Article Text

Abstract
Objective To evaluate the responsiveness of joint counts, patient-reported measures and proposed composite scores in hand osteoarthritis (HOA).
Methods Data were used from a previously reported study in which 83 patients with HOA were randomly assigned to CRx-102 or placebo. CRx-102 consists of prednisolone (3 mg/day) and dipyridamole (400 mg/day), and was shown to be superior to placebo. Assessments were performed at baseline and after 7, 14, 28 and 42 days, and included the Australian/Canadian osteoarthritis hand index (AUSCAN), visual analogue pain subscale (VAS) pain and patient global, and counts of distal interphalangeal (DIP), proximal interphalangeal (PIP), metacarpophalangeal and carpometacarpal (CMC) joints (tenderness, soft tissue swelling, bony enlargement, limited motion). Various combinations of patient-reported outcomes and joint counts were computed as composite scores (similar to clinical disease activity index) and tested for responsiveness. For each measure, mean change from baseline to day 42, treatment effect, standardised response mean (SRM) and relative efficiency compared with AUSCAN pain were calculated.
Results The SRM were largest for VAS patient global (0.92), VAS pain (0.77) and AUSCAN pain (0.68), whereas the responsiveness of tender (0.46) and swollen joint counts (0.51) (18 joint assessment of DIP, PIP, CMC) was similar to AUSCAN stiffness (0.53) and physical function (0.37). Composite scores showed similar responsiveness as patient-reported pain and global.
Conclusion Patient-reported pain and patient global assessment were the most responsive outcomes, whereas joint counts had similar responsiveness to patient-reported stiffness and physical function. Composite scores were as responsive as VAS pain, and these results encourage further elaboration and validation of composite scores in HOA in larger studies.
Statistics from Altmetric.com
Osteoarthritis is the most prevalent rheumatic joint disease. The hand joints are frequently involved, and radiographic hand osteoarthritis (HOA) has been found in 67% of women and 55% of men above 55 years of age.1 HOA leads to pain, stiffness, deformity and gradually loss of function, with major impact on health-related quality of life.2 With a growing older population, osteoarthritis will become an increasingly important health issue, and the World Health Organization has already defined osteoarthritis as one of the major global health problems.3
Outcome assessments in clinical trials as well as clinical practice require the use of feasible, valid, reliable and responsive instruments that adequately address the most important aspects of the disease. In rheumatoid arthritis (RA), a variety of standardised outcome measurements, both individual measures and composite scores including joint counts as well as patient-reported outcomes, are available.4,–,10
The Outcome Measures in Rheumatoid Clinical Trial (OMERACT) initiative and the Osteoarthritis Research Society (OARSI) issued recommendations about the use of outcome measures in clinical trials in osteoarthritis in 1996.11 12 These recommendations included a core set of three clinical domains (pain, physical function and the patient's global assessment) and additionally joint imaging for studies with follow-up for 1 year or longer. The conduct of osteoarthritis clinical trials was further improved by the definition of clinical responder criteria.13 14 Initially, the OMERACT–OARSI initiatives were focused on outcome measures in hip and knee osteoarthritis, but in 2000 the OARSI established a separate task force to develop guidelines specific for HOA.15 The research in HOA was further facilitated by the establishment of an international group, Disease Characteristics in Hand Osteoarthritis (DICHOA), in 2005. Given the limited knowledge and research in HOA, the DICHOA has ascertained that more data are needed to examine the clinimetric performance of various outcome measures that capture pain and inflammatory and physical dimensions of this disease.16
Responsiveness is a particularly important aspect of candidate outcome measures for clinical trials on treatment effect. However, lack of effective treatment has limited the opportunity to examine the responsiveness of outcome measures in HOA. Joint involvement reflects the inflammatory and destructive processes of the disease, and may potentially be a responsive measure in HOA, as they are in RA. A recent study showed that counts of finger joints with tenderness/pain were moderately correlated with other disease-specific outcome measures and grip strength.17 The aim of this study was to examine the responsiveness of patient-reported measures, various combinations of joint counts and proposed composite scores in a setting of a randomised placebo-controlled clinical trial (RCT), which demonstrated that CRx-102, a combination of prednisolone and dipyridamole, was superior to placebo.18
Patients and methods
Study population, design and medication
Details of the study population, design and medication have been presented in a previous paper.18 In short, 83 patients (77 women and six men) between 43 and 71 years of age with HOA according to the American College of Rheumatology criteria19 (intention to treat (ITT) population) were enrolled in this single-blinded 6-week placebo-controlled study. Additional eligibility criteria included radiographic HOA (Kellgren–Lawrence score ≧2),20 the presence of more than one swollen and more than one tender joint, and self-reported hand pain of at least 30 mm on the Australian/Canadian osteoarthritis hand index (AUSCAN) visual analogue pain subscale (VAS). After a screening visit, the patients were randomly assigned 1:1 to the CRx-102 or the placebo group. The CRx-102 patients received daily doses of 3 mg prednisolone and 200 mg dipyridamole for days 1–7, and 3 mg prednisolone and 400 mg dipyridamole for days 8–42. Patients in the placebo group received an equal number of placebo tablets at the same time points. Follow-up assessments with regard to efficacy were performed after 7, 14, 28 and 42 days.
Assessments
The AUSCAN index was used as the primary assessment instrument.21,–,23 AUSCAN has five items measuring pain, one item measuring stiffness and nine items measuring physical function. The pain and physical function scores were normalised to a 0–100 point scale before the analyses.18 Additional patient-reported outcomes included VAS joint pain (question: How would you describe the intensity of your joint pain during the last 2 days¿) and VAS global assessment (question: We ask you to evaluate the activity of your osteoarthritis over the last 2 days. When you take all symptoms into consideration, how will you evaluate your condition¿). The patients did not have access to previous scores in subsequent assessment visits.
Each of the distal interphalangeal (DIP) joints, proximal interphalangeal (PIP) joints, first interphalangeal joint, metacarpophalangeal joints and first carpometacarpal (CMC-1) joint on both hands were assessed for the presence of tenderness/pain on motion, soft tissue swelling, bony enlargement and limited motion. The joint assessments were performed by a rheumatologist, and usually by the same assessor at each visit. Joint counts were computed for each of the four manifestations (tender joint count, TJC; soft tissue swelling joint count, SJC; bony enlargement joint count, BEJC; limited motion joint count, LMJC) for the DIP joints (range 0–8), PIP joints (range 0–8), CMC joints (range 0–2) and for the DIP, PIP and CMC joints combined (range 0–18). The metacarpophalangeal joints were not included in the combined joint count because of infrequent involvement. The first interphalangeal joints were also excluded from the combined joint count because of no treatment effect for all four joint characteristics.
Sera were analysed to determine levels of C-reactive protein (CRP) at each visit.
Composite scores
We used the concepts of the patient activity score (PAS)9 and the clinical disease activity index (CDAI)8 in RA for the proposal of different composite scores in HOA. The patient-reported outcomes were normalised to a 0–10 scale, whereas the joint counts were based on an 18-joint assessment (DIP 2–5, PIP 2–5 and CMC-1 bilateral). As in the CDAI, only TJC and SJC were included as other joint counts were not responsive. The HOA–PAS score was calculated as the average of VAS pain, VAS global and AUSCAN physical function (range 0–10), while the HOA–CDAI scores were calculated as the simple summation of TJC (range 0–18), SJC (range 0–18) and combinations of VAS and AUSCAN scores as specified in table 1 (range 0–10 for each patient-reported outcome; total range 0–56 or 0–66).
Mean (SD) baseline values, LS mean (SD) changes from baseline adjusted for baseline value (analysis of covariance), treatment effect, SRM and relative efficiency compared to AUSCAN pain in the per-protocol population (score range is shown in parentheses)
Analyses
The statistical analyses were selected by the lead author (IKH) and performed by the study sponsor. The analyses of comparative responsiveness were conducted on the per-protocol (PP) population (59 patients), which was defined as all subjects who received at least one dose of study medication, had no major protocol violations and had a study drug compliance of at least 75%.
For each outcome measure, we calculated the mean change from baseline to day 42 adjusted for baseline value (analysis of covariance; least-squares (LS) mean) in the CRx-102 group and the placebo group. The last non-missing observation was carried forward to replace subsequent missing value in one patient. For each study outcome, the ability to detect treatment differences between the groups was evaluated using three measures:24 25 (1) Treatment effect (the difference between the adjusted mean change from baseline value in the CRx-102 group and the placebo group); (2) standardised response mean (SRM; the ratio of the treatment effect to the pooled SD of the adjusted mean change scores) (see supplemental file 2, available online only); (3) relative efficiency in relation to the AUSCAN pain score (the square of the SRM value for the various outcomes compared with the square of the AUSCAN pain score). SRM values above 0.20, 0.50 and 0.80 represent small, moderate and large responsiveness, respectively, and a relative efficiency greater than 1 implies that the outcome is more efficient than the AUSCAN pain score in detecting a treatment effect.
Results
The PP population consisted of 53 women and six men with a mean (SD) age of 59.9 (5.1) years, weight 72.4 (12.7) kg and height 166.4 (8.2) cm, without significant differences between treatment groups or compared with the total ITT population. Details about patient characteristics in the ITT population have been published in a previous paper.18 Baseline levels of pain, physical limitations and involvement of hand joints were similar in the two treatment groups, and adjusted mean changes from baseline (LS mean) were generally largest in the CRx-102 group (table 1).
The treatment effect was statistically significant for VAS pain, VAS global, AUSCAN pain and stiffness, whereas it was non-significant for AUSCAN physical function and CRP (table 1). With the exception of BEJC (negative treatment effect), the changes in joint counts from baseline were generally larger in the CRx-102 group compared with the placebo group, but the treatment effect was mostly non-significant (table 1).
The SRM values were largest for VAS patient global (0.92), VAS pain (0.77) and AUSCAN pain (0.68). Responsiveness of 18-TJC (0.46) and 18-SJC (0.51) was similar to AUSCAN stiffness (0.53) and physical function (0.37). Both separate joint counts and combined tender and swollen joint counts were responsive measures (table 1 and supplemental table 1, available online only). As expected, BEJC and LMJC were not responsive (table 1).
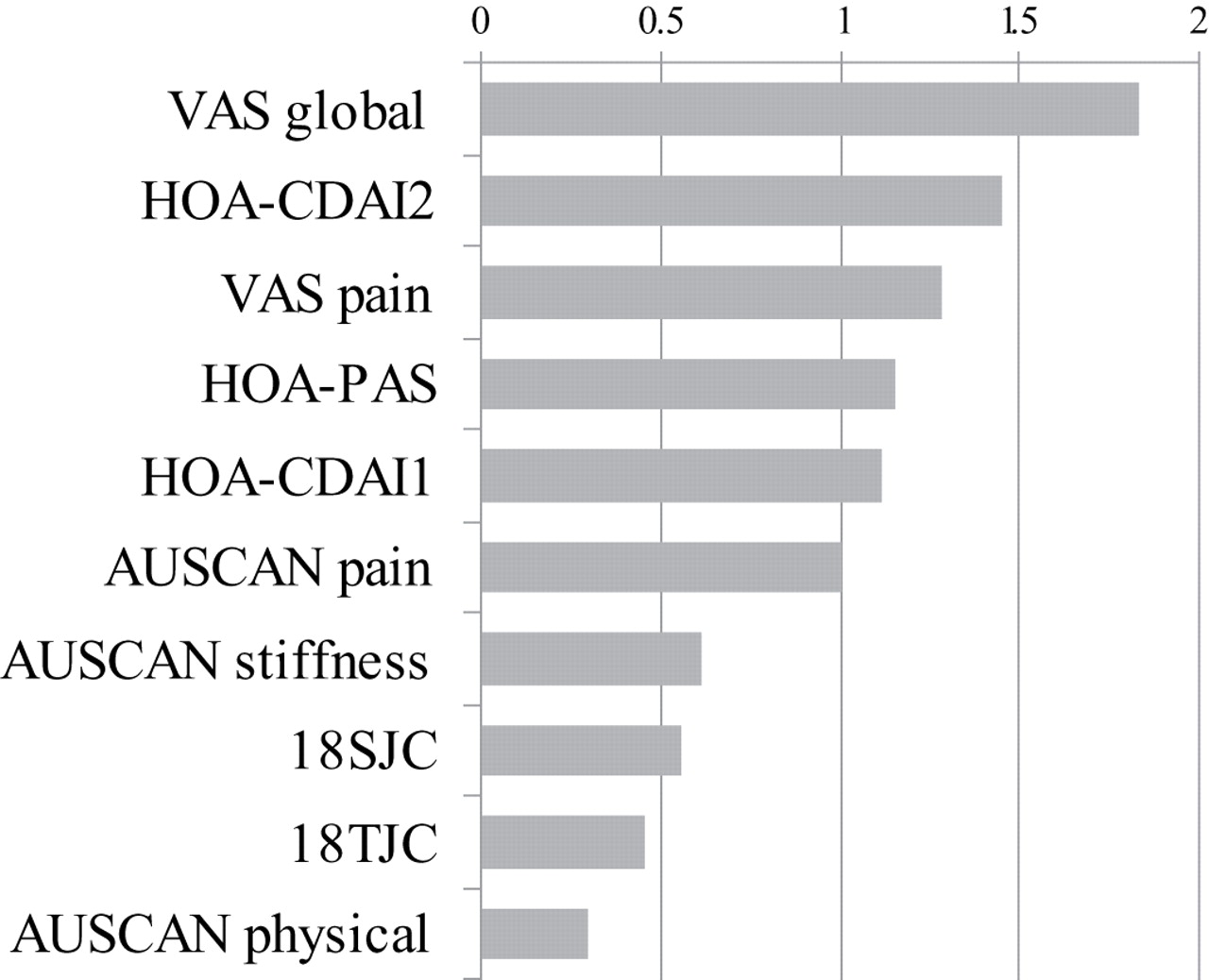
AUSCAN pain was the predefined endpoint in the calculation of the relative efficiency. VAS patient global (1.83) and VAS pain (1.28) were more efficient than AUSCAN pain in detecting a treatment effect. The relative efficiency for AUSCAN stiffness (0.61) was slightly superior to 18-TJC (0.46) and 18-SJC (0.56), which were superior to AUSCAN physical function (0.30) (table 1). The relative efficiency in decreasing order of magnitude is shown in figure 1.
{kind=link}
Relative efficiency of various outcome measures in relation to Australian/Canadian osteoarthritis hand index (AUSCAN) pain score in the per-protocol population. HOA–CDAI, hand osteoarthritis clinical disease activity index; HOA–PAS, hand osteoarthritis patient activity score; SJC, soft tissue swelling joint count; TJC, tender joint count; VAS, visual analogue scale.
The composite scores were responsive measures with significant treatment effect and SRM values similar to the VAS scores and AUSCAN pain (table 1). The relative efficiency in detecting a treatment effect was superior to AUSCAN pain for all composite scores. The most efficient composite measure in detecting change was the HOA–CDAI-2, which included 18-TJC, 18-SJC, VAS pain and VAS global (relative efficiency 1.45). The responsiveness of HOA–PAS including VAS pain, global and AUSCAN physical function was similar to HOA–CDAI-1 including joint counts and AUSCAN scores, with a relative efficiency of 1.15 and 1.12, respectively (table 1 and figure 1).
Discussion
These analyses demonstrated that patient-reported outcomes such as VAS global, VAS pain and AUSCAN pain were the most responsive single outcome measures in HOA patients receiving anti-inflammatory treatment. The responsiveness of tender and swollen joint counts was similar to AUSCAN stiffness and superior to AUSCAN physical function, and the new HOA–CDAI and HOA–PAS composite indices showed responsiveness similar to VAS pain.
Quantitative documentation of clinical outcomes is essential for the evaluation of disease progression and treatment effect, and we used the same methodological approach as Wells et al24 when we compared different outcome measures with regard to responsiveness. AUSCAN pain was predefined as the primary outcome measure in the RCT,18 and was therefore chosen as the reference when we computed the relative efficiency of the other measures in detecting a treatment effect. The clinimetric properties of the AUSCAN index has been validated in separate studies.22 26 27
Several other instruments for the assessment of patient-reported outcomes in HOA have been developed over the past few years, including the score for assessment and quantification of chronic rheumatic affections of the hands (SACRAH),28 the functional index in hand osteoarthritis (FIHOA)29 30 and the Cochin index.31 32 However, for feasibility reasons we chose not to include other available hand indices, and the responsiveness of these instruments in the condition of HOA needs to be compared.
In this study the responsiveness of VAS pain and VAS patient global were superior to all AUSCAN subscales, and these results encourage the use of VAS items in clinical practice, with the benefit of being easy to perform and free of charge.
Currently used single parameters or indices may not satisfactorily reflect the disease activity because they only cover part of the disease. The benefit of appropriate composite scores is the ability to capture multiple important aspects of disease activity into a single numerical value, which might increase the face and construct validity and sensitivity to change. Over the past few years, several composite scores have been developed for use in other rheumatic diseases, especially in RA, including the disease activity score in 28 joints (DAS28),6 the simplified disease activity index (SDAI)7 and the clinical disease activity index (CDAI).8 The SDAI and CDAI were developed to provide physicians with simple, sensitive and validated tools for clinical assessment of RA in daily practice. The SDAI is the numerical sum of five outcome parameters: tender and swollen joint count (28-joint assessment), patient and physician global assessment of disease activity (VAS 0–10 cm) and level of CRP (mg/dl). The CDAI is similar to the SDAI, but does not incorporate CRP. The PAS9 is based on patient-reported outcomes and is calculated as the average of VAS pain, VAS global and the health assessment questionnaire after normalisation of each domain on a 0–10 scale. Similar disease-specific composite measures do not currently exist in osteoarthritis.
This study showed that joints with tenderness and soft tissue swelling were numerically improved in the CRx-102 group compared with the placebo group, and both combined and separate counts of swollen and tender DIP, PIP and CMC joints were responsive measures (table 1 and supplemental table 1, available online only). This observation encouraged us to include counts of joints with tenderness and soft tissue swelling in composite scores in HOA, as in RA. An optimal collection of domains and item weight in composite scores requires complex statistical procedures as used in the development of the disease activity score and ankylosing spondylitis disease activity index (ASDAS). As the first study in this field in HOA, this was not our approach. The calculations of our composite scores were based on the analyses of responsiveness of single outcome components, including both patient-reported measures and joint counts, and the application of the simplistic concepts of CDAI and SDAI. These concepts are based on a simple summation of the components without any weight for the relative importance. We used CDAI instead of SDAI as a model because CRP was an insensitive marker in this RCT (table 1). The joint count items in our composite scores were based on an 18-joint assessment of tenderness and soft tissue swelling of the DIP, PIP and CMC-1 joints, which are the most frequently affected joints in HOA.
The composite score that was relatively most efficient in the detection of change was the HOA–CDAI-2, which included VAS global and VAS pain in addition to the joint counts. It can be argued that the responsiveness of the HOA–CDAI composite scores was similar to patient-reported pain and inferior to VAS global. Increased responsiveness was thus not achieved when the joint counts were included (table 1 and figure 1). However, similar to RA, composite scores provide information from several relevant aspects of the disease, which is important for face validity. The inclusion of AUSCAN items in the composite scores resulted in decreased responsiveness compared with composite scores with the inclusion of VAS scores. However, HOA–CDAI-1, which included joint counts and all AUSCAN subscales, showed greater responsiveness than all the separate items. The composite score based on patient-reported outcomes, the HOA–PAS, included all OARSI core set domains (pain, global and physical function), but was relatively less effective than HOA–CDAI-2 and similar to HOA–CDAI-1 in the detection of change. This observation was not surprising, because AUSCAN physical function had rather low responsiveness in this study.
A strength of the study was the extensive joint examination with specific assessment of four different features of joint involvement. In addition, this is the first study in HOA presenting composite scores similar to the CDAI and PAS composite scores for RA. However, as this RCT was a preliminary proof-of-concept study, there are limitations to our analyses. First, the number of patients enrolled was originally small, and because of side-effects (including headache and nausea) the drop-out rate was high in the CRx-102 group.18 Missing data were imputed using the last non-missing observation carried forward, which may produce biased results. We therefore chose to use the PP population (only one patient with missing observation) for the responsiveness analyses, but study results have previously been presented from both the PP and ITT populations.18 Second, the duration of treatment in this study was only 42 days, and longer treatment might increase the responsiveness of certain outcomes for which the resolution of inflammation and/or tissue damage is required, as joint counts. Finally, the reproducibility of joint counts and other aspects of the OMERACT filter were not assessed.
In conclusion, we have shown that both individual measures from different domains and composite scores are responsive in HOA. Our results should encourage additional larger studies of longer duration to examine the responsiveness of joint counts and to examine the full clinimetric performance, including feasibility, reliability and validity of various composite scores with combinations of patient-reported outcomes and joint counts.33 In addition, instruments other than AUSCAN and physician-reported outcomes such as VAS global should probably also be included in future studies addressing the performance of composite measures in HOA.
References
Supplementary materials
Web Only Data ard.2008.100156
Files in this Data Supplement:
Footnotes
-
Funding The RCT was funded by CombinatoRx.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Norwegian Ethical Committee Health Region East.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.