mass were somewhat younger (mean age 46.7 years) than subjects with RA in either our study (mean age 60.5 years) or the Giles study (mean age 59 years), both reporting low LV mass.28 29
Concurrent with several earlier studies,24,–,26 the duration of RA disease in our study was strongly associated with diastolic dysfunction, even after adjustment for traditional CV risk factors. This may reflect a chronic subclinical myocardial process leading to impairment of myocardial function as previously hypothesised.12 Concordant with this hypothesis, a number of studies suggested a strong relationship between RA characteristics, including extra-articular RA and diastolic dysfunction.8 9 24 30 The association of diastolic dysfunction with IL-6 in our study further emphasises the impact of immune dysregulation on myocardial abnormalities in RA. IL-6 was previously found to correlate closely with LV systolic and diastolic dysfunction in the general population.31 Our data suggest that this cytokine may also be implicated in diastolic dysfunction in RA.
Antirheumatic drugs did not appear to have a major impact on diastolic dysfunction in our study. Confounding by indication or contraindication might account for the increased likelihood of LV dysfunction in methotrexate users. For example, given concerns about HF with the use of TNFα blockers, patients at high risk of HF may be preferentially treated with methotrexate, rather than TNFα blockers. While some evidence from recent studies suggests that TNFα blockers may confer beneficial effect with regard to the risk of HF,32 studies on the changes of diastolic function with TNFα blockade are lacking. In our study there was no apparent association of biological agents with the risk of LV diastolic dysfunction. The reasons for this are uncertain, and the impact of antirheumatic drugs on diastolic dysfunction requires further investigation.
Our study has several potential limitations. First, the nature of a cross-sectional study limits the types of conclusions that can be drawn, as these observations are associations and not necessarily causal. Second, over 90% of the population of Olmsted County is white, and the generalisability of our findings to populations with different race/ethnicity may be limited. In addition, we could not fully exclude the possibility of participation bias, as subjects in both cohorts had to agree to filling out questionnaires and receiving echocardiography. Finally, the higher proportion of subjects with a history of hypertension in the RA versus non-RA cohorts might be expected to affect the diastolic dysfunction measurements unfavourably. However, this seems unlikely as blood pressures at the time of the study in both cohorts were within the normal range, suggesting that hypertension was well controlled. Further, adjustment for blood pressure did not affect the likelihood of LV diastolic dysfunction in RA, suggesting that other factors including RA-related factors may affect myocardial function.
Our study also has several strengths. It is the first large community population-based study of subjects without a history of HF, comparing the prevalence of diastolic dysfunction in patients with RA and non-RA subjects and determining risk factors for diastolic dysfunction in RA. Because it was a large population-based study, the RA cohort was representative of those patients meeting American College of Rheumatology classification criteria for RA in a defined community population. By using the comprehensive medical record linkage system of the Rochester Epidemiology Project, we identified a large number of patients in each cohort, integrated within two large population-based cohorts funded by the National Institutes of Health. Furthermore, our study used a standardised echocardiography protocol with rigorous definitions for mild, moderate and severe diastolic dysfunction.
In conclusion, among subjects without a history of HF, patients with RA have a higher prevalence of diastolic dysfunction than those without RA. Diastolic dysfunction in RA was associated with RA duration and IL-6 level, even after adjustment for CV risk factors. Our findings suggest the role of chronic autoimmune inflammation in development of diastolic dysfunction in RA. The clinical implications of these findings, particularly the impact of diastolic dysfunction on the excess risk of HF and mortality in RA, require further investigation.
References
Footnotes
-
Funding This work was funded by grants from the National Institutes of Health (NIH), National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) (R01 AR46849) and National Heart, Lung and Blood Institute (R01 HL 55502) and made possible by a grant from the NIH, NIAMS (AR-30582).
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Mayo Clinic and Olmsted Medical Center Institutional Review Boards.