Article Text

Abstract
Objectives: To compare the effects of etanercept (ETN) 50 mg once weekly plus methotrexate (MTX) versus MTX alone on patient-reported outcomes (PROs) and the relationship between remission and PRO improvement.
Methods: In this double-blind, randomised clinical trial (COMET), PROs included: the Health Assessment Questionnaire (HAQ), EuroQoL health status, fatigue and pain visual analogue scales, Hospital Anxiety and Depression Scale, and Medical Outcomes Short-Form-36. Mean changes from baseline were analysed by analysis of covariance using the last observation carried forward method. Results from week 52 are presented.
Results: Most PROs demonstrated significantly greater improvements with ETN+MTX than MTX alone, including physical functioning, pain, fatigue and overall health status. A significantly greater improvement in HAQ score was observed in the ETN+MTX than the MTX group (−1.02 vs −0.72; p<0.001) and a greater proportion reached the minimal clinically important difference of 0.22 (88% vs 78%; p<0.006). The relationship between PRO score and clinical status indicated that improvement was greatest among patients achieving remission.
Conclusions: Early treatment with ETN+MTX leads to significantly greater improvements in multiple dimensions of PROs than MTX alone. The close relationship between disease activity and PRO improvement suggests that early treatment, with remission as a goal, should maximise the chance of restoring normal functioning and HRQoL.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic, systemic, inflammatory disease characterised by progressive synovial joint inflammation and destruction.1 2 Over time, the disability may result in loss of mobility and inability to care for oneself, making physical and psychosocial outcomes important endpoints for analysis of treatment efficacy. Patients with RA report decreased health-related quality of life (HRQoL) for a number of physical functioning and mental health dimensions, including depression and fatigue.2 3 4 5
These are expected consequences from long-standing RA; however, even patients with early RA report that it adversely affects their HRQoL.3 6 7 8 Early therapeutic intervention to prevent irreversible joint damage may offer an opportunity to avoid disability from RA, thus improving HRQoL as shown in other reports.3 9 10 11
Remission, the most desired clinical outcome, is achieved by few patients with established disease;12 however, for patients with early RA, remission is a realistic goal if timely treatment is administered.13 The COMET (Combination of Methotrexate (MTX) and ETanercept (ETN) in active early RA) trial,14 which enrolled patients with moderate-to-severe RA with a disease duration from 3 months to 2 years inclusively, found that early intervention with ETN+MTX combination treatment prevented further joint damage with half the patients reaching clinical remission at the end of the study’s first year.
The objectives of the present study were to examine the effects of combination treatment with ETN+MTX versus MTX alone on HRQoL, using PROs in patients in the COMET trial, and to assess the relationship between remission and PRO improvement.
Patients and methods
PRO assessments were secondary endpoints to the COMET study, a 2-year, double-blind trial of patients randomised to receive ETN 50 mg once weekly plus MTX or MTX alone. Results from week 52 are reported here. Patients in this study had disease of duration ⩽2 years, were MTX-naïve, had disease activity scores based on a 28-joint assessment (DAS28) of ⩾3.2 and provided written informed consent in compliance with the Helsinki Declaration. Detailed study design and results of primary endpoints have been published.14
PRO measures included the Health Assessment Questionnaire (HAQ),15 EuroQoL health status (EQ-5D) and visual analogue scale (VAS) (EQ-5D VAS),16 fatigue VAS, pain VAS, Hospital Anxiety and Depression scale (HADS)17 and Medical Outcomes Short Form-36 (SF-36).18 Details of the instruments are provided in table 1.
Patient-reported outcome scores at baseline and week 52 in patients with early RA by treatment group
Data analysis on the modified intention-to-treat (mITT) population included patients that received at least one dose of assigned treatment and provided at least one post-baseline evaluation. The last observation carried forward (LOCF) method was applied for missing data.20
Changes from baseline to week 52 of treatment for all PRO scores underwent analysis of covariance (ANCOVA), including terms for baseline, country and treatment. The significance of within-group mean changes from baseline was assessed using paired t-tests. The impact of remission on PRO improvement was determined to evaluate how patient perspective on improvement tracked disease activity status. Both treatment groups were combined to create three mutually exclusive disease activity categories: “achieved remission” (DAS28 <2.6), “achieved low disease activity (LDA) but not remission” (DAS28 ⩾2.6 but ⩽3.2) and “did not achieve LDA” (DAS28 >3.2). ANCOVA models estimated least squares of mean of baseline to week 52 score changes for PROs, including factors for age, sex and baseline scores.
Results
The mITT population constituted 528 subjects (MTX = 263; ETN+MTX = 265). Baseline demographic and disease characteristics were similar with mean age 51 years, mean disease duration 9 months and mean DAS28 = 6.5. Detailed baseline data are published.14
As expected, patients at baseline reported major physical impairments with mean SF-36 PCS score that was 2 SDs below normal (50.0).18 Baseline HADS scores indicated that some patients had symptoms of depression (39.7%) and anxiety (47.3%) (data not shown), denoted by scores ⩾8 for each dimension,17 confirming SF-36 MCS scores also indicating poor mental health (table 1).
At the end of year 1 of treatment, subjects receiving ETN+MTX achieved a significantly greater improvement in HAQ score than those receiving MTX alone (−1.02 vs −0.72; p<0.001; table 1). Most patients (55%) receiving ETN+MTX reached HAQ scores representative of the general population (⩽0.5),21 compared with 39% of patients receiving MTX (data not shown). In addition, the ETN+MTX group had significantly more subjects meeting minimum clinically important differences in HAQ (−0.22)22 than the MTX group (88% vs 78%; p = 0.006).
ETN+MTX subjects achieved a significantly greater improvement in EQ-5D utility and EQ-5D VAS scores than did the MTX group. Significantly more patients receiving ETN+MTX achieved an EQ-5D VAS score approaching population norms (>82)23 than did the MTX group (39.8% vs 29.9%; p = 0.029, data not shown).
Decreases in fatigue VAS scores (indicating improvement) were rapid and significantly greater for patients receiving ETN+MTX than patients receiving MTX (p<0.001), declining to almost half in the ETN+MTX group as early as week 2 (data not shown). Improvement in the pain VAS was significantly greater with ETN+MTX compared with MTX alone (p<0.001).
Improvement in HADS anxiety and depression subscale scores, achieved by both groups, was not significantly different.
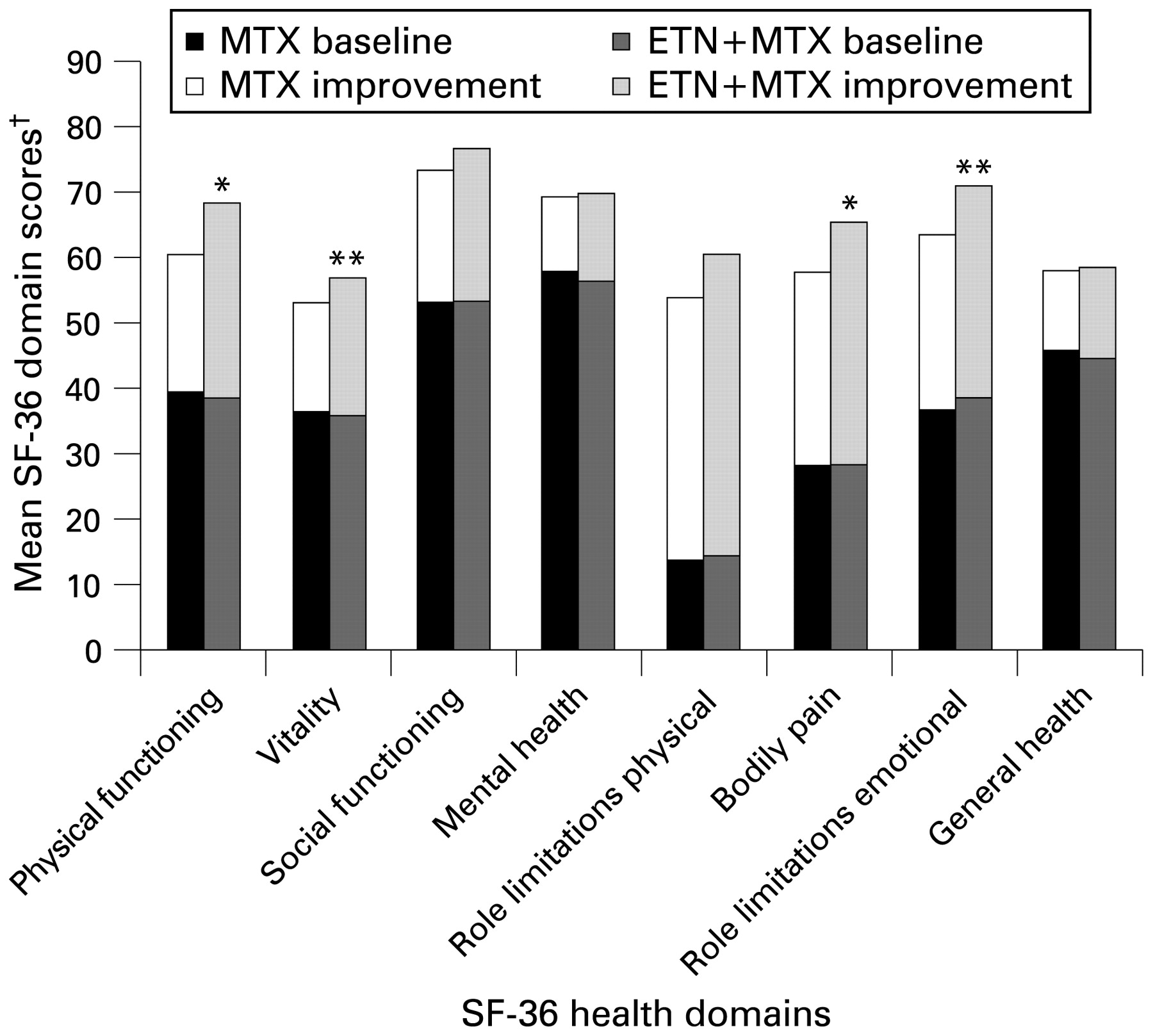
Improvement in SF-36 scores was significantly greater in the ETN+MTX group than the MTX group in domains of physical functioning, vitality, bodily pain and role-limitation emotional (fig 1) and SF-36 PCS scores (table 1). Greatest improvements were observed in physical domains, including physical functioning, role limitations-physical and bodily pain. SF-36 MCS yielded no significant differences.

{kind=link}
Change in mean SF-36 scores from baseline and 52 weeks after treatment with ETN+MTX or MTX alone. ETN, etanercept; MTX, methotrexate; SF-36, Medical Outcomes Short-Form 36. *p<0.001. **p = 0.02. †Each domain range is from 0 (worst) to 100 (best).
Analyses performed to examine the relationship between 52-week PROs and remission or LDA were adjusted for age, sex and baseline score (table 2). Overall, for all PROs, the differences between patients who “achieved remission”, “achieved LDA but not remission”, and “did not achieve LDA” were statistically significant (p<0.0001). Patients who achieved remission showed greatest improvement in PROs, followed by patients who achieved LDA but not remission. Pairwise comparisons of changes in PROs between disease activity categories also revealed statistically significant differences, favouring groups who achieved better disease control with one exception (table 2).
Adjusted mean change (SE) in patient-reported outcomes from baseline to week 52 by disease status
Discussion
Patients with early RA may experience chronic pain, stiffness and joint damage, leading to severe disability. The COMET trial demonstrated that early therapeutic intervention with ETN+MTX yielded significantly greater improvements in most PROs, including physical functioning, fatigue, pain and overall health state over MTX alone.
Fatigue, an important symptom in the majority of patients with RA, has numerous consequences on HRQoL.24 The Outcome Measures in Rheumatology group recommends that it be an outcome measured in RA studies.25 In COMET, the ETN+MTX group reported a significantly greater improvement in fatigue VAS scores than the MTX group. A rapid and substantial reduction of fatigue may have contributed to overall improvement in HRQoL.
Patients receiving ETN+MTX reported a significantly greater improvement in functional status with a greater proportion achieving clinically meaningful improvement than patients receiving MTX. By week 52, 55% of the ETN+MTX group achieved a HAQ score of ⩽0.5, scores comparable with those for the general population.21 In the TEMPO (Trial of Etanercept and Methotrexate with Radiographic Patient Outcomes) study of patients with established RA, 44% of those receiving ETN+MTX reached this same HAQ score.26 Moreover, combined analysis from six recent RA trials demonstrated that difficulty to improve HAQ scores increased with disease duration.27 Taken together, these data suggest that early intervention may offer a better chance of restoring normal physical functioning and improvement.
Consistent with HAQ results, improvement in SF-36 PCS scores was significantly better for patients receiving ETN+MTX than the MTX group (13.7 vs 10.7; p = 0.003). A change from baseline in PCS or MCS score of 2.5 to 5.0 or of 5 to 10 points in the individual domain scores of SF-36 are considered minimums to attach clinical importance to differences (MCID),28 29 30 thus the changes seen in the COMET trial can be considered substantial improvements. Additionally, between-group differences in SF-36 PCS scores fall within the MCID. Although not all SF-36 domain scores differed between the groups, the largest differences were observed in domains of physical functioning and bodily pain.
This study also demonstrates that the impact of remission directly translates into greater benefit from the patient perspective, supporting recommendations of the EULAR Working Group31 and the American College of Rheumatology Subcommittee on RA Guidelines,32 which state that remission should be the goal of treatment for patients with RA. Gains from baseline SF-36 PCS scores in the “achieved remission” group would place most of these patients with early RA at population norms of 50.0.18 This is consistent with the post-treatment HAQ score reduction from a baseline score of 1.7 to 0.4 among subjects achieving remission and also approaching values in the general population.21 Similarly, the improvement in EQ-5D utility score was substantial among patients achieving remission. This evidence demonstrates that early treatment, with remission as the ultimate goal, could allow more patients to return to normal functioning.
Study limitations include use of the LOCF method for missing PRO data, which may introduce bias if scores change over time;20 however, results of analysis of the observed (per protocol) population are consistent with LOCF results. The single-item fatigue VAS may limit the ability to measure multiple aspects of fatigue; however, comparison with a longer fatigue questionnaire showed there was no performance advantage.33
In summary, the COMET study demonstrated that ETN+MTX provide a significantly greater improvement in multiple PRO measures than MTX alone. Moreover, the close relationship between disease activity and PRO improvement suggests that clinical remission as a treatment goal in early RA should maximise the chance of restoring normal functioning and HRQoL.
Acknowledgments
The authors wish to thank the investigators, their staff and the subjects involved in the trial.
REFERENCES
Footnotes
Funding This study was funded by Wyeth Research, USA. This article was prepared with the assistance of BioMedCom Consultants inc, Montreal, Canada.
Competing interests JK was an investigator for this trial. RM and PE has served as a consultant, received research grants from Wyeth, and were investigators for this trial. PD was an investigator for this trial and has received speaker's fee from Wyeth. DR, RP, AS, AK, BF and RS are employees of Wyeth.
Provenance and Peer review Not commissioned; externally peer reviewed.
Linked Articles
- Miscellaneous