Article Text

Abstract
Objective Inflammation at the entheses is a distinguishing feature of spondyloarthritis (SpA). Enthesitis at the heel is the most common location and is often chronic, refractory to standard treatment and may have socioeconomic consequences. The objective of this study was to investigate the efficacy of etanercept in refractory heel enthesitis related to SpA.
Methods The present work was a 12-week, randomised, double-blind, placebo-controlled study compared etanercept with placebo in patients with SpA according to Amor's criteria, and heel enthesitis proven by MRI. The primary efficacy end point was the normalised net incremental area under the curve (AUC) between randomisation and week 12 for the patient's global assessment (PGA) of disease activity. Secondary end points included change from baseline in PGA, heel pain, the Western Ontario and McMaster Universities Osteoarthritis index (WOMAC) function subscale and improvement in enthesitis as measured by MRI.
Results A total of 24 patients were randomised. Mean normalised net incremental AUC for PGA of disease activity over 12 weeks was significantly greater in the etanercept versus placebo group: −28.5 versus −11.1, respectively (p=0.029). Significant improvements were also reported in the etanercept versus placebo group for PGA, −37.6 versus −11.6 (p=0.007); heel pain, −36.7 versus −13.1 (p=0.022); and WOMAC function, −23.2 versus −7.8 (p=0.024). No significant changes were observed in the MRI findings between groups. No unexpected adverse events or changes in laboratory values or vital signs.
Conclusions This trial is the first randomised placebo-controlled study of an anti-tumour necrosis factor (TNF) agent in refractory heel enthesitis in patients with SpA. It demonstrates that etanercept has a statistically significant and clinically relevant benefit in such patients.
ClinicalTrials.gov identifier NCT00420303.
Statistics from Altmetric.com
Introduction
Inflammation at the entheses, the sites of attachment of tendons, ligaments, fascia or joint capsules to bone, is the distinguishing pathological feature of spondyloarthritis (SpA).1,–,5
Enthesiopathy is a frequent manifestation involving mainly the heel at the insertion of the Achilles tendon or fascia plantaris. Entheseal pain may be disabling and resistant to standard antirheumatic treatment.
Evaluation of enthesiopathy is traditionally performed at the patient level with an enthesitis scoring system (eg, the Mandel enthesitis index,6 the Stoke Enthesitis index,7 the University of San Francisco Enthesitis Score,8 the Maastricht Ankylosing Spondylitis Enthesitis Score (MASES)9 or the Berlin Enthesitis Score10).
These scoring systems have been evaluated mainly as secondary objectives or exploratory analyses in clinical trials aimed at evaluating the symptomatic spinal effect of tumour necrosis factor (TNF) blockers.11,–,13 All reported data were in favour of the TNF blockers. However, such scoring systems have been criticised because they are time consuming and have poor interobserver reliability and face validity.
The poor face validity of such scoring system has given rise to the concept of using a scoring system based not on the subjective clinical findings (eg, pain on pressure), but rather on objective evaluation. MRI may be used to screen for inflammatory lesions at different locations in patients with SpA.13 Recent research has suggested that an ultrasound enthesis score could be a valid tool in the diagnosis of SpA.14 Another possible means of assessing enthesiopathy that is more clinically relevant for daily practice is evaluation at a specific location, such as the heel, with use of conventional symptomatic outcome measures such as patient's global assessment (PGA), pain and functional impairment.
In patients with painful disabling enthesiopathy refractory to local treatments (eg, supportive or accommodative ortheses, physiotherapy, local steroid injection2), treatment options are limited. In this condition, TNF blockers might be an option.
Relatively few studies have reported a positive impact of TNF blockers on entheseal inflammation in SpA. For example, a significant improvement in refractory inflammatory heel pain, measured by ultrasonography, was reported following treatment with infliximab, in two patients with human leucocyte antigen (HLA)-B27 positive SpA who had refractory erosive calcaneal enthesitis.15
Etanercept is a recombinant human TNFα soluble receptor fusion protein that antagonises the effects of endogenous TNF by blocking the binding of TNF to cell surface receptors and the initiation of intracellular signalling. Etanercept has demonstrated efficacy in axial and peripheral presentations in patients with SpA and resulted in effective, safe and sustained reduction of the clinical signs and symptoms.16,–,22
Peripheral enthesitis, in particular heel enthesitis, leads to high morbidity and is often resistant to standard antirheumatic treatment. Because a positive impact of TNF blockers on entheseal inflammation in SpA has been reported in only a few anecdotal observations, and because of the potential value of TNF blockers for treating SpA, we aimed to compare the efficacy of etanercept injection, 50 mg once weekly for 12 weeks and placebo in patients with refractory heel enthesitis.
Methods
Study design
This was a 12-week, randomised, double-blind, placebo-controlled, multicentre study (ClinicalTrials.gov identifier: NCT00420303) conducted in 14 centres in 3 European countries (France, Germany and The Netherlands) comparing etanercept 50 mg injection once weekly with placebo (1:1 ratio).
Patients were screened for up to 6 weeks to ensure their eligibility to enter the study, then were randomised to receive either etanercept 50 mg once weekly or matching placebo. Patients were evaluated at screening, baseline, and weeks 2, 4, 8 and 12. A safety follow-up visit, which could be by telephone, was performed 2 weeks after the last dose.
Patients
For inclusion in the study, patients needed to be between 18 and 70 years of age with a current diagnosis of SpA (as defined by Amor's criteria).23 Patients were required to present with heel enthesitis (pain of the posterior and/or inferior part) that was MRI positive according to the local radiologist (bone marrow oedema of the calcaneum adjacent to the insertion site of either Achilles tendon or fascia plantaris; bone marrow oedema was defined as a high signal area on short Tau inversion recovery (STIR)-weighted images). The enthesitis was refractory to standard treatment (defined as non-steroidal anti-inflammatory drugs (NSAIDs) for >3 months at the maximal tolerated dose or appropriate local treatment). PGA of heel enthesiopathy activity (on a 100-mm visual analogue scale (VAS)) had to be >40 mm. All women patients of childbearing potential were required to provide a negative serum pregnancy test at screening.
Patients were excluded from the study if they had been injected with any local steroid injection within 2 weeks of screening, if they had prior exposure to any TNF inhibitor, including etanercept, if their NSAID dose had changed within 2 weeks of baseline evaluation, if their prednisone (or equivalent) dose was >10 mg/day or had changed within 2 weeks prior to baseline evaluation or if their possible disease-modifying antirheumatic drugs had changed within 4 weeks prior to baseline. Patients were also excluded if they had significant concurrent medical disorders, abnormal laboratory test values, or a known contraindication or sensitivity to etanercept or its excipients.
This trial was conducted in accordance with the ethical principles of the Declaration of Helsinki and was consistent with the guidelines for good clinical practice (ICH-E6) and local regulations. All participating patients provided written informed consent. The study protocol and informed consent documents were approved by each institution's review board or independent ethics committee.
Primary end point
The primary efficacy end point was the normalised net incremental area under the curve (AUC) for PGA of heel enthesiopathy activity (measured on a 100-mm VAS) between randomisation and week 12 and calculated as the area between baseline and the PGA curve as a function of time by the linear trapezoidal method. For patients who withdrew from the study, missing values were not replaced; for patients who had intermediate missing values, linear extrapolation was used to replace such values; for patients who did not withdraw from the study but did not complete the last evaluation, the last observation carried forward (LOCF) technique was used.
Secondary end points
Secondary efficacy end points were change from baseline in PGA of heel enthesiopathy activity, heel pain (measured on a 100-mm VAS), Western Ontario and McMaster Universities Osteoarthritis index ((WOMAC) function subscale chosen as a measure of physical function in the lower limbs; 0–100 normalised score, with 100 representing greatest functional impairment),24 the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI),25 and the MASES.8 For all these continuous variables, the missing variables were evaluated using the LOCF technique. Two further end points were evaluated by the patient: the minimum clinically important improvement (MCII) and the patient acceptable symptom state (PASS). The MCII comprises two questions aimed at defining whether the observed difference (less pain) from baseline constitutes a trivial or an important improvement according to the patient. The PASS comprises one question aimed at defining whether the observed changes in health status lead to an PASS according to the patient26; Efficacy was also assessed by the response at week 12, defined as ≥50% improvement (decrease) from baseline in the PGA.
Heel MRI, with coronal STIR-weighted, sagittal STIR-weighted and sagittal T1-weighted images, was planned for each patient in each centre at the screening visit and at week 12 or early discontinuation visit. MRI images were analysed centrally on a workstation by one radiologist who was blinded to study treatment and the chronological order of images. We report here the changes in area (in millimetres) of the calcaneum bone oedema.
Safety and tolerability were evaluated by assessing the incidence and severity of adverse events (AEs), as well as premature withdrawals from the study. Physical examinations were performed at baseline and at weeks 2, 4, 8 and 12, together with monitoring of vital signs and laboratory test values.
Statistical analysis
The planned sample size of 10 patients per group based on previous experience15 was sufficient to show a difference of 30 points between groups in the primary end point, assuming a SD of 20. This sample size was based on a power of 85% and a two-sided error of 5%. The primary end point was analysed by analysis of covariance (ANCOVA) with treatment as a factor and PGA at baseline as a covariate.
A mixed model ANCOVA, with an autoregressive correlation structure with treatment groups, visits and their interaction as fixed factors and baseline as a covariate was also used to analyse changes from baseline in PGA and other continuous secondary efficacy variables. For binary efficacy variables (PGA response, PASS), a generalised estimating equations model, with a logit link, a binomial distribution and an autoregressive correlation structure was used, with treatment groups, visits and their interaction as fixed factors. Kaplan–Meier survival analysis was used to illustrate the time to achieve a sustained PASS as assessed by PASS.
For each ANCOVA, mean change from baseline was calculated, together with corresponding SE, 95% CI and p value. AEs were coded using the Medical Dictionary for Regulatory Activities dictionary. Descriptive statistics were used to assess all measures of tolerability.
Results
Study patients
Of the 24 enrolled patients (66.7% men, mean (±SD) age 37.3±11.5 years old, 70.8% HLA-B27 positive), 12 received treatment with etanercept 50 mg once weekly and 12 received placebo. Figure 1 illustrates the disposition of patients during the study. The two groups were generally well matched in terms of demographic characteristics and symptomatic activity of disease at baseline (table 1). During the study, five patients withdrew from the study (three patients in the placebo group because of lack of efficacy, one patient in the placebo group because of lack of compliance and one patient in the etanercept group because of severe infection).
Patient demographics and disease characteristics at baseline

Patient disposition. *Two patients had a second reason for failing screening: one patient did not meet the Amor criteria and one patient had a patient global assessment (PGA) score not greater than 40.
Efficacy
Primary efficacy end point
The mean (±SD) normalised net incremental AUC for the PGA of disease activity during 12 weeks of treatment showed a significant difference between the placebo and etanercept groups (−11.1±18.0 and −28.5±18.0, respectively, p=0.029 (figure 2)).
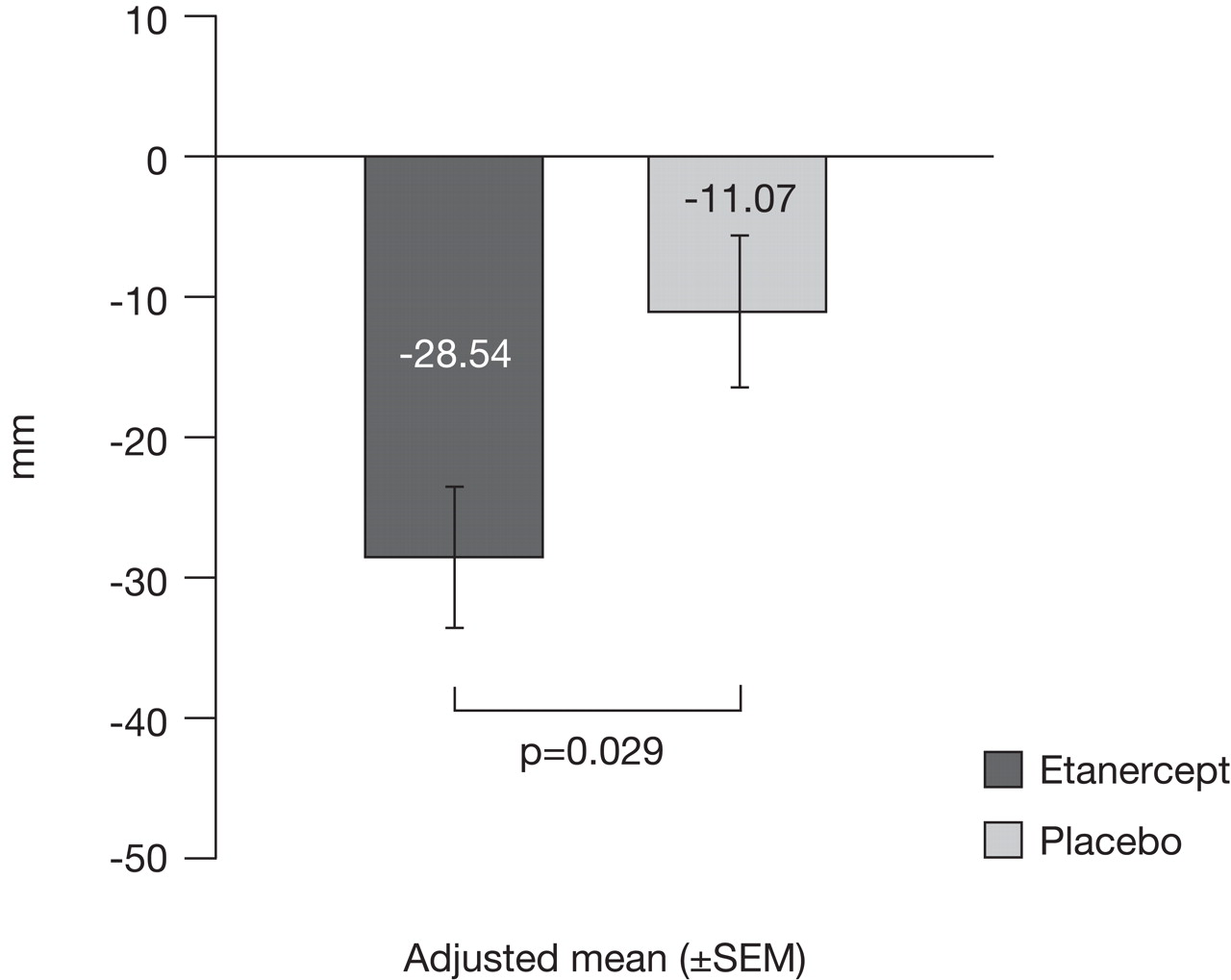
Normalised net incremental area under the curve for patient's global assessment (PGA) of heel disease activity over 12 weeks.
Secondary efficacy end points
Absolute changes between baseline and week 12 also showed statistically significant differences in favour of etanercept versus placebo for the PGA of heel enthesiopathy activity (−37.6±22.0 vs −11.6±22.0, p=0·007 (figure 3)), with a significant change from baseline beginning at week 8. Two-thirds of patients (66.7%) treated with etanercept achieved a PGA response (defined as ≥50% improvement (decrease) from baseline) at week 4 compared with 8.3% in the placebo group (p=0.011), which was maintained until week 12 (66.7% vs 16.7%, respectively, p=0.020). Statistically significant differences between etanercept and placebo were reported for the change in heel pain from baseline to week 8 (−36.1±24.0 vs −10.5±24.0, p=0.013) and to week 12 (−36.7±24.0 vs −13.1±24.0, p=0.022), WOMAC function subscale at week 12 (−23.2±16.0 vs −7.8±16.0, p=0.024) and MCII at week 12 (75.0% vs 22.2% patients very or moderately improved, p=0.020). No patients in the placebo group reported a sustained PASS, when the median time to reach such status in the etanercept group was 3.9 weeks (95% CI; 2.1; NA) (p value from a log-rank test: 0.0168) (figure 4).

Patient's global assessment (PGA) of disease activity. Absolute changes from baseline at weeks 2, 4, 8 and 12. VAS, visual analogue scale.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival analysis of time to sustained patient acceptable symptom state.
Absolute changes between baseline and week 12 showed numerical, but not significant, differences in favour of the etanercept versus placebo group for BASDAI (−19.83±20.8 vs −4.64±20.8, p=0.090), and MASES enthesitis index (−0.55±1.6 vs 0.13±1.6, p=0.296).
A total of 19 patients presented with positive MRI heel enthesitis defined by either bone marrow in the calcaneus, oedema located at Achilles tendon (posterior oedema) or at fascia plantaris (inferior oedema) according to the central radiologist. No statistically significant differences were observed in the changes in calcaneum bone oedema between the two groups (p=0.662) with an improvement in the placebo group (from 26±16 to 20±14; eg, an effect size of −0.375) and the etanercept group (from 27±16 to 17±17; eg, an effect size of −0.625).
Safety
Observed AEs are summarised in table 2. Overall, we observed no unexpected AEs or changes in laboratory test values or vital signs that gave cause for concern. A total of 10 patients in the etanercept group and 6 patients in the placebo group experienced at least 1 AE considered related to the study treatment. Infections (mainly in the upper respiratory tract) were reported in one patient in the placebo group and five patients in the etanercept group. All of these infections resolved after appropriate treatment except for one patient in the etanercept group who first experienced tonsillitis, which resolved after hospitalisation, and subsequent foot cellulitis that led to withdrawal from the study. Injection site reactions occurred in three patients in the etanercept group. Two cases of uveitis were reported during the study (one in each treatment group), but were not considered related to the study medication and no further flares were recorded. The patient in the placebo group had no history of uveitis while the patient in the etanercept group had one ongoing episode at inclusion considered as ‘stable’. In addition, one patient in the etanercept group had a history of uveitis that was considered to be ‘resolved’ at the time of inclusion and did not flare during the course of the study.
Adverse events (AEs) related to study drug during the randomised treatment period
Discussion
The HEEL trial is the first randomised, placebo-controlled, multicentre study of an anti-TNF agent for the treatment of patients with SpA with refractory heel enthesitis to show significant clinical benefits.
The study has a number of strengths, mainly the double-blind, placebo-controlled trial design that allowed for a quantitative assessment of symptomatic efficacy of etanercept in this specific presentation of SpA. In addition, the study had strict inclusion and exclusion criteria for a well defined population of patients with SpA with an objective diagnosis of heel enthesitis with calcaneum bone marrow oedema confirmed by MRI. The characteristics of the recruited patients, in particular, the long disease duration and the high level of symptoms, emphasise the disabling aspect of this condition.
The observed treatment effect of etanercept on PGA of heel enthesiopathy activity was as expected, with the primary end point being supported by statistically significant results in favour of etanercept for many of the secondary end points.
The focus on a single location of enthesiopathy could be considered a limitation of the study. In clinical trials, evaluation of enthesiopathy is traditionally performed at the patient level with use of an enthesitis scoring system to examine the tenderness at the enthesis.18 However, such scoring systems have been criticised because they are time consuming and have, poor interobserver reliability and poor face validity. Moreover, in daily practice, a frequent difficult question is related to management for a patient with a localised specific refractory enthesiopathy.
The relatively short time period of our study could be considered another limitation. However, the rapid onset of action and the sustained response with etanercept allow for a definite conclusion on its symptomatic efficacy. In contrast, the lack of statistically significant difference in the MRI findings can be explained by the small sample size and/or by the short duration of the study. The lack of statistical significance observed in the MRI evaluation in this study might be explained by the small sample size. However, at the spinal level, studies have been able to discriminate two treatment strategies (eg, placebo vs TNF blockers) after 12 weeks of treatment, even in trials of small sample size.27,–,29 The main difference between the ‘spinal’ trials and this ‘local enthesitis’ trial is that spinal trials involve use of a composite index considering different areas and the currently reported ‘local enthesitis’ trial refers to a specific area. As well, the previously reported ‘spinal’ trials lacked a placebo effect (eg, an effect size of +0.17, −0.07, −0.14 in the Barakalios et al, Lambert et al and Sieper et al studies, respectively27,–,29) as compared with the relatively relevant placebo effect we observed (eg, an effect size of −0.38). This placebo effect could reflect the natural history of the disease with spontaneous regression of heel enthesitis on MRI.2
Our results have clinical relevance because they demonstrate a marked symptomatic treatment effect of etanercept on primary and secondary end points, suggested by MRI findings. Treatment with etanercept resulted in significant improvement in PGA of disease activity over 12 weeks, along with significant improvement in secondary outcomes beginning at 8 weeks (decrease in heel pain and disability, improvement in patient global opinion (MCII and PASS)). Although the study was not designed to assess the potential toxicity of etanercept, we observed no unexpected AEs.
In summary, this is the first prospective, randomised, placebo-controlled study of enthesiopathy related to SpA that has demonstrated a symptomatic, clinically relevant and statistically significant benefit of etanercept for patients with refractory disabling heel enthesitis. The next step will be to determine the optimal management of this population in the long term.
Acknowledgments
We thank the investigators, their staff and their patients for participation in this clinical trial. We are grateful to RCTS, Lyon, France for monitoring of French centres, data management and statistical analysis of the study. Preparation of this manuscript was supported by Wyeth Pharmaceuticals, France and editorial assistance was provided by the Complete Medical Group Limited, Macclesfield, UK. We thank Carla Carvalho (Wyeth) and Florence Masson for their contributions to operational study management. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
References
Footnotes
-
Funding This study was sponsored by Wyeth Pharmaceuticals.
-
Competing interests MD, Wyeth Pharmaceuticals, consulting fees or other remuneration. BC, Schering, UCB, Wyeth Pharmaceuticals, research grants; UCB, Schering, Wyeth Pharmaceuticals: consulting fees or other remuneration. JB, Wyeth Pharmaceuticals, consulting fees or other remuneration. RL, Wyeth Pharmaceuticals, consulting fees or other remuneration. JS, Bristol-Myers Squibb, Roche Pharmaceuticals, Schering-Plough, research grants; Abbott Immunology Pharmaceuticals, Actelion, Bristol-Myers Squibb, GlaxoSmithKline, LFB, Merck Sharp Dohme, Pfizer Inc, Roche Pharmaceuticals, Schering-Plough, UCB, Wyeth Pharmaceuticals, consulting fees or other remuneration. AC, Roche Pharmaceuticals, research grants; Abbott Immunology Pharmaceuticals, Bristol-Myers Squibb, Merck Pharmaceuticals, Wyeth Pharmaceuticals, consulting fees or other remuneration. DvdH, Abbott, Amgen, Aventis, Bristol-Myers Squibb, Centocor, Pfizer, Roche, Schering-Plough, UCB, Wyeth Pharmaceuticals consulting fees or other remuneration. VL, Wyeth Pharmaceuticals, employment. IL, Wyeth Pharmaceuticals, employment.
-
Ethics approval This study was conducted with the approval of the ERC Cochin Hospital, Paris, France.
-
Provenance and peer review Not commissioned; externally peer reviewed.