Article Text

Abstract
Objective: To investigate the effect of tumour necrosis factor (TNF) antagonist treatment on workforce participation in patients with rheumatoid arthritis (RA).
Methods: Data from the Stockholm anti-TNFα follow-up registry (STURE) were used in this observational study. Patients with RA (n = 594) aged 18–55 years, (mean (SD) 40 (9) years) followed for up to 5 years were included with hours worked/week as the main outcome measure. Analyses were performed unadjusted and adjusted for baseline age, disease duration, Health Assessment Questionnaire (HAQ), 28-joint Disease Activity Score (DAS28) and pain score.
Results: At baseline patients worked a mean 20 h/week (SD 18). In unadjusted analyses, significant improvements in hours worked/week could already be observed in patients at 6 months (mean, 95% CI) +2.4 h (1.3 to 3.5), with further increases compared to baseline at 1-year (+4.0 h, 2.4 to 5.6) and 2-year follow-up (+6.3 h, 4.2 to 8.4). The trajectory appeared to stabilise at the 3-year (+6.3 h, 3.6 to 8.9), 4-year (+5.3 h, 2.3 to 8.4) and 5-year follow-up (+6.6 h, 3.3 to 10.0). In a mixed piecewise linear regression model, adjusted for age, sex, baseline disease activity, function and pain, an improvement of +4.2 h/week was estimated for the first year followed by an added improvement of +0.5 h/week annually during the years thereafter. Over 5 years of treatment, the expected indirect cost gain corresponded to 40% of the annual anti-TNF drug cost in patients continuing treatment.
Conclusion: Data from this population-based registry indicate that biological therapy is associated with increases in workforce participation in a group typically expected to experience progressively deteriorating ability to work. This could result in significant indirect cost benefits to society.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is characterised by progressive inflammatory synovitis and destruction of articular cartilage and marginal bone, adversely affecting physical function and workforce participation. The economic burden of RA is considerable and productivity loss is one of the main contributing factors.1 However, recently significant attention has also been directed towards the rapidly increasing drug costs due to the introduction of biological treatments such as tumour necrosis factor (TNF) antagonists. While their effects on slowing and even arresting joint destruction are well documented,2 3 4 5 6 7 effects on workforce participation and its cost implications are not.
The impact of anti-TNF treatment on work outcomes has been studied in short-term observational studies, but these have generated inconclusive results. Yelin et al found significant improvements in hours worked/week over 1 year in patients treated with etanercept compared to untreated patients.8 In contrast, no substantial decrease in cost was found in a recent observational study comparing work disability costs during the first year of treatment with infliximab to the costs incurred during the year before start of treatment.9 More recently employment loss was found not to differ between American patients with RA treated with TNF antagonists compared to matched controls, although a significant benefit was found in the subgroup with a disease duration <11 years.10 Mittendorf et al found sustained ability to work over 144 weeks of treatment with adalimumab in an open label study, but no significant improvement.11 In a recent randomised controlled trial (RCT), treatment with adalimumab was associated with reduced job loss.12 These results were confirmed in an open label extension study showing that patients with RA who were working at treatment initiation were able to work 7.3 months longer than the matched control group.13 No study has hitherto analysed long-term data on all three TNF antagonists in a population-based sample. Short-term data may be insufficient to capture effects on workforce participation due to system inertia. Furthermore, it is of interest to describe the trajectory over time of potential beneficial effects.
Therefore, the aim of this study was to determine whether treatment with etanercept, infliximab or adalimumab over up to 5 years is associated with changes in workforce participation in a population-based patient cohort. If such an increase appeared to be present, a secondary aim was to explore the economic implications of treatment with TNF antagonists.
Methods
Data source
Prospectively collected data in the Stockholm anti-TNFα follow-up registry (STURE) database were analysed. The STURE database collects efficacy data, including employment status, and safety data for all patients starting biological treatments at all major hospitals in Stockholm, Sweden. STURE is part of the nationwide registry for Anti-Rheumatic Therapies In Sweden (ARTIS).14 Assessments are performed at treatment initiation and at 3-month, 6-month and 12-month follow-up visits and annually thereafter. These include the American College of Rheumatology (ACR) core outcomes (ie, visual analogue scales for global health and for pain), the Health Assessment Questionnaire (HAQ), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), doctor’s global assessment of disease activity, 28 swollen and tender joint counts and the 28-joint Disease Activity Score (DAS28).15 16 At each visit, employment status is ascertained by a multiple choice question providing the following response alternatives: “I am retired since …… (year) …… (month)”, “I work full time ……hours/week”, “I cannot work full time due to my rheumatic disease, I’m currently working …… hours/week” (follow-up questions on type of sickness benefit/disability pension) or “I cannot state my current work force ability (unemployed, student, maternity leave)”.
Recruitment into the study occurred between 1999 and 2007. Therefore, the duration of follow-up varied from 6 months to 8 years. Data from follow-up after 5 years of treatment were not analysed.
Patients who were old age pensioners, on permanent work disability pension, those outside the usual workforce (eg, students, maternity leave, etc) or over the age of 55 years at start of treatment were excluded, resulting in a cohort of 594 patients. Only data from the first treatment period for each patient were used since patients could have been treated with several TNF antagonists during the study period (1999–2007).
Statistical analysis
Statistical analyses were conducted using SAS (V.9, SAS Institute, Cary, North Carolina, USA) and SPSS (V.15.0; SPSS, Chicago, Illinois, USA). Differences between males and females at baseline in age, HAQ, DAS 28, pain VAS and hours worked/week were assessed using independent samples Student t tests. Differences between patient groups defined by drug (etanercept, infliximab, adalimumab) were investigated using analysis of variance (ANOVA) with the Bonferroni post hoc test for multiple comparisons.
Crude changes in hours worked/week at 6 months, 1, 2, 3, 4 and 5 years were assessed by paired Student t tests using complete case analyses. As informative censoring can be suspected due to drug discontinuation, separate analyses were also performed for patients not discontinuing biological treatment during follow-up.
To model the trajectory of hours worked/week, a mixed piecewise linear regression model with a random intercept was fitted. This method uses all repeated measurements, taking unevenly spaced measurements and missing data into account and makes it possible to estimate within-subject variations in hours worked/week with great precision as each individual acts as his own control.17 By this method, fixed effects varying between, but constant within, subjects over time are accounted for. In order to allow for curvature in the trajectory, a knot was inserted at 1 year based on visual inspection. Consequently, the development could take on a different (or the same) slope before and after 1 year. The models rely on the assumption that missing observations are missing at random. As drug discontinuation is likely to result in informative censoring, the model was first fitted to the whole dataset and thereafter only to data from patients not discontinuing treatment. Furthermore, a model using only patients working half of the time at baseline was estimated in order to reduce the potential impact of left and right censoring.
An attempt to approximate the monetary value of changes in hours worked/week was made by using the mean wage rate in Sweden, retrieved from the Statistics Sweden website (http://www.scb.se). The area under the curve from annual change in hours worked was multiplied by the average wage rate/h in the population, including social fees. The productivity gains were estimated by using the most likely conservative assumption that without treatment the hours worked/week would remain unchanged over 5 years.
A p value of <0.05 was considered statistically significant.
Results
Patient characteristics at baseline are shown in table 1. In all, 66% of patients were female, and infliximab was the most common drug used (52.9%) followed by etanercept (34.5%) and adalimumab (12.6%). Age, disease duration and pain scores did not differ significantly between the sexes, but females had significantly higher HAQ (0.21; p<0.001) and DAS 28 (0.60; p<0.001) than males. No sex difference was detected in hours worked/week at baseline (−2.7 h; p = 0.08).
Patient characteristics at baseline (age range 18–55 years)
There were no between-drug differences, except for HAQ at baseline (adalimumab vs infliximab −0.23, p = 0.02; adalimumab vs etanercept −0.24, p = 0.01) and hours worked/week (adalimumab vs infliximab 8 h, p = 0.001; adalimumab vs etanercept 7 h, p = 0.008), most likely reflecting the later market introduction of adalimumab when an intention to treat earlier to prevent irreversible damage had developed.
In univariate correlation analyses, hours worked at baseline were significantly correlated with HAQ (r = −0.36), DAS28 (r = −0.29) and pain (r = −022; all p<0.001), but not age.
Drug discontinuation
During follow-up, 287 patients discontinued their first biological treatment. Discontinuers did not differ from continuers in age (0.4 years; p = 0.62) or pain at initiation (−0.5; p = 0.81), but had higher HAQ (0.14; p = 0.01) and DAS values (0.3; p = 0.02), as well as fewer hours worked/week at baseline (−5.4; p<0.001).
Changes in productivity (paired Student t tests)
Significant improvements in hours worked/week were seen in patients up to 5 years of follow-up (table 2). Not all patients contributed data at all time points and the sample size was diminished at each successive timepoint due to irregularly spaced follow-up measurements, variation in length of follow-up and treatment discontinuation. The number of hours worked at baseline was similar for patients followed for different durations, and significant increases in productivity were observed irrespective of length of follow-up for the whole sample (table 2). When restricting the analysis to only patients who did not discontinue treatment during follow-up, greater increases were observed (table 2).
Changes in hours worked/week at different lengths of follow-up for the whole sample and for patients not discontinuing treatment during follow-up
Changes in productivity (mixed effects model)
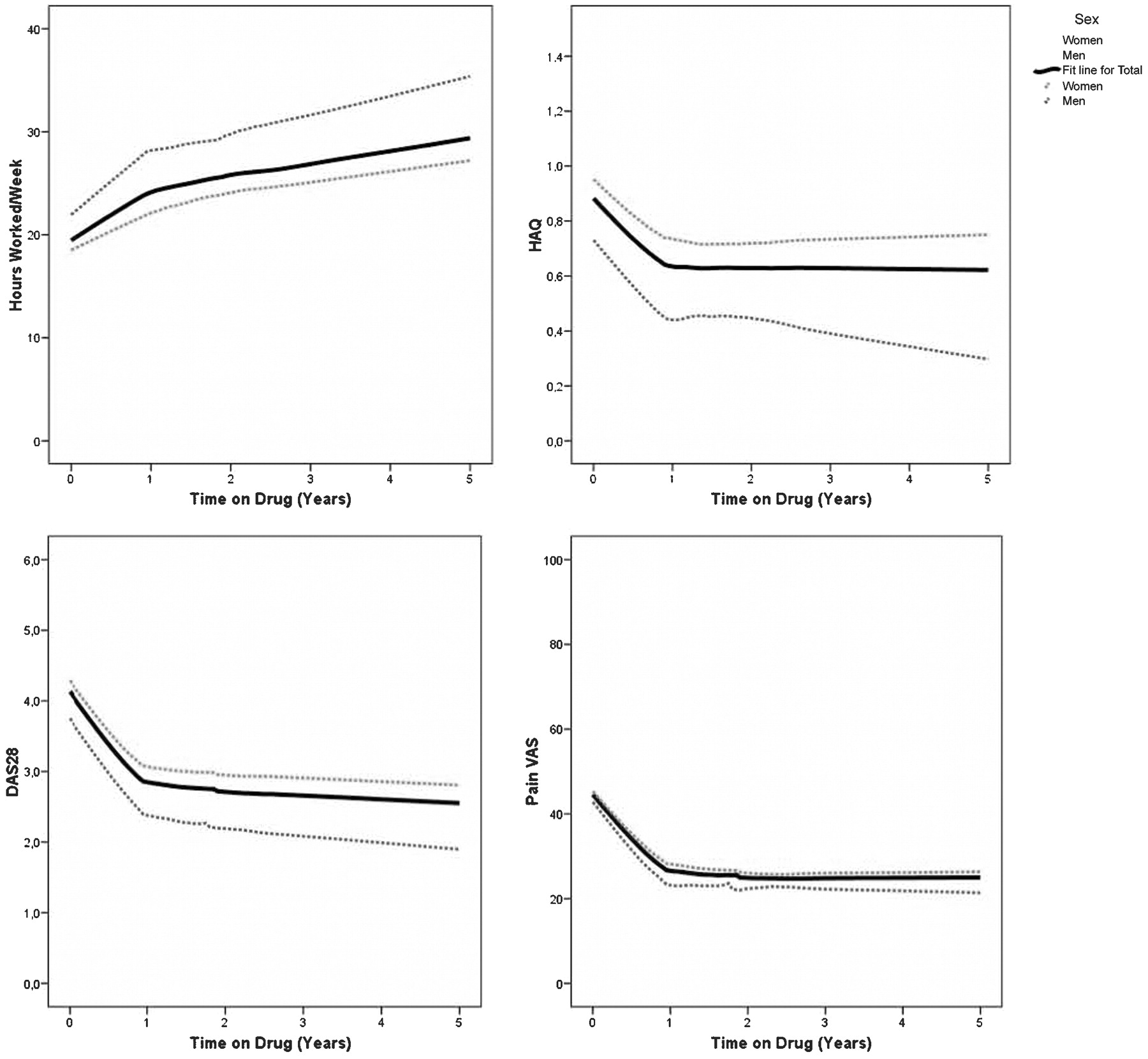
The development in hours worked/week, HAQ, DAS28 and pain VAS scores for the whole group is shown in fig 1, based on all observations during the first 5 years of follow-up. The Lowess-fitted curves indicate greater improvements in all outcomes during the first year of treatment than thereafter. Therefore a piecewise mixed model was fitted with a knot at the 1-year timepoint, allowing for a curvature change after 1 year. In the unadjusted model, an improvement of 4.2 h worked/week during the first year was estimated, and a smaller increase of an additional 0.5 h/year thereafter. After adjustment for sex, age, HAQ, DAS28 and pain at baseline, the estimate changed only marginally to 4.1 h during the first year and not at all for the years thereafter.
{kind=link}
Change in hours worked/week, Health Assessment Questionnaire (HAQ), 28-joint Disease Activity Score (DAS28) and pain visual analogue scale (VAS) over 5 years of biological treatment. Curves fitted by Lowess, using all available measurements from all patients (nh/week = 594 (394 F, 200 M), nHAQ = 528 (355 F, 173 M), nDAS = 521 (354 F, 167 M), npain VAS = 543 (367 F, 176 M). F, female; M, male.
Restricting analysis to patients working 20 h/week at baseline to reduce the impact of right and left censoring resulted in similar estimates of 4.0 and 0.6 h/week. Restricting analysis to non-discontinuers, a greater increase of 5.3 h/week was seen during the first year and 0.9 h/week in subsequent years. Adding anti-TNF drug did not improve model fit and no significant between-drug differences in productivity change could be detected (pinteraction = 0.79).
Economic consequences
Based on the most likely conservative assumption that patient productivity would not deteriorate from baseline values over 5 years without anti-TNF treatment, the productivity gains for society in patients continuing treatment would total €27 000 over 5 years. This corresponds to approximately 40% of the annual anti-TNF drug cost. Estimating the costs by using the unadjusted data, originating from fixed time points (table 2), a similar estimate of €28 000 over 5 years resulted. Note that these estimates only apply to patients who do not discontinue treatment, a group that may be difficult to identify before treatment initiation.
Discussion
In this observational study we investigated the development of hours worked/week in patients with RA treated for up to 5 years with TNF antagonists. At baseline the average patient worked half time, but during the first year of treatment this was increased by approximately 4 h. After the first year smaller annual improvements occurred. The shape of the trajectory was similar to the development in measures of disease activity, physical function and pain, although these measures had a more rapid improvement and had reached a more pronounced plateau at 1 year. Assuming that the patients’ ability to work had remained unchanged over 5 years without biological treatment, the indirect cost gains from improved ability to work in continuers would offset approximately 40% of the drug cost.
The results from the current study are congruent with some previous studies on effects on ability to work of anti-TNF treatment. Yelin et al found significant improvements in hours worked/week over 1 year in patients treated with etanercept compared to untreated patients and Allaire et al found a significant benefit in the subgroup with a disease duration <11 years.8 10 The results do, however, conflict with the findings of Mittendorf et al, who could not detect any improvements in hours worked/week over 3 years of follow-up, although ability to work did not deteriorate either, and Laas et al who found no substantial decrease in work disability costs during the first year of treatment with infliximab.9 11 The sources of these discrepancies may be different length of follow-up, differences in disease severity in the samples investigated, and differences in the labour market in the respective countries. Furthermore, the lack of or specific choice of control group may also contribute.
Anti-TNF treatment led to large and sustained improvements in disease activity and disease function over up to 5 years in this study, which was paralleled by improvements in ability to work. The small increases in ability to work observed beyond year 1, at which time the clinical effect of TNF antagonists stabilised may reflect inertia in the labour market or at the patients’ workplace. However, these small improvements are valuable especially if the improvement in working hours is sustained over several years.
It has been shown that early suppression of disease activity is essential for maintenance of work capacity in patients with recent onset rheumatoid arthritis.18 The disease leads to early consequences in the context of work capacity in the majority of cases, as exemplified by a Swedish study with 15 years of follow-up reporting work disability rates changing from 28% at study start to 44% at 15 years. HAQ was the only factor that remained significant at all time points during the study period.19 In the present study we found that several of the same factors are important in established RA. For example, disease status measured by HAQ at baseline remained strongly correlated with ability to work.
Anti-TNF treatment has been shown to be highly efficacious in several subgroups of patients, but is also very costly.2 4 20 21 This makes it a natural candidate for cost effectiveness analysis with the aim of finding in which patient subgroups their use provides good value for money. When performed from the perspective of the UK National Health Service (NHS), as recommended by the UK National Institute for Clinical Excellence (NICE), indirect costs are disregarded. Reimbursement authorities in other countries (eg, Sweden) require cost effectiveness analyses to be performed from the societal perspective, including also productivity losses. Direct data on productivity effects of anti-TNF treatment have henceforth been scarce, and indirect approaches have been used in modelling attempts: evidence of HAQ reductions while on treatment has been coupled with other data sources showing a relationship between HAQ and productivity.22 The results from the current study provide direct data indicating that anti-TNF treatment results in significant gains elsewhere in the societal budget for patients of working age. These data are of importance to inform decision makers facing reimbursement judgments.
The strengths of this study were its long follow-up, population-based design with prospectively collected data and availability to data on all three TNF antagonists. Its external generalisability is also a strength, as it was based on data from actual clinical practice and patients were not subjected to strict inclusion and exclusion criteria, as in randomised controlled trials.
The study was also subject to limitations. Firstly, there was no control group to which the ability to work changes could be compared to assess what would have happened without treatment. However, RA is a progressive disease and ability to work in patients with RA has been shown to be characterised by deteriorating ability to work over time.23 However, we could demonstrate increases in hours worked. Furthermore, the mean number of hours worked/week in the general population remained stable at approximately 30 h/week during the study period.24 In the current study, the overall hours worked/week by patients with RA were approximately 10 h lower at baseline, a difference that was approximately halved after treatment initiation.
Mittendorf et al, who did not detect increases in ability to work but no deterioration either in an observational study, argued that prevention of further work loss in this patient group may be a worthwhile goal. Hence it is likely that the actual productivity gains are larger than the ones calculated based on the assumption of unchanged ability to work over time. There is, however, a risk of effect overestimation in observational studies such as this, if anti-TNF treatment is initiated during a flare, and the observed gain is caused partly by regression to the mean.
Although more patients increased their number of hours worked per week, some also decreased, not only among full time workers. This is not evidence of absence of regression to the mean, but the fact that variations occurred in both directions indicates that treatment initiation did not necessarily happen when ability to work was at its minimum.
Secondly, ability to work was assessed by self-report. Objective assessment through retrieval of register data could potentially provide better information. It could also provide answers regarding the potential regression to the mean effect, as the long-term sick leave trajectory would be available.
Thirdly, data were only collected while patients were still on anti-TNF treatment, not after withdrawal. Hence the patients still on drug after 5 years were not a random sample of the initial population (ie, differential dropout is likely). Indeed, the productivity gains were greater in continuers than discontinuers, and the results regarding drug cost offsets can only be applied to the selected group of continuers.
Finally, impaired productivity while at work25 and unpaid work were not assessed in this study.
Conclusions
Data from this population-based study indicate that biological therapy is associated with increases in workforce participation over up to 5 years in a group typically expected to experience progressively deteriorating ability to work. This could result in significant indirect cost benefits to patients and society.
REFERENCES
Footnotes
Funding JA was funded by Apotekt Farmaci AB. The funding sources did not read or comment on any version of the manuscript, nor influence the analyses in any way.
Competing interests None.
Ethics approval The ethics committee at the Karolinska Institute, Stockholm, Sweden, approved the study.
JA and RFV conceived the hypothesis for the manuscript and conducted the initial statistical analyses. JA wrote the first draft of the manuscript and had the main responsibility for the manuscript process. MN contributed to statistical analyses, health economics and the manuscript. CCC contributed to data collection and SE contributed to the statistical analyses. CCC, MN, RFV and SE and provided critical input at all stages and critically reviewed and contributed to the final draft. All authors are guarantors.
Provenance and Peer review Not commissioned; externally peer reviewed.