Article Text

Abstract
Purpose It was hypothesised that the coding variant (R77H), rs1143679, within ITGAM could predict specific clinical manifestations associated with systemic lupus erythematosus (SLE).
Method To assess genetic association, 2366 patients with SLE and 2931 unaffected controls with European ancestry were analysed. The patients with SLE were coded by the presence or absence of individual American College of Rheumatology criteria. Logistic regression and Pearson χ2 tests were used to assess statistical significance.
Results For overall case-control analysis, a highly significant association was detected (p=2.22×10−21, OR 1.73). Using case-only analysis, a significant association was detected with renal criteria (p=0.0003), discoid rash (p=0.02) and immunological criteria (p=0.04). When patients with SLE were compared with healthy controls, the association became stronger for renal (p=4.69×10−22, OR 2.15), discoid (p=1.77×10−14, OR 2.03) and immunological (p=3.49×10−22, OR 1.86) criteria. Risk allele frequency increased from 10.6% (controls) to 17.0% (SLE), 20.4% (renal), 18.1% (immunological) and 19.5% (discoid).
Conclusion These results show a strong association between the risk allele (A) at rs1143679 and renal disease, discoid rash and immunological manifestations of SLE.
Statistics from Altmetric.com
Introduction
Systemic lupus erythematosus (SLE) is a genetically complex and clinically heterogeneous autoimmune disease. Several studies have reported differences in the prevalence of disease manifestations and outcome of SLE in various ethnic groups, which have shown variations among African Americans, Hispanics, European-derived and Asian populations. Clinical manifestations of SLE vary broadly, from relatively mild disease with long latency between the first symptom and diagnosis to the rapid progression of severe disease. In addition, clinical manifestations vary widely from patient to patient, with strong trends occurring by ethnicity and geography.1
We recently identified a novel non-synonymous single nucleotide polymorphism (SNP), rs1143679, at exon 3 of the ITGAM gene associated with SLE susceptibility2 in patients of European descent, but not in two Asian populations (Japanese and Korean).3 This missense coding polymorphism changes the amino acid arginine to histidine at position 77 (R77H). However, the effect of ITGAM on SLE was recently observed in Chinese living in Hong Kong and in a Thai population.4 These ethnic differences in genetic association with ITGAM reinforce the importance of assessing genetic polymorphisms with clinical sub-phenotypes. However, the relationship between this variant and clinical sub-phenotypes has not been studied in European-derived populations. We hypothesised that rs1143679 could predict specific clinical outcomes (sub-phenotypes) of the disease. In this study we examined the association between rs1143679 and individual American College of Rheumatology (ACR) criteria of SLE in a large cohort of patients from European ancestry.
Methods
Study population
There were 2266 unrelated cases of SLE and 2931 unrelated unaffected controls with self-reported European ancestry. All the patients with SLE met the revised ACR criteria.5 Although all individuals were ancestry-matched, most of the cases were matched by geographical location and gender with controls. The details of subject collection and characterisation are described elsewhere.2 3
Clinical data
Clinical data were collected by review of medical records based on clinical criteria classification following guidelines set out by the ACR. All individual ACR criteria were coded as positive, negative or missing. Missing data were not assumed to be negative but were excluded from clinical criteria-specific subgroup analyses.
Genotyping
Samples used in this study were part of a larger scale candidate gene association study. Details of genotyping procedures have been described elsewhere.2 3 6
Statistical analysis
The patients with SLE were grouped by the presence or absence of individual ACR criteria. Logistic regression and Pearson χ2 tests were used to assess statistical significance with rs1143679 in case-control and case-only analyses. Permutation analyses (10 000 tests) were performed to confirm significance to maximise the internal validity of these findings.
Results
As expected, we confirmed that the risk allele (A) of rs1134679 was significantly associated with SLE compared with unaffected controls (table 1). We then performed case-only analysis between individual ACR criteria-positive and ACR criteria-negative cases of SLE. This variant was significantly associated with renal criteria (p=0.0003, OR 1.39), discoid rash (p=0.02, OR 1.27) and immunological manifestations (p=0.04, OR 1.30) compared with SLE cases without these clinical manifestations. Permutation-based analyses confirmed the association with renal criteria (p=0.0007) and discoid rash (p=0.027) and borderline significance with immunological criteria (p=0.054). To see whether these variables are associated with each other, we performed three pairwise contingency association tests. While the renal criteria were significantly associated with both immunological manifestations (p=6.98×10−23) and discoid rash (p=1.89×10−5), the association between immunological manifestations and discoid rash was not significant (p=0.69). These results were also supported by multivariate logistic regression analysis using the renal criteria as the outcome variable and gender, discoid rash and immunological manifestations as covariates. Gender was not significant and was not included in the final model.
ITGAM (rs1143679) association results between patients with SLE with individual ACR criteria and controls
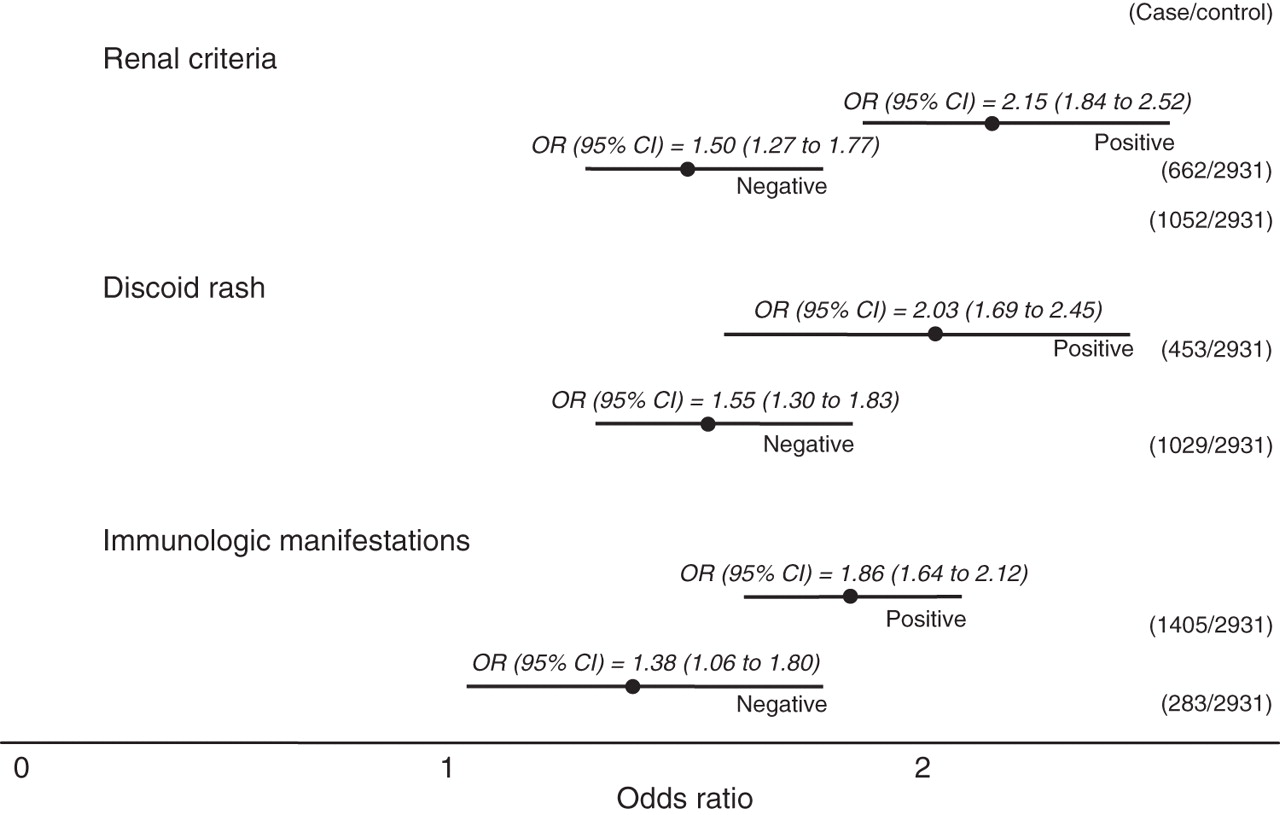
To further assess the magnitude of the associations between significant ACR criteria, we compared individual ACR criteria-positive cases with unaffected controls. The magnitude of the effect was stronger with renal criteria versus controls (p=4.69×10−22, OR 2.15), discoid rash versus controls (p=1.77×10−14, OR 2.03) and immunological manifestations versus controls (p=3.49×10−22, OR 1.86). Interestingly, renal criteria and immunological manifestations were both more significant than all SLE cases together versus controls, despite the relatively small sample numbers of ACR criteria-positive cases. The minor allele frequency (MAF) increased from 10.6% (controls) to 17.0% (SLE cases), 20.4% (renal criteria), 18.1% (immunological manifestations) and 19.5% (discoid rash). This increasing MAF confirms the trend of associations of this allele with renal criteria, discoid rash and immunological manifestations. Similarly, respective ORs were also increased from 1.73 (SLE vs controls) to 2.15 (renal criteria vs controls), 2.03 (discoid rash vs controls) and 1.86 (immunological manifestations vs controls) (table 1, figure 1). Notably, the 95% CIs did not overlap between renal criteria-positive cases versus controls and renal criteria-negative cases versus controls (figure 1). For discoid rash and immunological manifestations, the 95% CIs did overlap between positive cases versus controls and negative cases versus controls. However, the nature of the retrospective analysis could introduce bias, especially when clinical data were collected by different investigators over time. To examine the consistency of this association, we reanalysed our data separately as provided by the investigator. The consistency of our results is shown in table 1 in the online supplement.
{kind=link}
Odds ratios with 95% CI for American College of Rheumatology criteria positive and negative patients with systemic lupus erythematosus versus controls for renal criteria, discoid rash and immunological manifestations.
Autoantibody data were available for a subset of data (999 cases). Case-only analysis was performed for SLE patients positive and negative for anti-dsDNA, anti-La, anti-nRNP, anti-Ro and anti-Sm. Significant associations between rs1143679 and anti-dsDNA (p=0.0011, OR 1.65 (95% CI 1.22 to 2.23)) and anti-nRNP (p=0.006, OR 1.89 (95% CI 1.19 to 3.00)) were observed.
Discussion
ITGAM encodes a cell surface receptor protein (integrin) that is implicated in various adhesive interactions of monocytes, macrophages and granulocytes as well as in mediating the uptake of complement-coated particles. After identifying variants associated with disease risk, it is important to correlate genotypic data with phenotypic expression of the disease that may provide insight into the pathogenesis of the disease and, more importantly, new therapeutic approaches. Subsetting allows us to create more homogeneous groups of patients and thus may increase the power to detect associations despite the reduced sample size.
In this study we found that patients with SLE often had stronger associations between SLE and rs1143679 when they were stratified by certain clinical ACR criteria, especially renal criteria, discoid rash and immunological manifestations. While the results confirm that rs1143679 was strongly associated with SLE in general, patients with SLE with renal criteria, discoid rash and immunological manifestations were enriched for the risk allele (A) and risk estimates (ORs) were substantially increased, especially for renal criteria (figure 1).
The strongest associations in individuals of European descent were found for SLE cases positive for renal criteria compared with cases without this clinical manifestation. A similar result was recently observed among Chinese and Thai populations.4 Renal criteria are one of the most serious manifestations of SLE and are a major predictor of poor prognosis7 and mortality.8 Among those patients with renal criteria, nearly 70% of patients never treated with cyclophosphamide develop end-stage renal disease.8 As confirmed by our logistic regression analysis, various clinical manifestations are associated with renal criteria. It would be important to follow up this study with more clinical information and possibly information about environmental variables. Indeed, clinical and ethnic subsetting of SLE may help to explain the natural history of SLE differences by ethnicity.
Our results may provide a genetic correlate into the proposed role by which ITGAM mediates the inflammatory processes in the pathogenesis of SLE. ITGAM (CD11b) expression was shown to increase DNA fragmentation, a prerequisite for apoptosis, and the level of fragmented DNA is increased in intravascular cells, which induces interferon α in SLE mice.9 CD11b also induces tumour necrosis factor α10 and modulates the innate immune mechanism11 in patients with SLE. This suggests that the association of this SNP in ITGAM with the molecular mechanism of immunological manifestations may be correlated. Although the molecular mechanism of discoid rash and involvement of ITGAM has not previously been assessed, it could also be a clinical manifestation of cell-mediated immunological reactions. ITGAM is a major surface receptor in monocytes, and monocytes are involved in clearing deposits from glomeruli.12 In the normal kidney, ITGAM is expressed on endothelial cells of glomerular and peritubular capillaries of Bowman's capsule but, in patients with renal criteria, its expression is significantly increased on tubular epithelial cells and on infiltrating mononuclear cells.13 In contrast, extensive series of studies by two groups14 15 suggest that C3b receptor (CR3, ITGAM) expression is decreased in patients with renal criteria compared with control groups. It is also possible that cellular regulatory mechanisms allow ITGAM to be overexpressed to cope with the loss of clearance of deposits in glomeruli by monocytes. However, whatever the disease mechanisms, this SNP changes the amino acid (R77H) in the vicinity of α domain (metal ion binding domain or A domain) and may overall modulate the numerous ligand binding activities of ITGAM in monocytes, neutrophils and dendritic cells. Within this context, it is conceivable that risk allele (A) may confer its effect through mutant receptor protein with respect to ligand binding affinity, or this change may aggravate the inflammatory process by decreasing initial kidney cellular infiltration. These individuals are prone to develop renal criteria together with other manifestations such as discoid rash or immunological manifestations.
In summary, we have consistently shown a strong correlation between the coding variant (rs1143679) of ITGAM and renal, discoid and immunological manifestation of SLE. The next challenge is to understand how this coding variant actually modulates the molecular pathways leading to kidney involvement or other associated clinical manifestations in SLE.
Acknowledgments
The authors thank the patients and their families for their contribution to this study with both clinical and specimen data. They also acknowledge the support from LFRR staff, especially Jennifer Kelly, Dr Joshua Ojwang and Dr Ken Kaufman for conducting a large-scale genotyping project in which the current samples were genotyped. They also thank the three anonymous reviewers for their comments which definitely improved the quality of this manuscript.
References
Supplementary materials
Web Only Data ard.2009.120543
Files in this Data Supplement:
Footnotes
-
Funding This study was supported by funding from AR42460, AR12253, AR48940, Alliance for Lupus Research, A1063622, AR053483, RR020143 and AR049084.
-
Patient consent Obtained.
-
Ethics approval The study was approved by the Institutional Review Boards of the respective institutions.
-
Provenance and peer review Not commissioned; externally peer reviewed.