Article Text

Abstract
Objective: Cartilage oligomeric matrix protein (COMP), primarily found in cartilage, is thought to be an important regulator of assembly and maintenance of the fibrillar collagen I and II networks. Recently, COMP was shown to be produced by skin fibroblasts from patients with systemic sclerosis (SSc, or scleroderma). The purpose of this study was to examine whether COMP is released from skin to serum in patients with SSc, and may serve as indicator of activity of skin involvement.
Methods: Serum COMP levels were measured by enzyme linked immunosorbent assay in patients with SSc whose skin involvement was assessed with the modified Rodnan skin score (mRss) and high frequency ultrasound. The presence of COMP in skin biopsies was assessed by Western blot using a monoclonal antibody specific for the very C-terminal end of human COMP.
Results: Serum COMP correlated to skin involvement as measured by the mRss (n = 70; rS = 0.60; p<0.001), to skin thickness measured by ultrasound (n = 88; rS = 0.55; p<0.001) and inversely to skin echogenicity measured by ultrasound (n = 88; rS = −0.40; p<0.001). In 70 patients followed longitudinally there was a correlation between changes in serum COMP (n = 307) and changes in mRss (rS = 0.35; p = 0.008). In individual patients monitored with repeated measurements, serum COMP changes closely paralleled changes in mRss. A C-terminal COMP fragment, with an apparent molecular mass of 56 kDa, was identified in SSc skin biopsies, while no COMP reactivity was detected in normal skin.
Conclusion: The high turnover of COMP in SSc skin suggests a pathophysiological role. Serum COMP shows promise as a new biomarker in SSc.
Statistics from Altmetric.com
One characteristic component of systemic sclerosis (SSc, or scleroderma) is the fibrosis in skin and internal organs. The fibrotic process has features of an uncontrolled wound-healing process, where transforming growth factor β (TGF-β), released by a variety of immune cells, including macrophages and T cells, or platelets at sites of vascular injury, continuously stimulate fibroblast production of extracellular matrix (ECM).1
Studies of SSc have been complicated by the heterogeneity and rareness of the condition and the difficulty of discriminating between disease activity and damage. Therefore the number of reports on effects of treatment is strikingly low. Preliminary criteria for disease activity, mainly involving either severity or deterioration of skin, vascular, cardiac, pulmonary or articular involvement as well as measurements of inflammation, have been presented although not yet fully developed.2 In addition, the different components of the disease have a discordant natural history. Skin involvement often regresses spontaneously after reaching a peak within 3 years of disease, whereas lung involvement undergoes gradual worsening, especially if untreated during the first years of disease.3–6
Fibrosis of the skin can be assessed by palpation, and its extent predicts internal organ involvement and survival.7 The established method of skin assessment is the semi-quantitative Rodnan skin score (Rss), introduced by Rodnan in 1979, which is used worldwide with variations in definitions of maximum points per anatomical site or number of sites to score.8 Despite its feasibility, the Rss has limitations, ie, in discriminating between hard, tight or thick skin, as well as rather sluggish sensitivity to change. Therefore, new biomarkers, based on increased understanding of the molecular biology in SSc are needed to evaluate strategies for treatment of fibrosis.9
Measures of ECM metabolism are offered by different markers of fibroblast activity, exemplified by type III procollagen N-terminal propeptide (PIIINP). However, this indicator is widespread to most tissues in the body.10 Other collagen metabolites, such as N-terminal and C-terminal type I procollagen peptides (PINP and PICP, respectively), and crosslinked C-terminal telopeptide of collagen I (ICTP), have been evaluated and shown some relation to skin involvement.11 Recently, PINP was shown to be associated with change in Rss in a trial with a recombinant human antibody to TGF-β 1.6
Cartilage oligomeric matrix protein (COMP, also known as thrombospondin-5) is a large disulfide-linked pentameric glycoprotein that was discovered and characterised in cartilage and subsequently in tendon.12–14 COMP is primarily produced by chondrocytes and also by tenocytes. More recently, it has been shown that COMP can also be produced by dermal and synovial fibroblasts.15 COMP has been identified as a multivalent binding partner of triple helical collagen type I and II, and enhances fibril formation of collagen in vitro, which is consistent with a model where COMP plays a role for assembly and maintenance of the fibrillar collagen extracellular network.16 17
Production of the protein in cartilage is upregulated in osteoarthritis and by cyclic mechanical load.18 19 Serum levels of COMP fragments released have been shown to reflect joint tissue turnover in osteoarthritis and rheumatoid arthritis.20–25 Stimulation of human fibroblasts with the profibrotic cytokine TGF-β leads to an upregulation of COMP transcription, suggesting COMP production to be downstream to TGF-β in fibrotic diseases.26 In a study involving skin biopsies, non-lesional cultured dermal fibroblasts from patients with early SSc displayed increased expression of the COMP gene.27 COMP has not been reported to be present in normal skin, but has been shown to be expressed in SSc skin biopsies and cultured SSc fibroblasts.28 A role for COMP in fibrosis is implied by the high levels found in the ECM in equine scar tissue.24
Based on the role of COMP in collagen fibrillogenesis, the release of COMP from cartilage into synovial fluid and serum in arthritis and the presence of COMP in SSc skin, the objective of this study was to test the hypothesis that serum COMP could be used as a biomarker for skin involvement in patients with SSc.
SUBJECTS AND METHODS
Subjects and study design
All patients in the present study were recruited from the SSc cohort in Lund and the patients in this study have been evaluated at the Department of Rheumatology on three or more occasions to enable longitudinal correlates. The cohort consists of 420 patients from the whole of Sweden, but the majority are local referrals. The disease onset was defined as the first non-Raynaud manifestation. The time of the first evaluation ranged from June 1984 to January 2002.
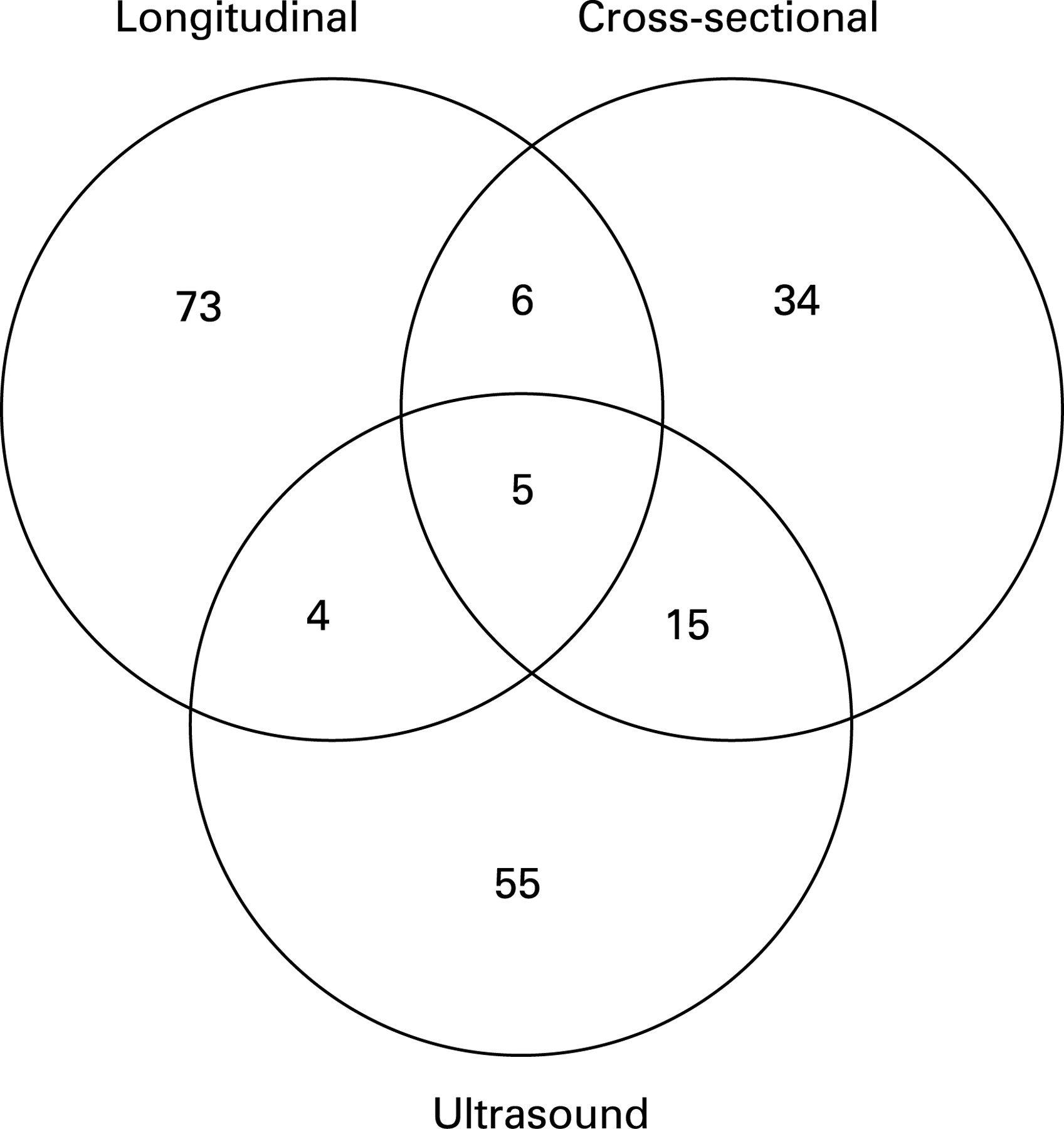
Three principal cohorts of patients with SSc were evaluated (table 1). In a cross-sectional analysis, serum COMP was correlated to mRss in patient groups, which differed regarding skin involvement. In a longitudinal study, serum COMP was correlated to mRss at different time points in two subsets of patients with SSc with mild and extensive skin involvement, respectively. To further investigate the relationship between skin involvement and serum COMP, a cross-sectional study was performed in patients with short disease duration who had undergone ultrasound examination of the skin at the same time as serum COMP and mRss were measured. Based on these three studies, eight patients with high serum COMP and one patient with clinical skin flare were identified and studied to evaluate the correlation between skin involvement and serum COMP over time. Finally, patients in the cross-sectional study with different degrees of pulmonary involvement were evaluated for possible relationship between pulmonary involvement and serum COMP. In total, 464 COMP analyses in 227 patients were performed in the 3 studies. The 227 patients in the studies were 192 unique patients with 162 patients included in only 1 study, 25 were included in 2 studies and 5 patients were included in all studies (fig 1).
Clinical features
Lung involvement was assessed by chest radiography using standard posteroanterior and lateral radiographs, and high-resolution computed tomography (HRCT) of the lungs. Vital capacity (VC) was measured with a water-filled spirometer and the diffusing capacity for carbon monoxide (DLCO) was ascertained by application of the single breath method. The gender, age, lung status and skin involvement of the patients is displayed in table 2.
All subjects met the American College of Rheumatology (ACR) criteria for SSc.30 The disease was classified as diffuse cutaneous SSc (dcSSc) or limited cutaneous SSc (lcSSc) according to the extent of skin involvement.31 Skin involvement was determined by the modified Rodnan skin score (mRSS) with palpation of 17 anatomical sites (face, fingers, hands, forearms, upper arms, chest, abdomen, thighs, legs and feet) and scoring on a 0–3 scale, where 0 = normal skin, 1 = slight thickening, 2 = moderate thickening and 3 = hidebound skin sclerosis.32 The scores for all sites were summed to give a total score, with a maximum possible score of 51. All subjects were examined by one of four doctors in the scleroderma group, trained to be concordant in the skin scoring technique.
Ultrasound
Skin thickness and skin echogenicity were measured with a high frequency ultrasound scanner (Dermascan, Cortex Technology, Denmark), in which a 20 MHz transducer was mounted. Two scans of the tissue were obtained: a 1-dimensional A mode image with different echoes defining the interfaces between epidermis, dermis and subcutis, and a 2-dimensional B mode image with different colours reflecting the differing echogenicities of the skin. The echogenicity in the dermal region was represented on an arbitrary scale (0–255 pixels) where a low value represents high water content and a high value represents low water content. By outlining a block of skin the mean echogenicity was estimated for a selected region.33 All measurements were made before noon. Five anatomical sites, selected in order to distinguish skin involvement in lcSSc and dcSSc, and to monitor disease development over time were analysed; the dorsal aspect of the interarticular portion of the proximal phalanx of the right second finger (phalanx), the area (valley) between the metacarpophalangeal joints II and III of the right hand (hand), the dorsal aspect of the right forearm 3 cm proximal of the wrist (forearm), the lateral aspect of the right leg 12 cm proximal of the ankle joint (leg), and the sternum 2 cm distal from the upper part of the manubrium (chest). The sum of skin thickness and the sum of skin echogenicity from all five anatomical regions were used to compare with serum COMP.
Serum COMP analyses
Serum samples stored in aliquots at −70°C were used for COMP analyses. Serum COMP was measured with a commercial sandwich ELISA using two monoclonal antibodies directed against separate antigenic determinants on the human COMP molecule (AnaMar Medical, Lund, Sweden). The detection limit was 0.1 U/litre and the intra- and interassay coefficient of variation was <5%.
Detection of COMP in skin biopsies
For detection of COMP, skin biopsy punches (3 or 5 mm in diameter) from forearm were frozen immediately after sample collection. Tissue samples between 10 to 15 mg wet weight were thawed on ice, briefly rinsed in Tris-buffered saline (TBS; 0.15 M NaCl, 50 mM Tris, pH 7.4) to remove blood traces and extracted over night at 4°C in 100 μl of 4 M GuHCl, 50 mM Tris pH 7.5, 150 mM NaCl containing 5 mM N-ethylmaleinimide, 20 mM EDTA, 5 mM benzamidine and 100 mM 6-aminohexanoic acid. Proteins were recovered from the supernatant by ethanol precipitation (10-fold excess of 95% ethanol containing 50 mM sodium acetate). Samples were dissolved in 4% sodium dodecyl sulfate (SDS) sample buffer, reduced with 50 mM dithiothreitol and samples representing 10–15 mg of wet weight skin were analysed by SDS-polyacrylamide gel electrophoresis (PAGE) in 4–12% gradient gels and transferred to nitrocellulose membranes using a BioRad tank (Bio-Rad, Hercules, California, USA). Membranes were briefly stained with Ponceau red (0.1% in 5% acetic acid) to check for correct transfer and protein content. After blocking over night at 4°C with 5% (w/v) skimmed milk powder in TBS-Tween (TBS-T; 50 mM Tris pH 7.5, 150 mM NaCl, 0.1% (w/v) Tween, pH 7.4), membranes were incubated with a monoclonal antibody CH 12-7 raised against the C-terminal 15 amino acids of human COMP and diluted at 1:5000 in 2% (w/v) milk powder/TBS-T at room temperature for 1.5 h. Subsequent washing with TBS-T and incubation with a horseradish peroxidase (HRP)-labelled goat anti-mouse secondary antibody (1:10000) (Jackson Immunoresearch) under the same conditions were followed by electrochemical luminescence (ECL) detection of the labelled proteins.
Statistical analyses
Differences between groups were analysed using the Mann–Whitney U test. Associations between variables were analysed using the Spearman correlation. A p value <0.05 was considered significant.
RESULTS
Serum COMP correlates with mRss
The two groups in the longitudinal study were selected to differ in the degree of skin involvement. Serum COMP was twice as high at the initial assessment in the patients who scored an mRss of 25 or higher (31 out of 35 were dcSSc) compared to patients whose mRss never exceeded 10 (all of whom were lcSSc) (p<0.01; table 2). Serum COMP correlated to mRss in the longitudinal study at the initial assessment (rS 0.60; p<0.001; fig 2A) and at all assessments (rS 0.49; p<0.001). The correlation between serum COMP and mRss was also seen in the cross-sectional study (rS 0.57; p<0.001; fig 2B) and in the ultrasound study (rS 0.51; p<0.001).

Changes in serum COMP correlate to changes in mRss
To evaluate the changes in serum COMP during follow-up, regression lines for every individual patient were calculated. The median slope for patients with mild skin involvement (mRss never >10), low-longitudinal group, was −0.10 and for the patients with extensive skin involvement (mRss at least once >25), high-longitudinal group, −0.50 (fig 3A,B).

The change in serum COMP did not follow a straight line; the largest decrease was seen during the first year of observation. To evaluate sensitivity to change during the first year, ΔCOMP and ΔmRss was calculated by subtracting the first measurement from the second (1 year later). Mean (SD) ΔCOMP in the low-longitudinal group and the high-longitudinal group were −0.024 (2.44) and −1.813 (5.35) U/litre/year respectively, whereas mean (SD) ΔmRss in the low-longitudinal group and high-longitudinal group were −0.52 (1.98) and −4.74 (8.34), respectively. There was a correlation between ΔCOMP and ΔmRss (rS 0.35; p = 0.008).
Serum COMP correlates to skin thickness and skin echogenicity as measured by ultrasound
In the 97 patients with short disease duration (mean 0.9 years) at ultrasound examination, we found that serum COMP levels correlated to the total skin thickness (rS 0.55; p<0.001), and inversely to total skin echogenicity (rS −0.40; p<0.001) calculated as the sum of the five different anatomical sites (fig 4A,B).

Serum COMP changes in individual patients correlates to changes in mRss
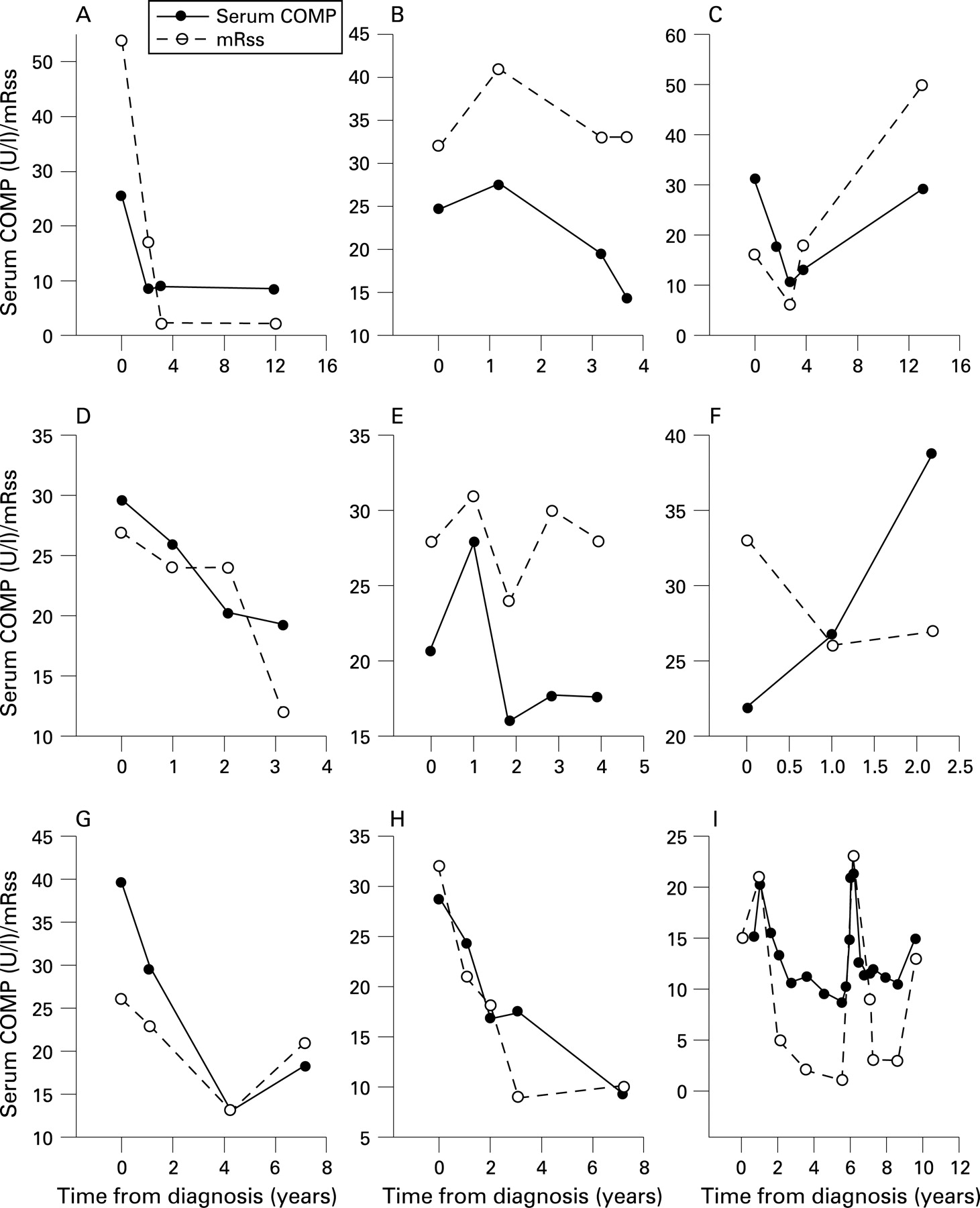
Of the 35 patients in the high-longitudinal group, 8 patients displayed very high serum COMP levels, >25 U/litre, rarely seen in osteoarthritis or inflammatory joint conditions. Figure 5A–H shows that the serum COMP levels closely paralleled mRss in all patients except one (fig 5F), who had deteriorating renal function (serum creatinine rose from 91 to 165 μmol/litre) associated with severe left heart failure secondary to aortic valve stenosis. In a patient with the unusual feature of clinically apparent skin flare serum COMP and mRss changed in parallel (fig 5I).
COMP is detected in SSc skin biopsies but not in normal skin biopsies
Protein extracts from punch biopsies of affected skin areas obtained from patients with SSc were submitted to Western blot analysis compared to normal human skin using a monoclonal antibody against the very C-terminal sequence of human COMP. In fig 6 the Ponceau red staining of normal vs SSc skin extract after blotting is shown, as well as the image of the same blot after immune reaction with the anti-C-terminal peptide antibody and ECL development. The result of two additional samples from patients with SSc submitted to the same analysis is also shown. Only in extracts from patients with SSc did we observe reactivity of a doublet protein band with apparent molecular weight of 56 kDa. The COMP molecule consists of five identical subunits of 84 kDa each. The fragment detected with the monoclonal antibody directed against the most C-terminal 15 amino acids of COMP contains the entire functional C-terminal part. Cleavage has apparently occurred in the stalk region. The mobility of the fragment was similar without reduction (data not shown) demonstrating that the cleavage reduced COMP from a pentamer to this single chain structure.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Serum COMP levels do not correlate with pulmonary involvement
The subgroups in the cross-sectional study were defined by the presence of ground glass appearance on HRCT and pulmonary fibrosis, and by the extent of skin disease. There were no differences in mean serum COMP between the subgroups (table 1) and serum COMP did not correlate to VC (rS −0.14; ns) or to DLCO (rS −0.02; ns). This was confirmed in the longitudinal study, where serum COMP did not correlate to VC (rS −0.05; ns) or DLCO (rS 0.34; ns).
DISCUSSION
This study shows a close correlation between serum levels of COMP and skin changes in SSc as measured by mRss or ultrasound strongly supporting a possible use as biomarker for disease process in the skin of patients with SSc. Thus, serum COMP levels reflect the ECM turnover and development of fibrosis in the skin.
COMP has previously been shown to be a marker for cartilage turnover in osteoarthritis and rheumatoid arthritis and it should be stressed that although the protein is most prominent in cartilage it is found in low levels in other tissues.25 However, the close correlation between the two other measures of skin involvement in SSc and serum COMP in this study makes it highly likely that a large proportion of circulating COMP in patients with SSc originates from the skin. In support of this, in a substantial number of patients serum levels of COMP were much higher than previously seen in joint diseases.25 The hypothesis of skin as the origin of circulating COMP in SSc was further supported by the demonstration of COMP in skin biopsies from patients but its absence in control skin.
It is important to stress that the method used for visualising COMP by immunoblot utilises an antibody recognising the C-terminal part of human COMP. The fragment of apparent molecular weight of 56 kDa, which was detected in the SSc biopsies, has not been previously identified in other tissues and its role in the developing pathology is unknown. Since COMP is not detected in normal skin, the molecule when expressed in SSc skin must have been synthesised as a result of as yet undefined stimuli involved in the fibrotic process. Furthermore, COMP detected in serum is unlikely to consist of the 56 kDa fragment since the monoclonal antibodies used in the serum assay are directed to more N-terminal sites, possibly not represented in the fragment found in the skin. Thus it appears that COMP is not merely laid down in the tissue but parts of it are released, ie, a turnover of the protein occurs in the pathologically deranged skin of patients with SSc. It is of interest to note that the fragment retained contains the functional part of COMP, previously shown to bind to collagens I and II, collagen IX and fibronectin.16 34 This part of the molecule also contains a stretch of amino acids identical to one in thrombospondin-1 that has been shown to bind to CD47 (IAP).35 36 This may bind to the cell receptor, modulating integrin signalling and cell phenotype. It remains to be seen whether these interactions have roles in cells organising the fibrotic tissue.
The part of the study that included a small subset of patients with lung involvement, indicated that serum COMP was not informative of changes relating to pulmonary function tests. COMP has been found in biopsies from lung tissue in SSc.37 There are several explanations for our negative findings. First, it is highly likely that the contribution to circulating COMP from affected lung tissue is too small to detect against the background of COMP released from skin, which is a much larger organ. Secondly, the methods for evaluating lung involvement, ie, VC and DLCO, may be too imprecise to estimate the burden of fibrosis in the lungs and therefore a correlation to serum COMP may not be seen. Finally, and highly speculatively, it cannot be ruled out that fragmentation and release of COMP from lungs is different than in other organs, and that fragments from the lungs are not detectable by the current COMP assay.
The need for sensitive and specific methods for diagnosis, evaluation of prognosis and monitoring therapy in SSc cannot be overemphasised.37 In this respect, the present study has shown that serum COMP should represent a valuable novel tool that should be explored in other settings to establish its role in the clinical management of patients with SSc. However, the full implications of altered serum COMP in SSc and during treatment need to be further investigated. At this stage it seems established that serum COMP closely relates to skin involvement in the disease and apparently depicting molecular events pertinent to the fibrosis. It is possible that serum COMP can be used as a marker for response to therapeutic interventions in early phases of drug trials and in the clinic. Since a biomarker is expected to react much faster to an intervention than mRss, trials for proof of principle may be facilitated by the use of serum COMP in early stages of drug development. The prognostic and diagnostic utility of serum COMP should be evaluated in further studies including combinations of other biomarkers, eg, to reflect collagen turnover.
Acknowledgments
Skilful technical assistance by Mrs Mette Lindell is appreciated. AnaMar Medical provided the kit for COMP-assay. We thank professor Frank Wollheim for insightful comments during the writing of this article.
REFERENCES
Footnotes
RH and AK contributed equally to the study.
Funding: This study was supported by grants from the Swedish Medical Research Council, the Medical Faculty of Lund University, the Swedish Rheumatism Association, King Gustaf V 80-year Fund, the Österlund Foundation, the Kock Foundation and the European Community’s FP6 funding (AUTOCURE project) and the Anna-Greta Crafoord stiftelse (AK).
Competing interests: DH and TS are cofounders and minor shareholders of AnaMar Medical, Lund, Sweden. This publication only reflects the author’s views. The European Community is not liable for any use that may be made of the information herein.
Ethics approval: The study was approved by the regional ethics board.